0684
Accelerated abdominal 4D flow MRI using 3D golden-angle cones trajectory1Electrical Engineering, Stanford University, Stanford, CA, United States, 2Radiology, Stanford University, Stanford, CA, United States, 3Applied Sciences Laboratory, GE Healthcare, San Diego, CA, United States
Synopsis
4D flow MRI enables comprehensive abdominal evaluation, but long acquisition times and motion corruption limit its clinical applicability. To address these limitations, we present a 4D flow sequence with a 3D golden-angle reordered cones sampling trajectory. Cones has high sampling efficiency to allow for vastly accelerated scan times, and excellent aliasing properties that diffuse respiratory and bowel motion artifacts. To further improve motion-robustness, respiratory signals are estimated from each cone readout, and then used to suppress motion during reconstruction. We show that these techniques can be combined to achieve high quality abdominal 4D flow renderings in under 5 minutes.
Purpose
Cartesian 4D flow MRI enables simultaneous assessment of cardiovascular anatomy and flow, but long acquisition times limit its clinical use in the abdomen. Further, long scan times allow respiratory and bowel motion to impair anatomical visualization and flow quantification accuracy. We propose to acquire data along efficient non-Cartesian trajectories to reduce scan time and diffuse motion artifacts across more dimensions. Both 3D radial projection1,2,3 and stack-of-spirals4 imaging have previously been applied to 4D flow, each with their own unique advantages. The 3D cones trajectory5,6 combines advantages of both by acquiring samples along twisting paths that lie on conical surfaces. Like stack-of-spirals, it has high sampling efficiency, and like 3D radial, it exhibits excellent motion aliasing properties while maintaining short echo times to reduce flow-induced errors. In this work, we develop a 4D flow sequence that acquires k-space data along a 3D golden-angle reordered cones sampling trajectory and develop a soft-gated image reconstruction that leverages self navigation data. We assess resulting image quality, including motion artifacts, in abdominal scans.Methods
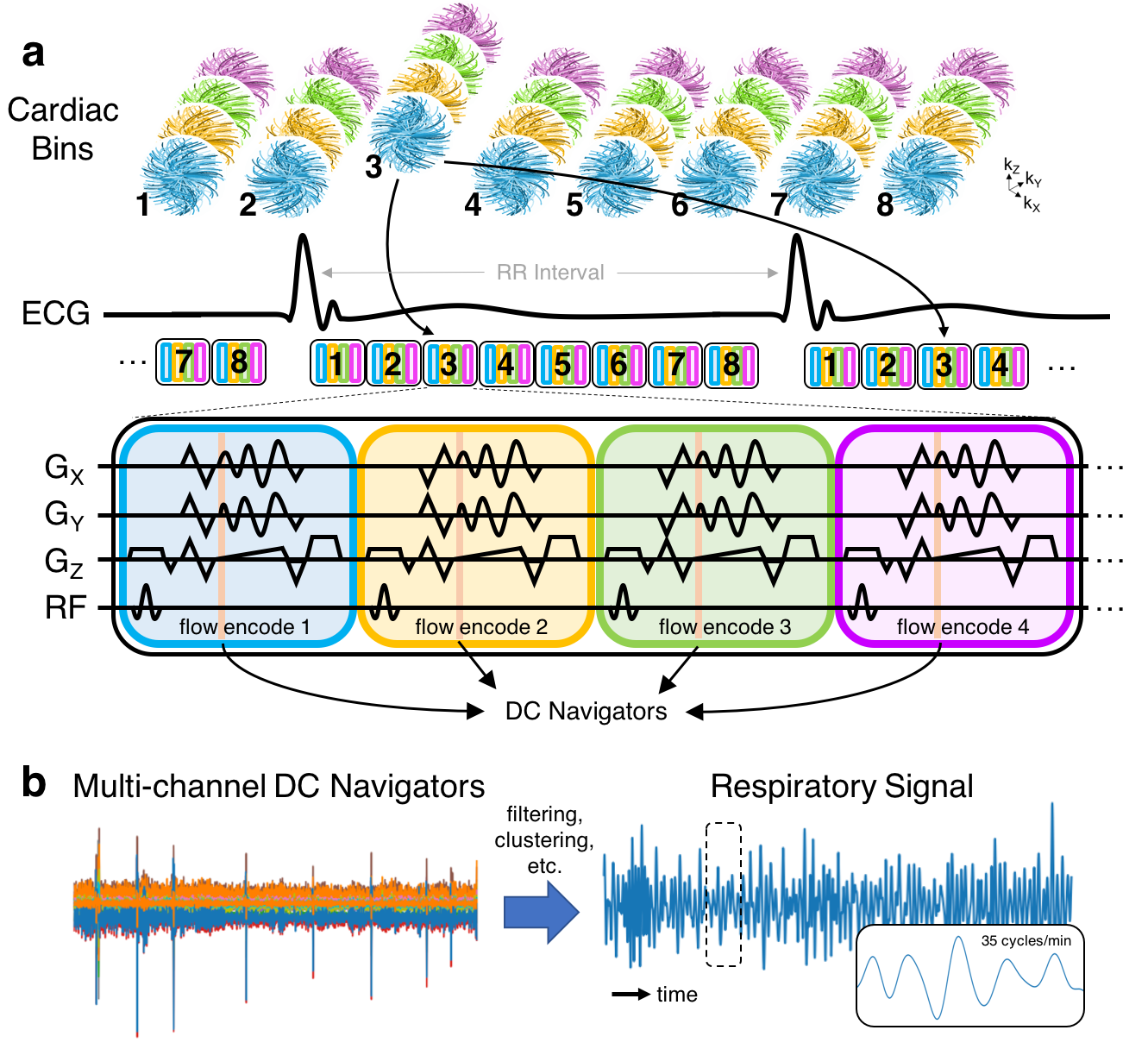
Trajectory design and pulse sequence: Gradient waveforms are iteratively designed on-the-fly as described by Gurney et al5. Cone interleaves are permuted by the 2D golden-means algorithm7 to enable arbitrary temporal resolution, and enhance motion-robustness (Figure 1a). The pulse sequence is based on RF-spoiled gradient recalled echo (SPGR) with a simple 4-point interleaved velocity encoding scheme (Figure 2).
Image reconstruction: All datasets are reconstructed in BART8 using l1-ESPIRiT9 with spatial wavelet and temporal total variation regularization. Due to memory limitations, data required coil compression from 32 to 16 channels using the singular value decomposition. A low pass filter (cutoff at 0.67 Hz) is applied to a DC navigator10 to estimate respiratory motion signals from each coil element (Figure 1b). The dominant signal is chosen by a coil clustering algorithm11. Motion estimates are used during reconstruction to suppress respiratory motion artifacts by assigning lower weights to motion-corrupted readouts in the data consistency term (soft-gating)12.
Experiments: With informed consent and IRB approval, subjects referred for contrast-enhanced abdominal MRI were scanned using the cones 4D flow sequences on a 3T scanner (GE MR750, Waukesha, WI) with a 32-channel cardiac coil. All data was acquired with subjects freely breathing. Cones 4D flow scan parameters include flip angle: 15o, readout bandwidth: +/- 250 kHz, readout duration: 0.9 ms, TE: 0.9-1.1 ms, TR: 3.9-4.1 ms, spatial resolution: 1.0x1.0x1.5 mm3, matrix size: 256x256x120, 8 cardiac phases, venc: 100-150 cm/s, and scan durations: 4-7 minutes. One subject was also scanned with radially view-ordered Cartesian 4D flow13 for comparison. Cartesian acquisition and reconstruction parameters were kept the same as cones except for readout bandwidth: +/- 125 kHz, TE: 2.2 ms, and TR: 6.3 ms.
Results
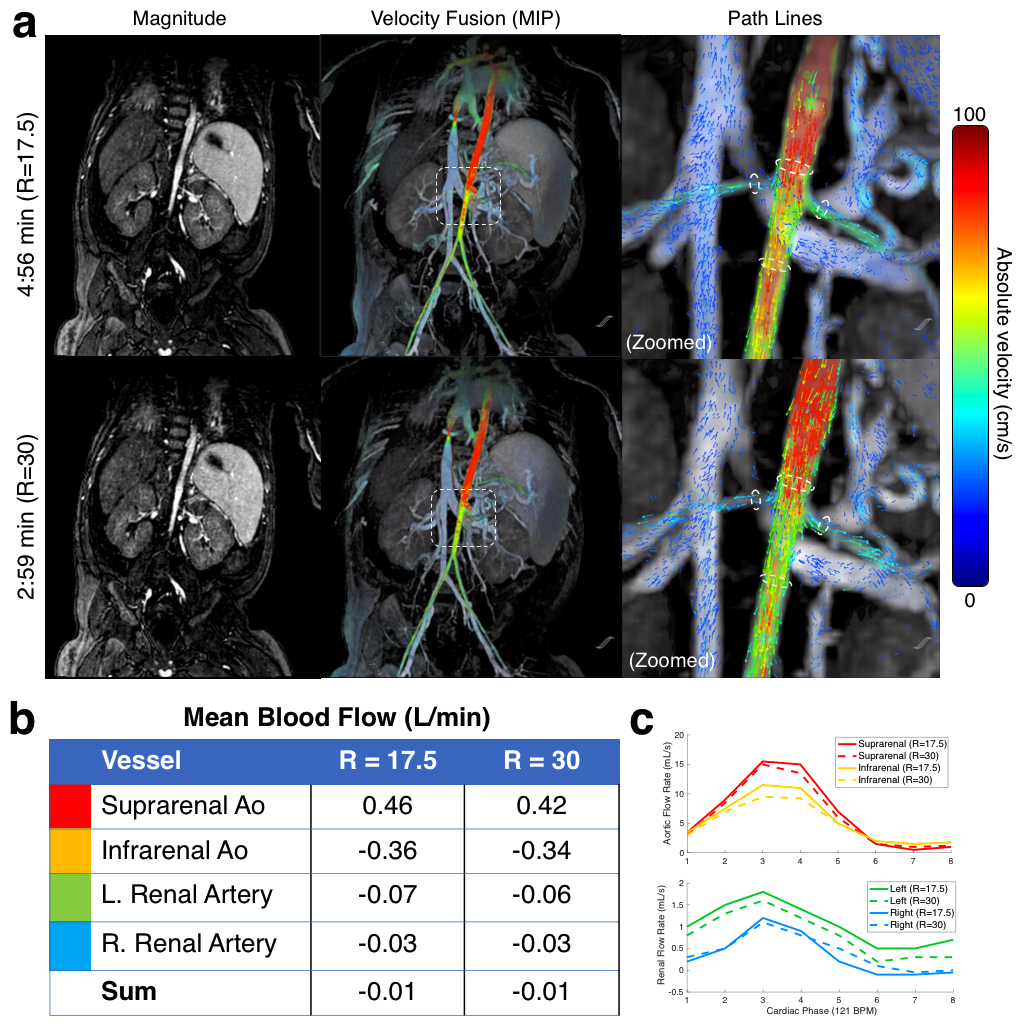
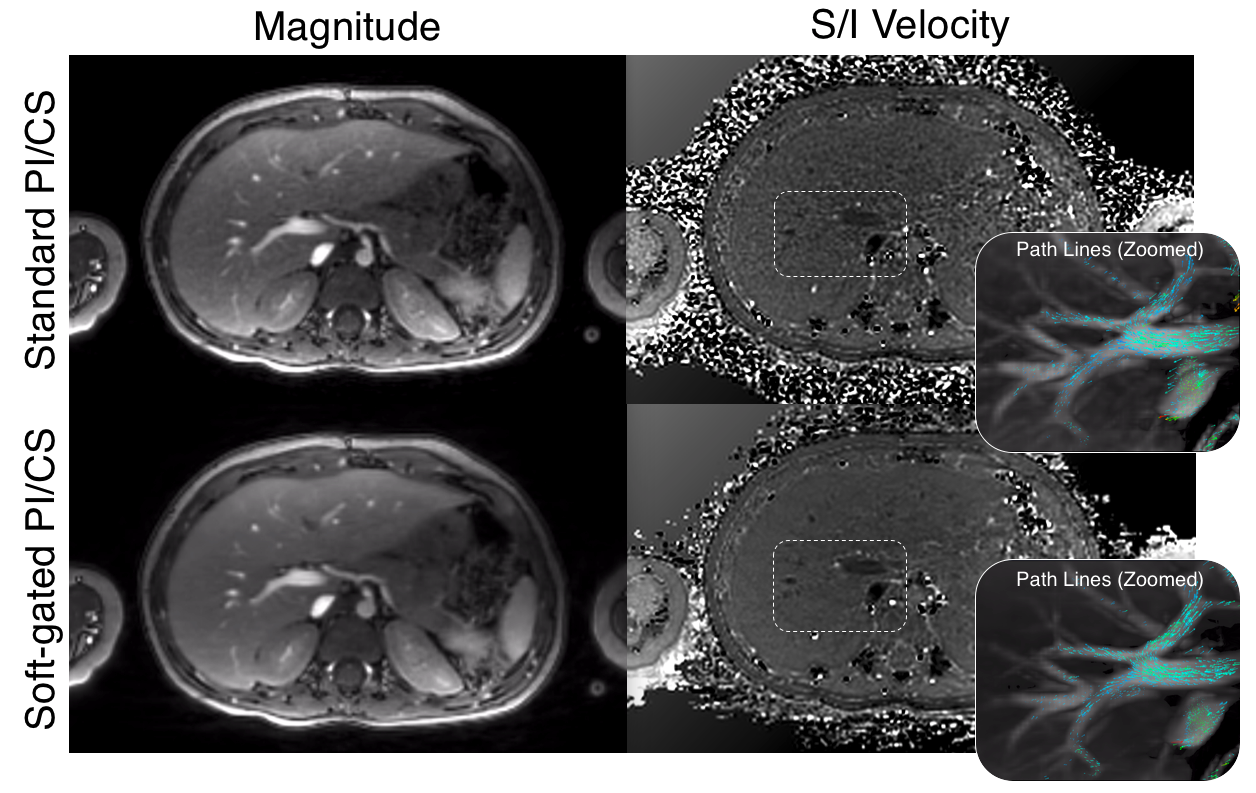
Cones 4D flow provides excellent delineation of abdominal vasculature in scan times as short as 3 minutes (Figure 3a). Aortic and renal arterial blood flow are measured and shown to be conserved (Figures 3b,c). By nature of the cones sampling trajectory, both motion and aliasing artifacts appear noise-like and incoherent. Soft-gating reconstructions suppress noise-like motion artifacts, and can improve image quality in both magnitude and velocity images (Figure 4). Compared to the Cartesian acquisition/reconstruction, cones velocities and scan time were similar, but with reduced flow and motion artifacts (Figure 5).Discussion
We introduce the first 4D flow sequence with a cones sampling trajectory. Higher k-space sampling efficiency allows scan time acceleration rates of up to R=30 without significant loss of image quality or change in velocity quantification. Due to desirable aliasing properties and soft-gating, motion artifacts are reduced in the cones reconstructions when compared against Cartesian.
Similar to findings with PC-VIPR1, cones 4D flow underestimates peak flows relative to those estimated by Cartesian (Figure 5), although a more rigorous evaluation is necessary. Since readout begins shortly after flow encoding, short-term eddy current effects during DC acquisition induce larger phase errors in velocity maps than in Cartesian 4D flow. These effects were corrected after careful tuning of the phase correction. As with any non-Cartesian trajectory, cones is also sensitive to off-resonance artifacts, particularly from fat, and may require fat saturation in certain patients.
This initial implementation yielded a reasonable scan time and spatiotemporal resolution for venous imaging. For arterial applications, cones 4D flow acquisitions may require further acceleration by increasing the sampling efficiency via extended readouts with more twisting. However, further study is required to determine the resulting impact on both flow quantification and off-resonance blurring.
Conclusion
Here, we show that the 3D cones sampling trajectory can highly accelerate 4D flow acquisitions and reduce both flow and motion artifacts.Acknowledgements
NIH R01 EB009690, National Science Foundation Graduate Research Fellowship (DGE-114747), and GE HealthcareReferences
[1] Gu T, Korosec FR, Block WF, Fain SB, Turk Q, Lum D, Zhou Y, Grist TM, Haughton V, Mistretta CA. PC VIPR: a high-speed 3D phase-contrast method for flow quantification and high-resolution angiography. Am J Neuroradiol. 2005;26(4):743-9.
[2] Frydrychowicz A, Landgraf BR, Niespodzany E, Verma RW, Roldán-Alzate A, Johnson KM, Wieben O, Reeder SB. Four-dimensional velocity mapping of the hepatic and splanchnic vasculature with radial sampling at 3 tesla: a feasibility study in portal hypertension. J Magn Reson Imaging. 2011;34(3):577-84.
[3] Motoyama D, Ishii Y, Takehara Y, Sugiyama M, Yang W, Nasu H, Ushio T, Hirose Y, Ohishi N, Wakayama T, Kabasawa H, Johnson KM, Wieben O, Sakahara H, Ozono S. Four-dimensional phase-contrast vastly undersampled isotropic projection reconstruction (4D PC-VIPR) MR evaluation of the renal arteries in transplant recipients: Preliminary results. J Magn Reson Imaging. 2017;46(2):595-603.
[4] Sigfridsson A, Petersson S, Carlhall CJ, Ebbers T. Four-dimensional flow MRI using spiral acquisition. Magn Reson Med. 2012;68(4):1065-73.
[5] Gurney PT, Hargreaves BA, Nishimura DG. Design and analysis of a practical 3D cones trajectory. Magn Reson Med. 2006;55(3):575-82.
[6] Zucker EJ, Cheng JY, Haldipur A, Carl M, Vasanawala SS. Free-breathing pediatric chest MRI: Performance of self-navigated golden-angle ordered conical ultrashort echo time acquisition. J Magn Reson Imaging. 2017. Pre-print.
[7] Chan RW, Ramsay EA, Cunningham CH, Plewes DB. Temporal stability of adaptive 3D radial MRI using multidimensional golden means. Magn Reson Med. 2009;61(2):354-63.
[8] Uecker M, Ong F, Tamir JI, Bahri D, Virtue P, Cheng JY, Zhang T, Lustig M. Berkeley advanced reconstruction toolbox. ISMRM 2015. Toronto, Ontario, Canada.
[9] Uecker M, Lai P, Murphy MJ, Virtue P, Elad M, Pauly JM, Vasanawala SS, Lustig M. ESPIRIT – An eigenvalue approach to autocalibrating parallel MRI: Where SENSE meets GRAPPA. Magn Reson Med. 2014;71(3):990-1001.
[10] Larson AC, White RD, Laub G, McVeigh ER, Li D, Simonetti OP. Self-gated cardiac cine MRI. Magn Reson Med. 2004;51(1):93-102.
[11] Zhang T, Cheng JY, Chen Y, Nishimura DG, Pauly JM, Vasanawala SS. Robust self-navigated body MRI using dense coil arrays. Magn Reson Med 2016;76:197-205.
[12] Johnson KM, Block WF, Reeder SB, Samsonov A. Improved least squares MR image reconstruction using estimates of k-space data consistency. Magn Reson Med. 2012;67(7):1600-8.
[13] Cheng JY, Hanneman K, Zhang T, Alley MT, Lai P, Tamir JI, Uecker M, Pauly JM, Lustig M, Vasanawala SS. Comprehensive motion-compensated highly accelerated 4D flow MRI with ferumoxytol enhancement for pediatric congenital heart disease. J Magn Reson Imaging. 2016;43(6):1355-68.
Figures