0566
MR Imaging Biomarkers of Cardiac Function and Rotational Mechanics in Boys with Duchenne Muscular Dystrophy1Department of Bioengineering, University of California, Los Angeles, CA, United States, 2Department of Radiology, University of California, Los Angeles, CA, United States, 3Department of Medicine (Cardiology), University of California, Los Angeles, CA, United States, 4Department of Internal Medicine/Division of Cardiovascular Medicine, The Ohio State University, Columbus, OH, United States, 5Dorothy M. Davis Heart and Lung Research Institute, The Ohio State University, Columbus, OH, United States
Synopsis
Duchenne Muscular Dystrophy (DMD) severely impacts heart health. Decreasing LV ejection fraction (EF) is a late and highly variable outcome in this cohort. Earlier indications of cardiac involvement would improve patient management and provide insight into the utility of emerging therapy. Boys with DMD (N=25) and healthy volunteers (N=8) underwent cardiac MRI exams including short-axis tagged images. EF, peak LV twist, and peak mid-wall circumferential strain (Ecc) were estimated. Ecc and twist were significantly reduced in patients (9.3°±4.3° vs. 14.8°±3.6°, p< 0.004) and (-15.8±5.8% vs. -18.5±3.2%, p<0.02). Whereas, EF was not significantly different between groups. ~50% of DMD patients with normal EF had reduced twist and Ecc. Reduced peak LV twist and mid-wall Ecc measured by MR tagging may be earlier and more sensitive indicators of cardiac involvement in boys with DMD.
Background
Duchenne Muscular Dystrophy (DMD) is a fatal genetic disorder affecting 1 in 3000 boys. DMD severely impacts heart health, which has prompted recent clinical trials to include cardiac MRI biomarkers as end-points. Ejection fraction (EF) has been shown to decline ~2%/year, but is a late outcome and highly variable1. Identifying earlier indications of cardiac disease in this cohort may allow for more effective patient treatment and earlier insight to the utility of emerging therapies. Recent reports have indicated that peak mid-wall circumferential strain (Ecc) and LV twist are reduced in boys with DMD compared to healthy volunteers2-3. This work further characterizes both peak mid-wall Ecc and LV twist in a cohort of boys with DMD compared with healthy volunteers. The objective was to determine if reductions in peak mid-wall Ecc and LV twist can more sensitively distinguish cardiac dysfunction in this cohort compared to EF.Methods
Study Population: In this IRB-approved and HIPAA-compliant prospective study, boys with DMD (N=25, age=14±5 years) and healthy volunteers (N=8, age=17±5 years) underwent a cardiac MRI examination after receiving informed consent.
MRI Protocol: Subjects were imaged at either 1.5T or 3T (Siemens Avanto/Skyra) using: 2D CINE images (1.4x1.4x6mm, TE/TRes=1.2/45.1 ms) and basal, mid, and apical LV short-axis tagged images (1.4x 1.4x8mm, TE/TRes=2.12/24-48 ms, 11-31 phases, tag spacing=8mm). Five DMD patients received a follow-up examination 12±5 months after the initial scan.
Data Processing and Statistical Analysis: LV Ejection Fraction (EF) was quantified from CINE images (Qmass, Medis; Argus, Siemens; and Circle CVI42, Circle Cardiovascular Imaging). Peak mid-wall Ecc and peak LV twist were estimated from tagged MR images (Diagnosoft, Myocardial Solutions). Normally distributed data were compared with a two-tailed t-test. Non-parametric data were compared with a Kruskal-Wallice test. A Holm-Sidak post hoc correction accounted for multiple comparisons. Effect size (Cohen’s d) was computed to determine the non-overlap of statistically significant results.
Results
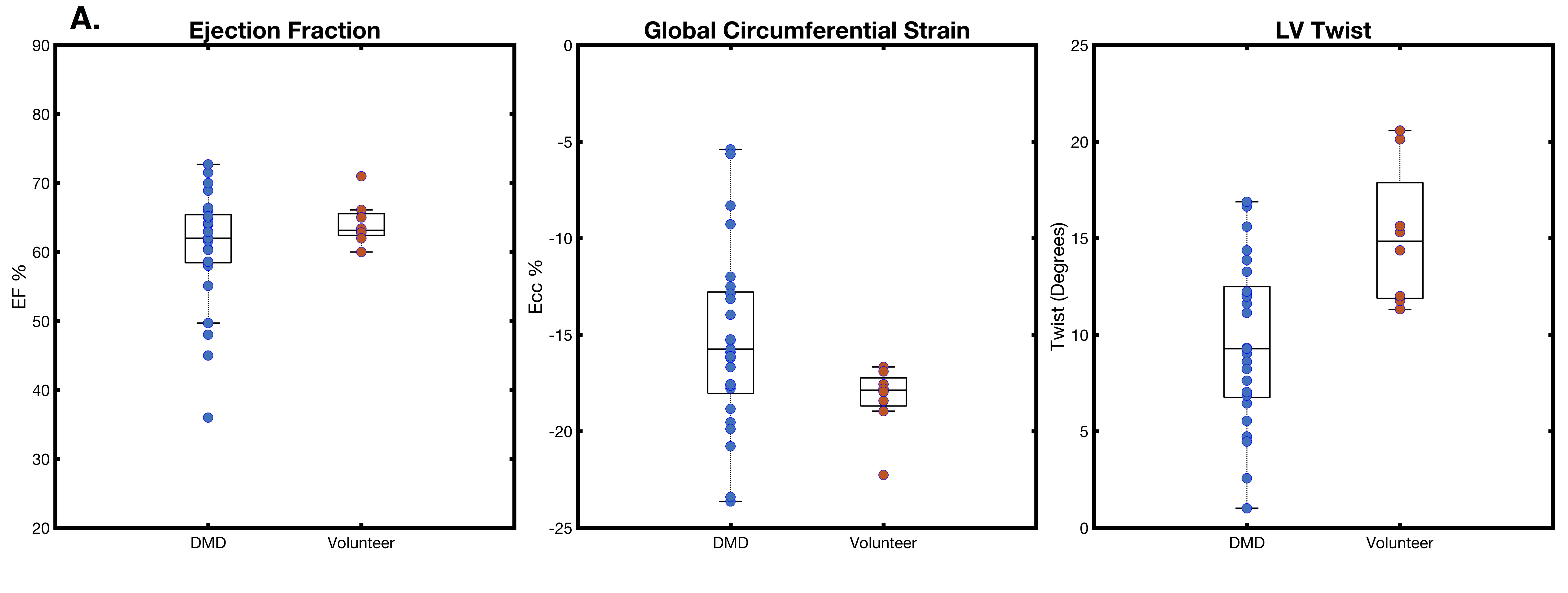
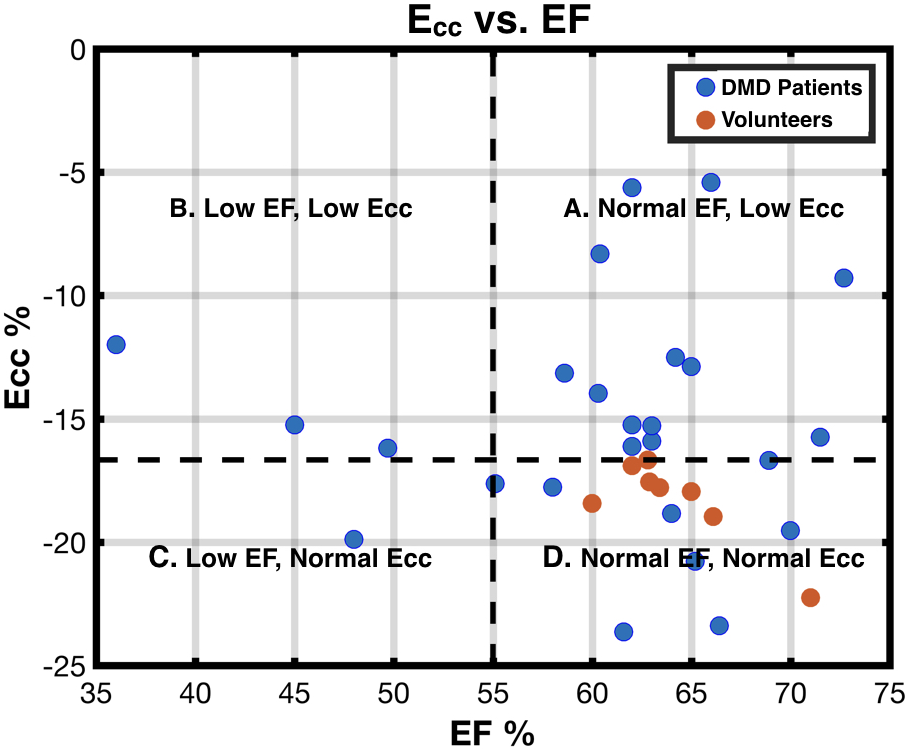
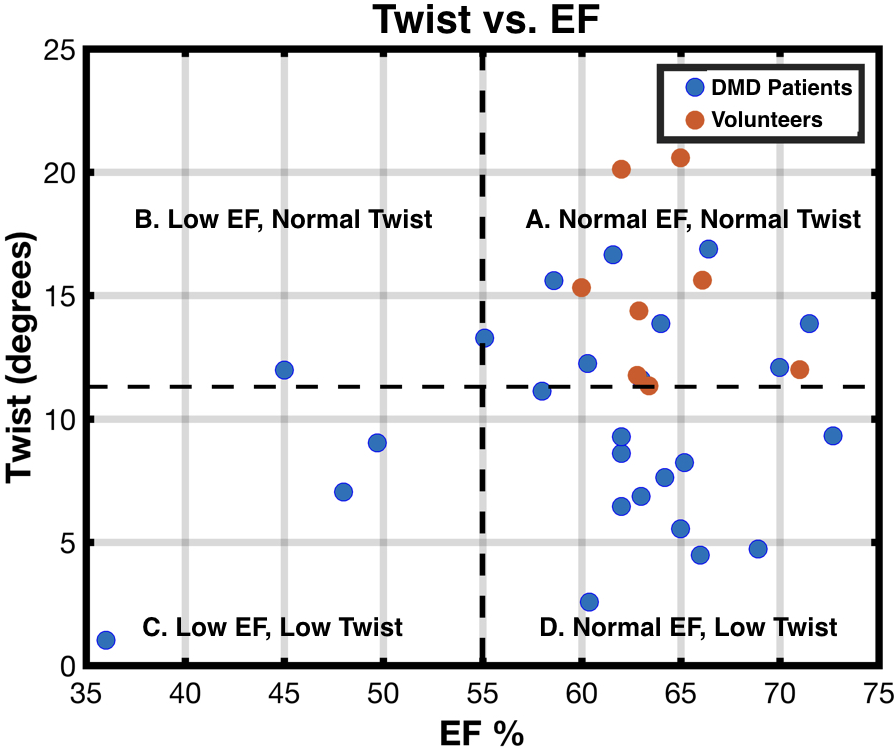
Table 1 and Figure 1 summarize LV ejection fraction, peak mid-wall Ecc, and LV twist in boys with DMD and healthy volunteers. There was no significant difference in EF between groups (62.5±8.3% vs. 63.2±3.3%, p=N.S.). A significant reduction in LV twist (9.3°±4.3° vs. 14.8°±3.6°, p< 0.004) was observed in boys with DMD compared to volunteers. Peak mid-wall Ecc (-15.8±5.8% vs. -18.5±3.2%, p<0.02) was significantly lower in magnitude. The effect sizes for Ecc and LV twist were 0.29 and 0.56, which corresponds to a 21% and a 33% non-overlap of patient and volunteer data respectively. Figures 2 and 3 plot global LV peak mid-wall Ecc and LV twist as a function of EF. Patient and volunteer data were stratified into four categories: “normal EF, normal Twist/Ecc”, “low EF, normal Twist/Ecc”, “normal EF, low Twist/Ecc”, and “low EF, low Twist/Ecc” using the smallest peak twist or Ecc values observed in our healthy volunteer cohort, and a clinical standard for cardiac dysfunction of EF<55%4 as a cutoff. Minimum values for twist and Ecc observed in volunteers agree with prior reports2,3. For Ecc and LV twist respectively, 52% and 48% of DMD patients presented with “normal EF, low Twist/Ecc” compared to all healthy volunteers. 32% and 36% of patients were “normal EF, normal Twist/Ecc” respectively. 12% of patients had “low EF, low Twist/Ecc”. 4% of patients were “low EF, normal Ecc” and “low EF, normal Twist” respectively. All volunteers had “normal EF and normal Twist/Ecc”. Table 2 summarizes data for patients (N=5) who received a follow-up scan. LV EF, twist, and Ecc were all reduced compared to the first examination, but a larger cohort is needed to test for statistical significance.Discussion & Conclusion
This data suggests that patients with DMD exhibit decreases in LV twist and peak mid-wall Ecc that likely precede decreases in EF as only a single patient with DMD was found to have “low EF, normal Twist/Ecc.” Hence, LV twist and peak mid-wall Ecc measured by MR tagging may be earlier and more sensitive indicators of cardiac dysfunction in boys with DMD. Patients with reduced EF also displayed reductions in LV twist and Ecc, but importantly, ~50% of patients with normal EF had low twist and peak mid-wall Ecc. Further, early results with a limited sample size suggest that patients that have reduced EF on a follow-up exam also exhibit reductions in twist and Ecc. LV twist has a larger effect size than Ecc and consequently may be a more sensitive measure of early dysfunction. These results corroborate the strain reports of Hor et al. and twist results of Rehyan et al. While volunteers and DMD patients were not precisely age matched, peak mid-wall Ecc is known to decrease with age, and twist remains relatively constant until middle age5. Further investigation in a larger, longitudinal cohort is warranted.Acknowledgements
This work was supported by NIH NHLBI R01 HL131975.References
1. Hagenbuch, Sean C., et al. "Detection of progressive cardiac dysfunction by serial evaluation of circumferential strain in patients with Duchenne muscular dystrophy." The American journal of cardiology 105.10 (2010): 1451-1455.
2. Hor, Kan N., et al. "Regional circumferential strain is a biomarker for disease severity in duchenne muscular dystrophy heart disease: a cross-sectional study." Pediatric cardiology 36.1 (2015): 111-119.
3. Reyhan, Meral L., et al. "Effect of free‐breathing on left ventricular rotational mechanics in healthy subjects and patients with duchenne muscular dystrophy." Magnetic resonance in medicine 77.2 (2017): 864-869.
4. Sweitzer, Nancy K., et al. "Comparison of clinical features and outcomes of patients hospitalized with heart failure and normal ejection fraction (≥ 55%) versus those with mildly reduced (40% to 55%) and moderately to severely reduced (< 40%) fractions." The American journal of cardiology 101.8 (2008): 1151-1156.
5. Reyhan, Meral, et al. "Left ventricular twist, but not circumferential-longitudinal shear angle, increases with increasing age in normal subjects." Journal of Cardiovascular Magnetic Resonance 15.1 (2013): P7.
Figures