0597
Association between Tremor Severity Improvement and Functional Connectivity Changes after Magnetic Resonance Guided Focused Ultrasonic Thalamotomy Treatment in Essential Tremor Patients1Department of Diagnostic Radiology & Nuclear Medicine, University of Maryland Baltimore, Baltimore, MD, United States, 2Department of Neurosurgery, University of Maryland Baltimore, Baltimore, MD, United States, 3Department of Neurology, University of Maryland Baltimore, Baltimore, MD, United States
Synopsis
Essential tremor (ET) is the most common movement disorder and often characterized by a slowly progressive involuntary posture and/or kinetic tremor, usually affecting both upper extremities. Ablation of the ventral intermediate nucleus (VIM) of the thalamus with MRgFUS is an effective and FDA-approved treatment for medication refractory ET patients. However, very little is known regarding brain functional changes before and after the treatment and even less about its association with the tremor severity changes after treatment. This study aimed at investigating the longitudinal tremor improvement and its association with the changes of Functional connectivity of left VIM at 1-year post-treatment.
Purpose
Essential tremor (ET) is the most common movement disorder and manifests as a slowly progressive involuntary posture and/or kinetic tremor, usually affecting both upper extremities. Recently FDA approved MRguided focused ultrasonic (MRgFUS) thalamotomy as an effective neurosurgical treatment for medication refractory ET patients. It targets the ventral intermediate nucleus (VIM) of the thalamus, which contains nerve cells causing tremor, usually on only one side of the brain. A randomized trial of MRgFUS thalamotomy in ET patients showed significant tremor improvement during the 12month study period after treatment [1]. However, very little is known regarding brain functional changes and even less is known about its association with the tremor severity changes after treatment. The disruption of functional connectivity (FC) especially in the cerebellothalamo-cortical circuit has been shown to contribute to the tremor in ET patients [2, 3]. Our previous study also showed that altered FC of the targeted VIM immediately post treatment [4]. In this study, we aimed at investigating the longitudinal tremor improvement and its association with the changes of FC of the left VIM at 1-year post-treatment.Materials and Methods
Twenty medication refractory ET patients were recruited to undergo unilateral MRgFUS thalamotomy. Each patient obtained thermal ablation at the VIM contralateral to the dominant hand. Tremor severity was assessed using Clinical Rating Scale for Tremor (CRST) before and 1, 3, 6 and 12 months post treatment. An upper extremity tremor (UE-Tremor) subscore was defined as the sum of items in CRST Part A and B applicable to upper extremity and hand. Higher score indicates more severe of tremor. MRI was performed on a 3T Trio-Tim Siemens Scanner at pre-treatment, 24-hour and 1-year post-treatment. The rs-fMRI data was acquired using T2*-weighted EPI sequence with TR/TE of 3000/30ms and total 200 volumes. High resolution T1-MPRAGE images were obtained with TR/TE of 2300/2.91ms. Only 15 out of the total 20 patients (age: 72.85±5.38, 1Female/14Male, right-handed, left VIM treated) who completed CRST assessment and rs-fMRI scans at all the time points were used.
The rs-fMRI data were preprocessed with SPM12 standard procedures and smoothed 6mm FWHM Gaussian Kernel and filtered with 0.008-0.1 Hz. Nuisance variables (six motion parameters and BOLD signals from WM and CSF) were regressed out. A 6mm spherical seed was placed on the left VIM with coordinates estimated from the normalized T1-MPRAGE images at 24-hour post-treatment. Seed-to-whole brain FC analysis was performed using the CONN toolbox to obtain the FC map. At the second level, the association map between the FC changes of left VIM (post-pre) and contralateral UE-tremor reduction (pre-post) was estimated with age as a covariate using a threshold of voxel-wise uncorrected p-value of 0.009 and cluster-wise FDR-corrected p value of 0.05 for multiple comparison. Using the significant clusters thus obtained, we calculated the FC between the left VIM and these clusters. The FC was then Fish-Z transformed and their association with the contralateral UE-tremor reduction was also assessed.
Results
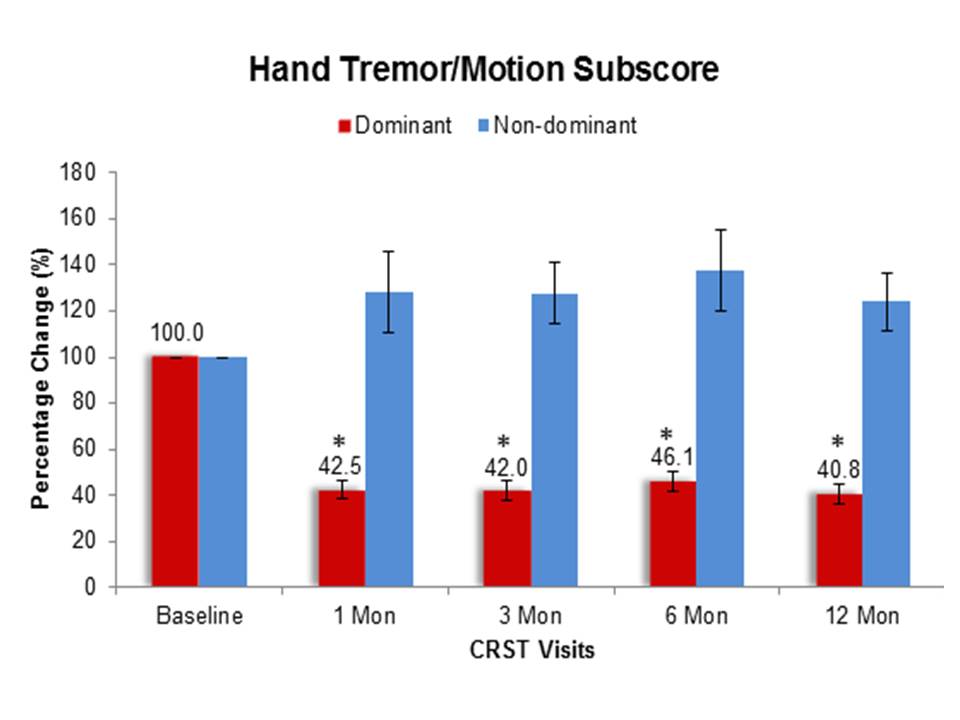
A repeated measure ANOVA was applied to determine if the UE-tremor changed significantly following the treatment. As shown in Fig. 1, the percentage change of dominant UE-tremor significantly reduced from baseline to 42.5% (p < 0.0001) at 1-month post-treatment and this reduction persisted throughout the 12-month study period. However, although non-significant, the non-dominant UE-tremor increased slightly and remained at an elevated level over one year of observation. Given non-significant findings on the non-dominant UE-tremor we focused our connectivity analysis to the dominant hand.
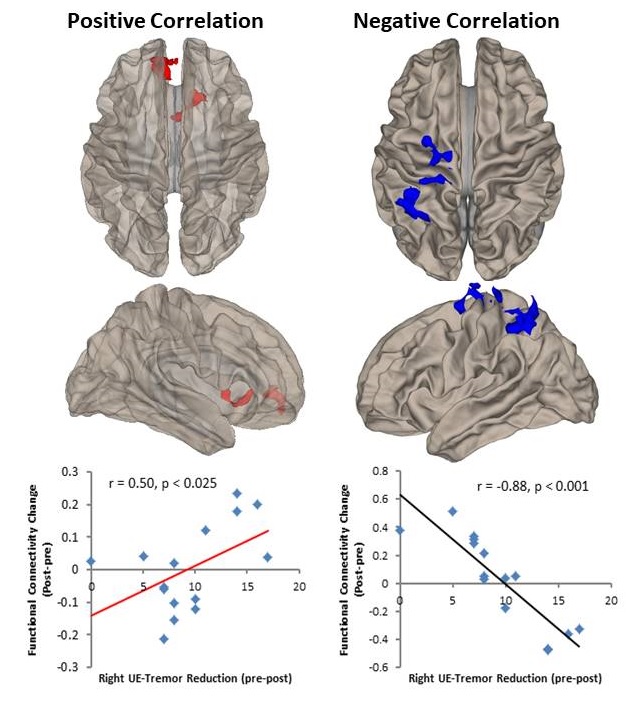
Fig.2 shows the correlation maps between the changes of FC of left VIM (post-pre) and the difference of dominant UE-tremor (pre-post). Increased FC (r=0.50, p<0.025) was associated with greater tremor reduction in ipsilateral paracingulate gyrus, medial frontal cortex, anterior cingulate cortex, contralateral caudate, and subcallosal regions indicating greater connectivity involving executive and motor, and emotional function. Whereas a reduction in FC (r = -0.88, p<0.001) associated with greater tremor reduction was found in the ipsilateral superior parietal lobule, supramarginal gyrus, superior occipital cortex, precentral gyrus and postcentral gyrus suggesting alterations in the visuomotor and visual-spatial function.
Discussion and Conclusion
In this study, for the first time we examined the FC changes in the brain and its association with longitudinal change of tremor severity for treated and non-treated side of the upper extremity separately. We observed that the unilateral VIM lesioning improved tremor symptoms only on the side of the body and the effect occurred immediately after the treatment and lasted for at least 1 year. Our results also demonstrate significant connectivity changes between the VIM of the treated side to other cortical and sub-cortical regions involving motor, visual, and emotion and their association with the changes in tremor symptoms.Acknowledgements
No acknowledgement found.References
1. Elias WJ, et al. A Randomized Trial of Focused Ultrasound Thalamotomy for Essential Tremor. N Engl J Med. 2016. 375(8):730-9.
2. Julian Benito-Leon, Elan D. Louis et al. Altered functional connectivity in essential tremor a resting-state fMRI study. Medicine. 2015. 95: 49
3. Weidong Fang, et al. Essential tremor is associated with disruption of functional connectivity in the ventral intermediate nucleus-motor cortex – cerebellum circuit. Human Brain Mapping. 2016. 37: 165-178
4. Jiang L., et al., Altered Functional Connectivity in Essential Tremor Patients immediately following Thalamotomy using MRI guided Focused Ultrasound, ISMRM 25th Annual Meeting, 2017, Honolulu, Hi, USA
Figures