0563
LGE-CMR derived texture features reflect poor prognosis in hypertrophic cardiomyopathy patients with systolic dysfunction: preliminary results1Peking Union Medical College, Beijng, China, 2CAS Key Laboratory of Molecular Imaging, Institute of Automation, Chinese Academy of Sciences, Beijing, China
Synopsis
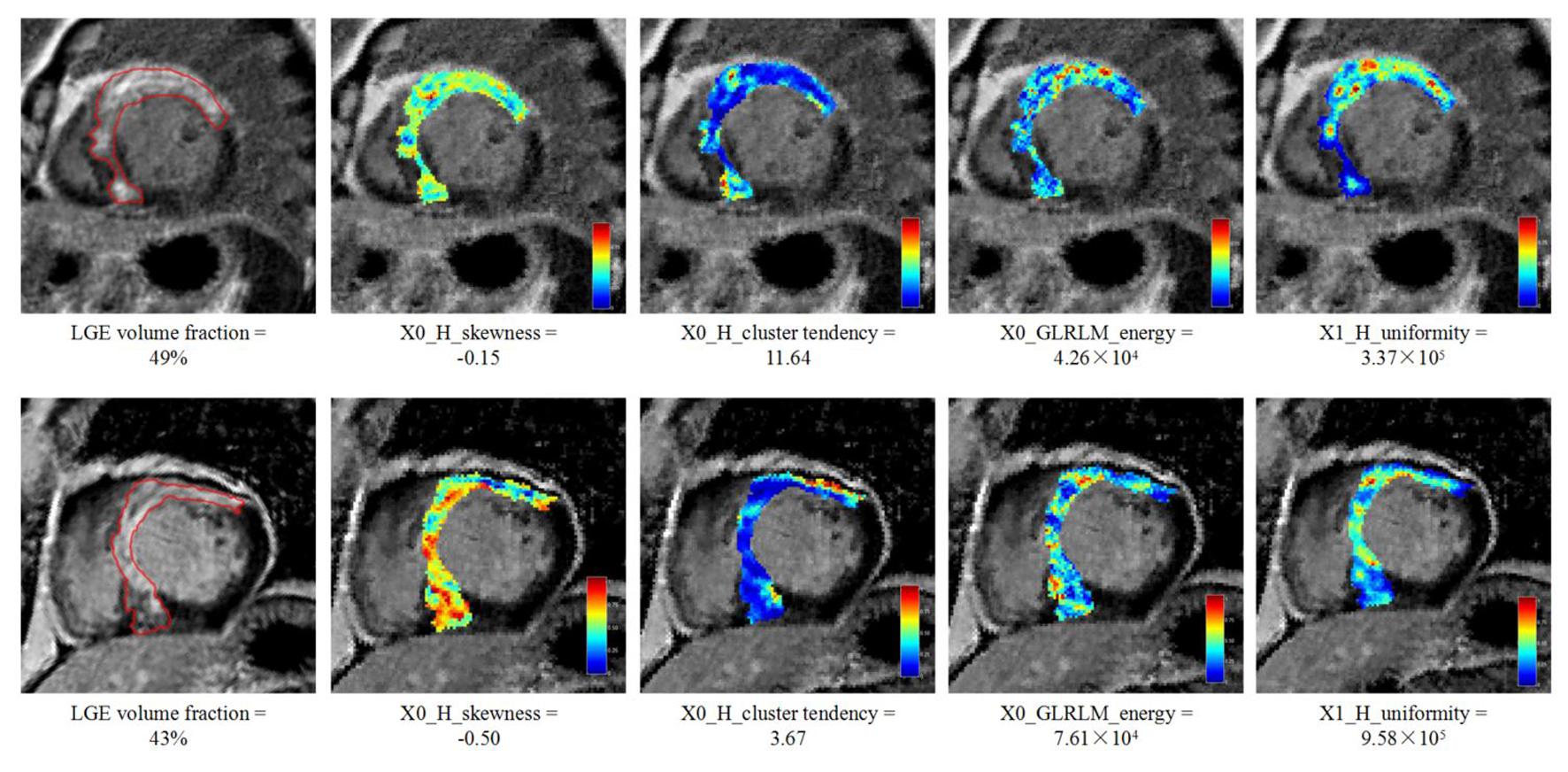
In this study, we evaluated the prognostic value of texture features based on late gadolinium enhancement cardiac magnetic resonance (LGE-CMR) images in hypertrophic cardiomyopathy (HCM) patients with systolic dysfunction. 1.5 T CMR cine and LGE images were performed on 67 HCM patients with systolic dysfunction. Texture features were extracted from LGE images. Cox proportional hazard analysis and Kaplan-Meier analysis were used to determine the association of texture features with event free survival. The result showed that increased LGE heterogeneity (higher X0_GLRLM_energy, higher X1_H_uniformity, lower X0_H_skewness and lower X0_GLCM_cluster_tendency) was associated with adverse events in HCM patients with systolic dysfunction.
Introduction
LGE derived from CMR has gained wide interest to assess fibrosis in HCM. Several studies of large cohorts indicated that the presence or extent of LGE is a prognostic factor of adverse events 1-3. However, in previous studies, investigators only evaluated LGE by positive/negative or by LGE extent (LGE volume/myocardial volume). Thus, the challenge is how to describe heterogeneous LGE patterns in an objective way to provide further insights into the role of LGE on adverse events.Medical image texture contains important information about the structural arrangement of surfaces and their relationship to the surrounding environment which are often invisible to the naked eye. We hypothesize that texture features of LGE are associated with event free survival in HCM patients with systolic dysfunction. Thus, the purpose of this preliminary study was to evaluate texture features of LGE-CMR images in HCM patients with systolic dysfunction to assess the prognostic potential.Methods
We collected 67 HCM patients with advanced systolic dysfunction from January 2011 to January 2016 in our Hospital. All patients underwent systematic clinical evaluation and CMR examinations. MR images were acquired on a 1.5-T scanner (MAGNETOM Avanto, Siemens). LGE images were obtained using a segmented phase-sensitive inversion recovery Turbo Fast Low Angle Shot sequence (FOV, 370×320mm; matrix, 256×168; slice thickness, 8mm; slice gap, 2mm). LGE volume fraction were quantitatively evaluated according to the American Heart Association 17-segment model by using CMR 42 (Circle Cardiovascular Imaging, Calgary, Alberta, Canada). LGE image segmentation were performed on ITK-SNAP 2.2.0 software. The process of image filtering and feature extraction was performed using in-house software with algorithms implemented in MATLAB 2014a (Mathworks, Natick, MA, USA). All patients were followed up every 6 months after CMR examination. The end point was the composite of cardiovascular death (cardiac death due to progression of heart failure or SCD), aborted SCD, heart transplantation and unscheduled heart failure hospitalization. Spearman correlation coefficients between each pair of features were computed to analyze the linear correlation. Based on these correlation coefficients, features were divided into different groups to ensure all pairs of features in each group had a |r| greater than 0.6. Based on different groups of the independent segmentations of 30 patients, the intra-/inter-class correlation coefficient (ICC) was used to estimate the robustness of the texture features extracted. Kaplan-Meier curves and log rank test were used to explore the association of the LGE volume fraction and texture features with survival. LGE extent and each texture feature were dichotomized according to the receiver operating characteristic (ROC) optimum point to split the survival curves. Univariate and multivariate proportional hazard analysis was used to estimate the predictors of end point events.Results
The preliminary study on LGE texture features shows that increased LGE heterogeneity [higher X0_GLRLM_energy (HR=0.735), higher X1_H_uniformity (HR=1.269), lower X0_H_skewness (HR=0.783) and lower X0_GLCM_cluster_tendency (HR=0.735)] as well as LGE extent (HR=1.911) was strongly associated with adverse events in HCM patients with systolic dysfunction. Furthermore, LGE extent (HR=1.548, 1.650, 1.586 and 1.766 respectively, p<0.05) remained a good independent predictor of event free survival outcome when adjusted by texture features.Discussion
In this study, some patients with similar LGE extent experienced different survival outcomes in this preliminary study. This may be partially explained by the LGE (fibrosis) heterogeneity. A histological study of 30 transplanted HCM hearts with systolic dysfunction showed that there exist at least 3 qualitative types of fibrosis in HCM with systolic dysfunction, that is, prevalently replacement (or scar-like), prevalently interstitial-perimyocyte, and mixed fibrosis type 4. The different fibrosis type and the mix between fibrosis and viable myocytes may be the source of the heterogeneous internal information of myocardial fibrosis as well as the LGE heterogeneity. The heterogeneously distributed fibrosis not only forms electric conduction barriers but also facilitates the formation of critical isthmuses of viable myocytes that support reentrant circuits, which is especially arrhythmogenic 5. It is not possible to quantify fibrosis heterogeneity visually by current LGE technique, but our preliminary findings showed that texture analysis can be used to characterize the myocardial fibrosis spatial heterogeneity in LGE images, which may represent arrhythmogenic substrate and subsequently adverse event.Conclusions
Our study showed that increased fibrosis heterogeneity (higher energy, higher uniformity, lower skewness and lower cluster tendency) was associated with adverse events in HCM patients with systolic dysfunction. Texture features could take advantage of conventional LGE-CMR images.Acknowledgements
No acknowledgement found.References
1. O'Hanlon R, Grasso A, Roughton M, et al. Prognostic significance of myocardial fibrosis in hypertrophic cardiomyopathy. J Am Coll Cardiol. 2010;56:867-874.
2. Green JJ, Berger JS, Kramer CM, et al. Prognostic value of late gadolinium enhancement in clinical outcomes for hypertrophic cardiomyopathy. JACC Cardiovasc Imaging. 2012;5:370-377.
3. Chan RH, Maron BJ, Olivotto I, et al. Prognostic value of quantitative contrast-enhanced cardiovascular magnetic resonance for the evaluation of sudden death risk in patients with hypertrophic cardiomyopathy. Circulation. 2014;130:484-495.
4. Galati G, Leone O, Pasquale F, Olivotto I, et al. Histologic and histometric characterization of myocardial fibrosis in end-stage hypertrophic cardiomyopathy: a clinical-pathological study of 30 explanted hearts. Circulation: Heart Failure. 2016;9: e003090.
5. Wu K C. Sudden Cardiac Death Substrate Imaged by Magnetic Resonance Imaging: From Investigational Tool to Clinical Applications. Circulation: Cardiovascular Imaging. 2017;10(7):e005461.
Figures