0675
Cardiac Magnetic Resonance Fingerprinting in Heart Transplant Recipients1University Hospital (CHUV) / University of Lausanne (UNIL), Lausanne, Switzerland, 2Biomedical Engineering, Case Western Reserve University, Cleveland, OH, United States, 3Centre for BioMedical Imaging (CIBM), Lausanne, Switzerland
Synopsis
Cardiac MRF (cMRF) has recently emerged as a method of rapidly characterizing myocardial tissue. It has been shown to be robust to different and varying heart rates with high reproducibility in T1 and T2 regardless of the length and regularity of the cardiac cycle. While these techniques have been validated in healthy volunteers, patient studies have yet to be performed. Therefore, in this abstract, we present the first use of cMRF in a patient population - heart transplant recipients - and show initial results.
Introduction
Cardiac MRF (cMRF) has recently emerged as a method of rapidly characterizing myocardial tissue. It has been shown to be robust to different and varying heart rates (1) with high reproducibility in T1 and T2 regardless of the length and regularity of the cardiac cycle. While these techniques have been validated in healthy volunteers, patient studies have yet to be performed. Therefore we present the first use of cMRF in a patient population - heart transplant recipients - and show initial results.
In heart transplant patients, cardiac health is routinely diagnosed by histological assessment of endomyocardial biopsies, which can detect inflammation, fibrosis, and the associated myocyte damage (2). However, biopsy is invasive and localized to the apico-septal region of the heart, which results in low sensitivity and makes ongoing monitoring of rejection challenging. A more desirable approach would be to diagnose and characterize graft health non-invasively, such as with cardiac MRI. Myocardial T1 has been shown to correlate with fibrosis (3), whereas T2 correlates with edema, a hallmark sign of graft rejection. Some initial work has demonstrated the utility of cardiac MRI for transplant patients (4,5), though existing protocols are lengthy and still under development. Additionally, traditional cardiac parameter mapping techniques are sensitive to heart-rate variability and can suffer from low inter-scan reproducibility. Therefore, cMRF may provide a robust, easily repeatable, and non-invasive alternative for providing quantitative information about transplanted heart health.
Methods
Heart transplant
recipients (n=13, age=53.1±13.7) and healthy controls (n=5, age=32.6±6.3) were recruited for this IRB-approved study. Endomyocardial biopsy was performed in all patients and acted as the gold standard measure of graft rejection. Both patients and controls were scanned with an ECG-triggered cMRF sequence (1) using a
48-fold undersampled spiral readout (NUFFT gridded), a 192x192
matrix, and a 300x300mm2 FoV on a 3T clinical scanner (MAGNETOM
Prisma, Siemens). Short-axis basal and medial slices were each acquired during a single-breathhold scan of 15 heartbeats, with 50 TRs/heartbeat. Flip
angles varied between 4-25° with a 5.1ms TR. Five magnetization
preparation modules were alternated prior to each heartbeat (Inversion Recovery=21ms,
No Preparation, TE-T2-Prep=30,50,80ms). For each subject, an MRF
dictionary was simulated incorporating the scan-specific heart rate
timings of each acquisition, and dot-product matching (6) was used to reconstruct T1, T2, and M0 maps. The mean
myocardial T1 and T2 were then recorded for each slice.
In patients, this was repeated both pre- and post-contrast, though controls did not receive contrast injections. Commercial T1 and T2 mapping sequences (Myomaps, Siemens), based on MOLLI and T2-Prepared bSSFP, were also used pre-contrast (and post-contrast for T1 mapping). Pearson correlations between cMRF and Myomap were established, and
Bland-Altman plots were generated to determine agreement between the sequences.
An unpaired Student's t-test was also used to compare mean parameter measurements in both patients and controls.
Results
Cardiac MRF images
were successfully acquired in all subjects. From a single
breathhold, it was possible to reconstruct T1, T2, and M0 maps from a
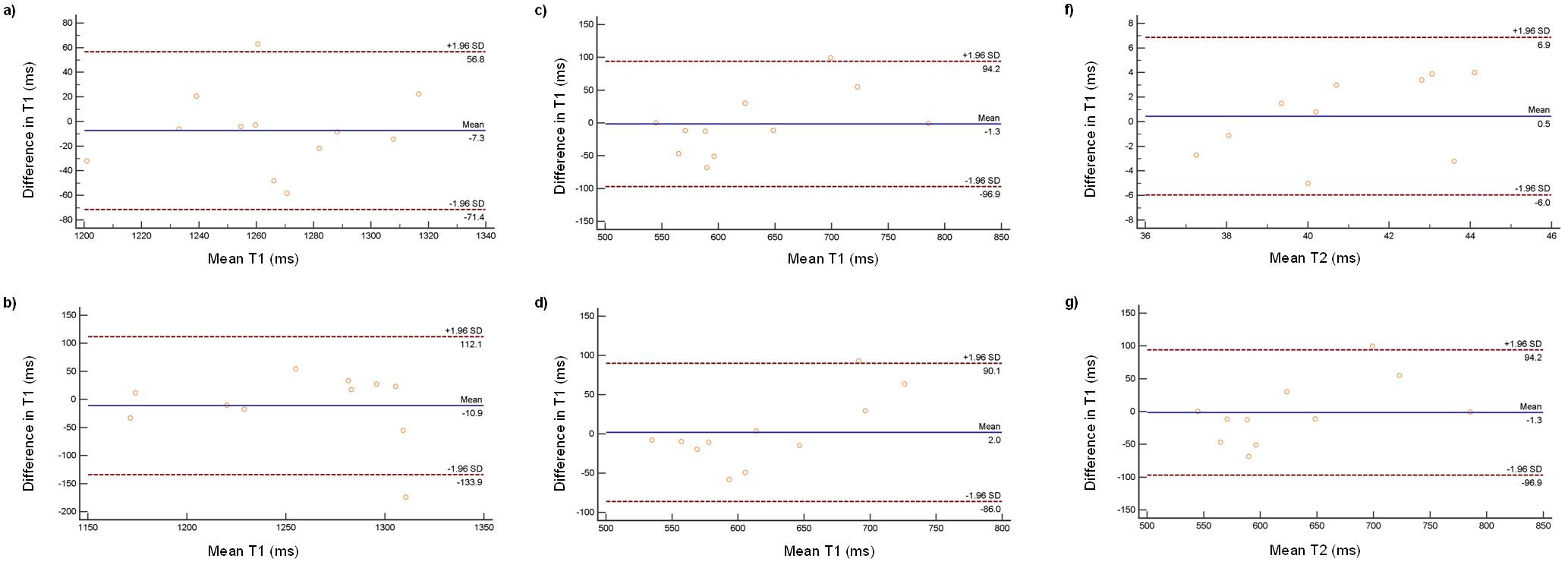
short-axis slice acquisition (Figure 1). Whole slice T1 measurements correlated well between cMRF and Myomap (pre-contrast: basal r=0.59, medial r=0.47; post contrast:
basal r=0.87, medial r=0.86, and Bland-Altman analysis also
demonstrated good agreement [pre-contrast:
basal mean=-7.3ms (CI=±64.1ms), medial mean=-10.9ms (CI=±123ms); post
contrast: basal mean=-1.3ms (CI=±95.6ms), medial mean=2.0ms (CI=±88.1ms )]. Likewise, T2 measurements showed both good correlation (pre-contrast: basal r=0.40, medial r=0.73) and good Bland-Altman agreement [pre-contrast:
basal mean=0.5ms (CI=±6.5ms), medial mean =1.9ms (CI=±6.9ms)]. T1 and T2 values were lower in controls than patients (Table 1), though this was not statistically significant in all cases.
In this study, histology indicated no graft rejection in any of the 13 patients. The range of myocardial T2 values measured by cMRF (basal: 33.3-46.1ms; medial: 34.4-50.8ms) were nonetheless consistent with those previously reported in non-rejecting heart transplant recipients (3), demonstrating agreement with previous studies, and providing a range of myocardial T1 and T2 values for cMRF in non-rejecting heart transplants.
Discussion & Conclusion
This study shows the first use of cMRF in patients and demonstrates its feasibility in scanning heart transplant recipients. In a single breathhold, it was possible to obtain T1, T2, and M0 maps, as compared to a routine clinical mapping technique (Myomap), which only yielded a single parameter per breathhold (e.g. T1). Additionally, a range of cMRF-measured T1 and T2 values were measured for non-rejecting heart transplant recipients, which differed from those of healthy controls, providing a potential baseline for future comparisons to actual rejection. Interestingly, and perhaps due to motion correction or other filters, standard deviation in T2 across patients was notably higher with cMRF than Myomap. Nonetheless, this work demonstrates the potential of cMRF to increase the available diagnostic information provided by MRI when ongoing monitoring of cardiac health is paramount.
Acknowledgements
This work was in part supported by the Swiss National Science Foundation grants #320030_143923, #326030_150828, #PZ00P3_154719, and #P2LAP3_164909; NIH grants R01HL094557 and R01DK098503; and Siemens Medical Solutions.Additional support was provided in part by the Centre d’Imagerie BioMedical (CIBM) of the UNIL, EPFL, UNIGE, CHUV, and HUG, as well as the Jeantet and Leenaards Foundations. We would also like to thank Dr. Jessica Bastiaansen for her aid with data collection.
References
1. Hamilton et al, Mag Res Med 77.
2. From et al, Mayo Clinic Proc. 86.
3. Ambale-Venkatesh et al, Nature Rev. Cardio. 12.
4. Van Heeswijk et al, JCMR 2014;16(S1):M11.
5. Butler et al, J. Heart & Lung Trans 34.
6. Ma et al, Nature 495.
Figures
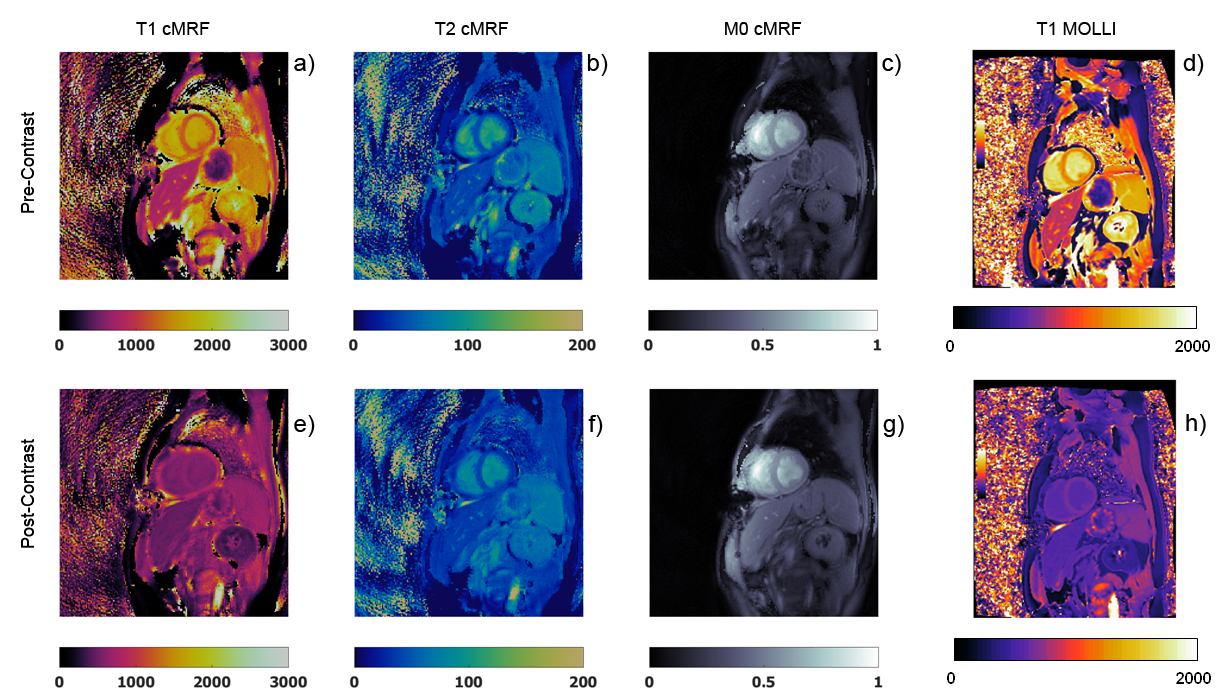
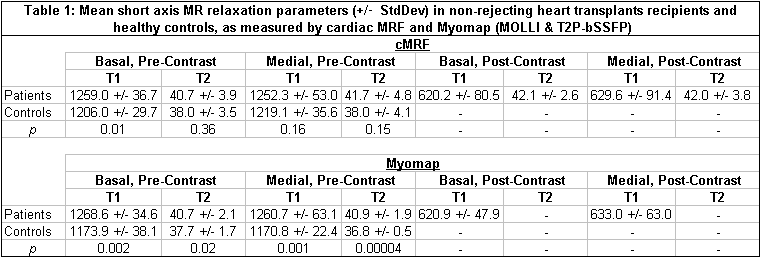
Table 1: Mean short axis MR relaxation parameters (+/- StdDev) in non-rejecting heart transplants recipients and healthy controls, as measured by cardiac MRF and Myomap (MOLLI & T2-Prepared bSSFP).