0524
Developmental Score of the Neonatal Brains: Characterizing Diffusion MRI Changes in the Term- and Preterm-born Infants1Radiology, Johns Hopkins University School of Medicine, BALTIMORE, MD, United States, 2Diagnostic Radiology and Nuclear Medicine, University of Maryland School of Medicine, BALTIMORE, MD, United States, 3Laboratory Medicine, Children’s and Women’s Health, Norwegian University of Science and Technology, Trondheim, Norway
Synopsis
Postmenstrual age (PMA) is used as a time-scale to evaluate brain development, but it contains inaccuracy with regards to the estimated time of conception because the duration from the last menstrual period to conception varies. To address this variation, we designed a developmental score (DevS) that aligned individuals with similar development patterns together, and provides a linear trajectory of DTI-measurement as a function of an underlying brain developmental index. Compared to PMA, DevS showed an improved the regression with DTI-measurements, and it better separated the developmental differences between term- and preterm-born infants.
Introduction
Diffusion tensor imaging (DTI) is useful in studying developmental changes in the neonatal brain.1-5 However, analyzing DTI data in longitudinal and cross-sectional large cohort studies, however, is challenging, because individuals enter the study at different developmental stages with uncertainty in duration since conception. We aim to develop a computational method that characterizes the developmental trajectory from such database. The proposed developmental score (DevS) is a surrogate of postmenstrual age (PMA), which aligns cross-sectional data in a pseudo-longitudinal manner, and forms a linear relation with biomarkers, e.g., the DTI-measurements. We used DevS to investigate normal brain developmental changes in the term-born neonates, and the deviations from normal development due to preterm-birth.Methods
Developmental score (DevS): The rationale and mathematical model of DevS is similar to the previously published work on disease progression score.6, 7 Briefly, two relations between PMA ($$$t$$$), DevS ($$$s$$$), and DTI measurement ($$$y$$$, MD in this study) were used:
$$$s_{i,j}=\alpha_{i}\cdot t_{i,j}+\beta_{i}$$$ Equation 1
$$$y_{i,j}=a\cdot s_{i,j}+b+\epsilon_{i,j}$$$ Equation 2
where $$$i$$$ and $$$j$$$ refer to subject $$$i$$$ at the $$$j$$$th visit; [$$$\alpha$$$, $$$\beta$$$, $$$a$$$, $$$b$$$] are the model parameters to fit; and $$$\epsilon$$$ is the variance of DTI measurement. The model was fitted using an expectation–maximization (EM) approach7.
Data acquisition: MRI of the infants (PMA between 37-57.5 weeks) was performed at the University of Hawaii and the Queen's Medical Center MR Research Center in Honolulu, HI, as described in our prior work.8-10 Preterm-born infants (n=48, gestational age at birth <37 weeks) and term-born infants (n=79, ≥37 weeks) were included in the analysis, and each infant had 1-4 longitudinal follow-up scans. DTI was acquired using a single-shot EPI at 2 x 2 mm2 in-plane resolution; 40-50 slices with 2.5 mm thickness; TE = 106 ms and TR = 7- 9 s; and 12 diffusion directions with b = 1000 s/mm2.
Image analysis: The individual DTI images were transformed to the JHU-neonate single brain DTI atlas,11 through linear AIR transformation followed by dual-channel (FA and MD) Large Deformation Diffeomorphic Metric Mapping (LDDMM),11, 12 after which the images were parcellated into 126 ROIs. A MD threshold of 2x10-3 mm2/s was to exclude CSF component.
Results
Two sets of analysis were performed.
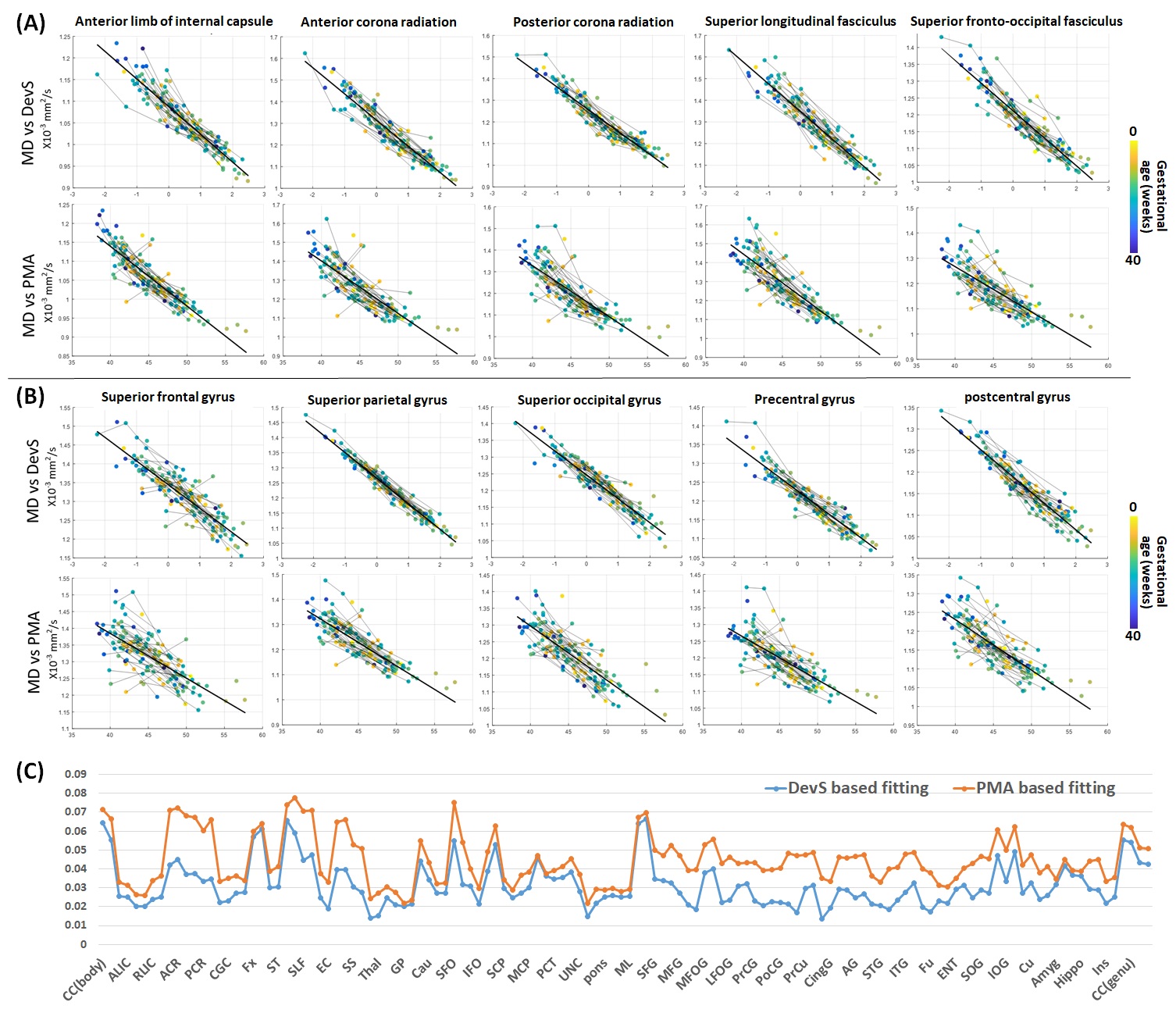
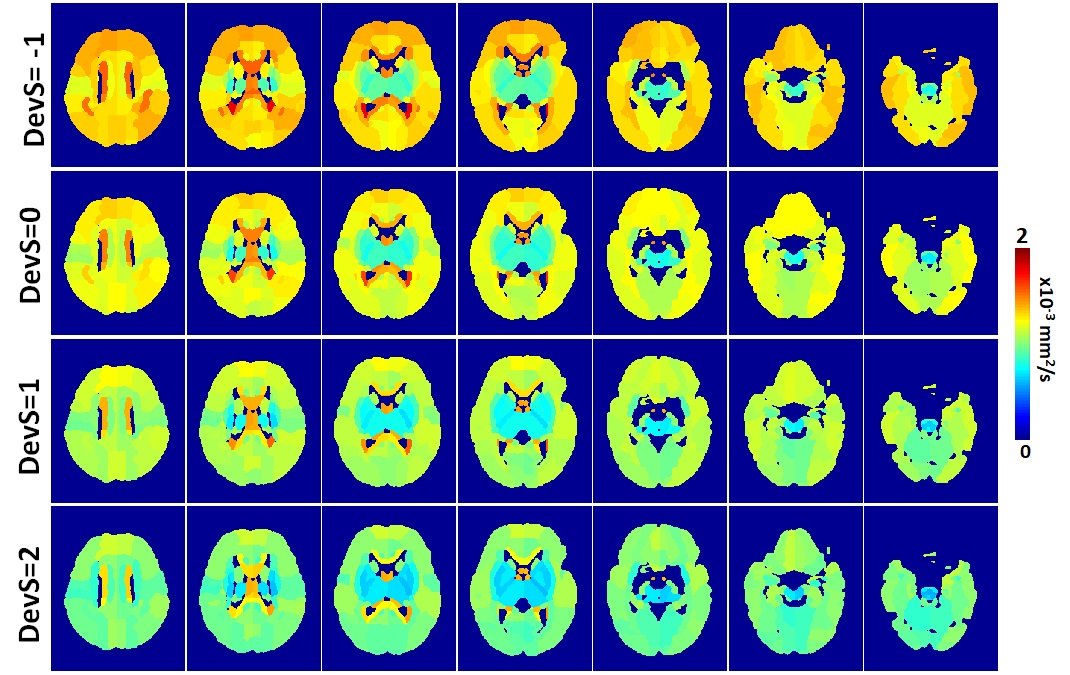
1) DevS in the term-born neonates. DevS was derived using PMA and MD measurements in 126 ROIs of 79 neonatal DTI data (1-4 visits per data, 171 data in total), according to Equations 1-2. Fig. 1A-B shows the linear regressions between MD and DevS and those between MD and PMA in several representative white and gray matter structures. The fitting errors (root-mean-square, RMS) were significantly reduced using DevS as the x-axis (Fig. 1C). Based on the DevS model, we were able to infer the MD values in each ROI at specific developmental stage (Fig. 2). For example, during early development (DevS= -1), the frontal cortex and commissural and projection fibers had relatively high MD compared to the other brain regions; whereas at late gestation (DevS = 2), MD decreased in general, and deep brain regions showed the lowest MD.
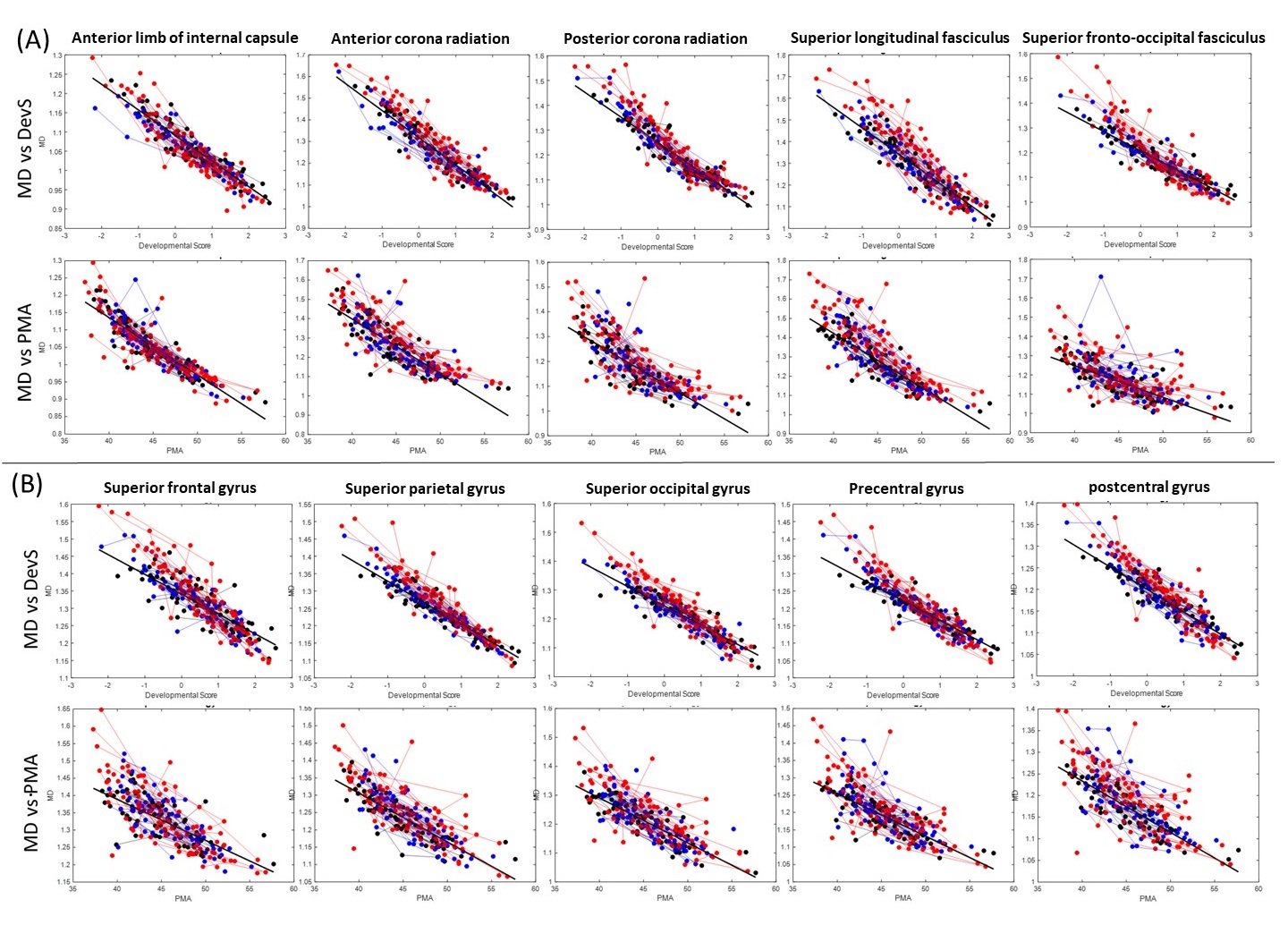
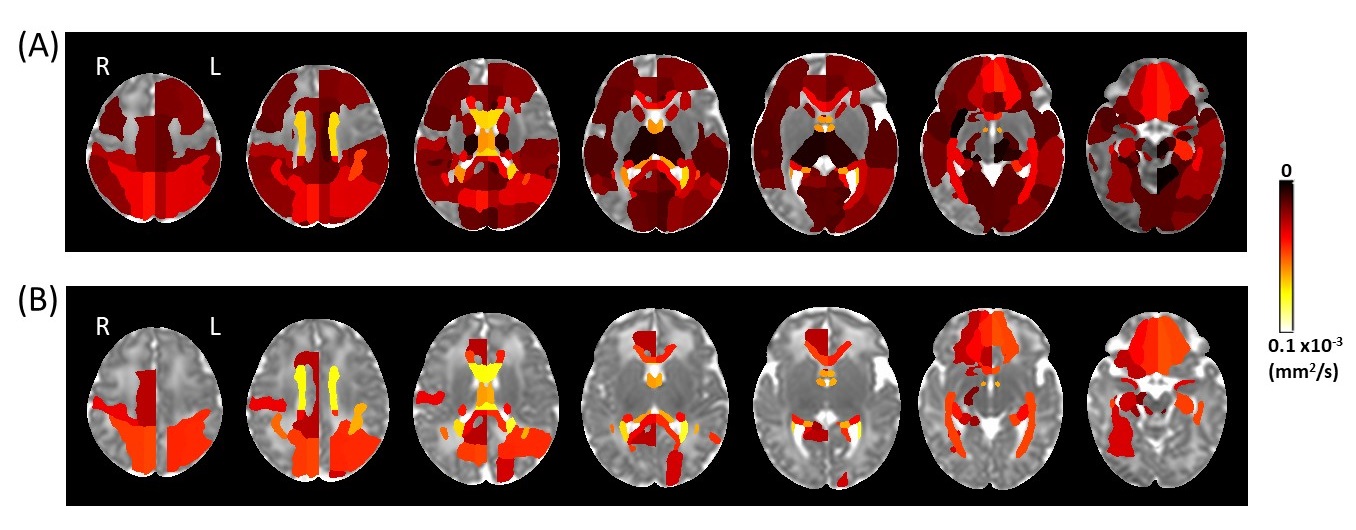
2) Developmental differences between term-born and preterm-born neonates. We used the scans from half of the term-born neonates (n=40) to train the DevS model, and used the model parameters to obtain DevS in the other half of term-born (n=39) and preterm-born (n=48) infants. The differences in developmental trajectories were more easily separated after transforming the x-axis from PMA to DevS (Fig. 3). We compared the RMS of regression errors between the fitted (using term-born training data) and true MD values. Using the DevS, significantly higher RMS was found in the preterm-born group compared to the term-born group, in multiple ROIs (Fig. 4A), indicating that the model trained by term-born infants did not fit well with the preterm-born infants. Fewer regions showed higher RMS in the preterm-born group compared to the term-born group, when PMA was used in regression (Fig. 4B).
Discussion and Conclusion
We proposed that the DevS can serve as a standardized index of brain development, which can be derived from DTI-measurements in the infant brains. Transforming the x-axis from PMA to DevS improved the linear regression with DTI-measurements, which helped to differentiate the brain development in term- and preterm-born neonates. The results indicate that the use of DevS could improve the characterization of normal developmental pattern and detection of developmental abnormalities. A potential limitation of this method is that the relationship between DevS and DTI-measurements was assumed to be linear, which may not be optimal if applied to non-linear developmental trajectories.Acknowledgements
This work is supported by NIH grants R21NS098018 and R01HD065955.References
1. Mukherjee P, Miller JH, Shimony JS, et al. Normal brain maturation during childhood: developmental trends characterized with diffusion-tensor MR imaging. Radiology. 2001; 221: 349-58.
2. Brown TT, Kuperman JM, Chung Y, et al. Neuroanatomical assessment of biological maturity. Curr Biol. 2012; 22: 1693-8.
3. Zhang L, Thomas KM, Davidson MC, Casey BJ, Heier LA and Ulug AM. MR quantitation of volume and diffusion changes in the developing brain. AJNR American journal of neuroradiology. 2005; 26: 45-9.
4. Saksena S, Husain N, Malik GK, et al. Comparative evaluation of the cerebral and cerebellar white matter development in pediatric age group using quantitative diffusion tensor imaging. Cerebellum. 2008; 7: 392-400.
5. Yap QJ, Teh I, Fusar-Poli P, Sum MY, Kuswanto C and Sim K. Tracking cerebral white matter changes across the lifespan: insights from diffusion tensor imaging studies. J Neural Transm (Vienna). 2013; 120: 1369-95.
6. Jedynak BM, Lang A, Liu B, et al. A computational neurodegenerative disease progression score: method and results with the Alzheimer's disease Neuroimaging Initiative cohort. NeuroImage. 2012; 63: 1478-86.
7. Bilgel M, Prince JL, Wong DF, Resnick SM and Jedynak BM. A multivariate nonlinear mixed effects model for longitudinal image analysis: Application to amyloid imaging. NeuroImage. 2016; 134: 658-70.
8. Akazawa K, Chang L, Yamakawa R, et al. Probabilistic maps of the white matter tracts with known associated functions on the neonatal brain atlas: Application to evaluate longitudinal developmental trajectories in term-born and preterm-born infants. Neuroimage. 2016; 128: 167-79.
9. Chang L, Akazawa K, Yamakawa R, et al. Delayed early developmental trajectories of white matter tracts of functional pathways in preterm-born infants: Longitudinal diffusion tensor imaging data. Data in brief. 2016; 6: 1007-15.
10. Wu D, Chang LD, Akazawa K, et al. Mapping the critical gestational age at birth that alters brain development in preterm-born infants using multi-modal MRI. NeuroImage. 2017; 149: 33-43.
11. Oishi K, Mori S, Donohue PK, et al. Multi-contrast human neonatal brain atlas: application to normal neonate development analysis. Neuroimage. 2011; 56: 8-20.
12. Miller MI, Christensen GE, Amit Y and Grenander U. Mathematical textbook of deformable neuroanatomies. Proceedings of the National Academy of Sciences of the United States of America. 1993; 90: 11944-8.
13. Christensen GE, Rabbitt RD and Miller MI. Deformable templates using large deformation kinematics. Ieee T Image Process. 1996; 5: 1435-47.
Figures