0480
Estimation of a signal-appropriate reference volume to improve registration of high b-value diffusion volumes in the human placenta1Medical Biophysics, Western University, London, ON, Canada, 2Dept of Obstetrics and Gynaecology, Western University, Ontario, ON, Canada, 3Division of Maternal, Fetal, and Newborn Health, Children's Health Research Institute, London, ON, Canada
Synopsis
A technique is presented to aid in better motion correction of high b-value diffusion images of the human placenta in utero for the purposes of quantification using intra-voxel incoherent motion (IVIM). A registration reference volume is calculated with signal intensities and tissue features with similarity to volumes with high diffusion weighting, and produce more successful registrations than when using the b=0 volume as a reference.
Introduction
Intravoxel incoherent motion (IVIM) is a diffusion imaging technique utilizing a range of diffusion weightings (b-values) to estimate fast and slow water movement within a tissue compartment1. IVIM is of interest for non-invasive study of the human placenta, as placental perfusion difficulties are thought to contribute to diseases of pregnancy such as inter-uterine growth restriction2. However, when using IVIM to assess the human placenta in utero, volumes representing individual b-values may become misaligned during imaging due maternal respiration, uterine contraction, and fetal movements. Registration algorithms (e.g. Elastix3) exist to correct these misalignments by re-orienting and scaling individual volumes to a reference image. Volumes with higher b-values are more challenging to register because of their low SNR and differing tissue representation (e.g. amniotic fluid signal) relative to the reference volume. Ben-Amitay et al4 suggested a method of high b-value registration in the brain by fitting an initial diffusion curve without the high b-values and applying this model of signal decay to the reference volume, resulting in a “template” reference volume similar in features to the high b-value volume to be registered. The purpose of this study was to test the efficacy of a similar approach in registering high b-value diffusion-weighted volumes of the human placenta.Methods
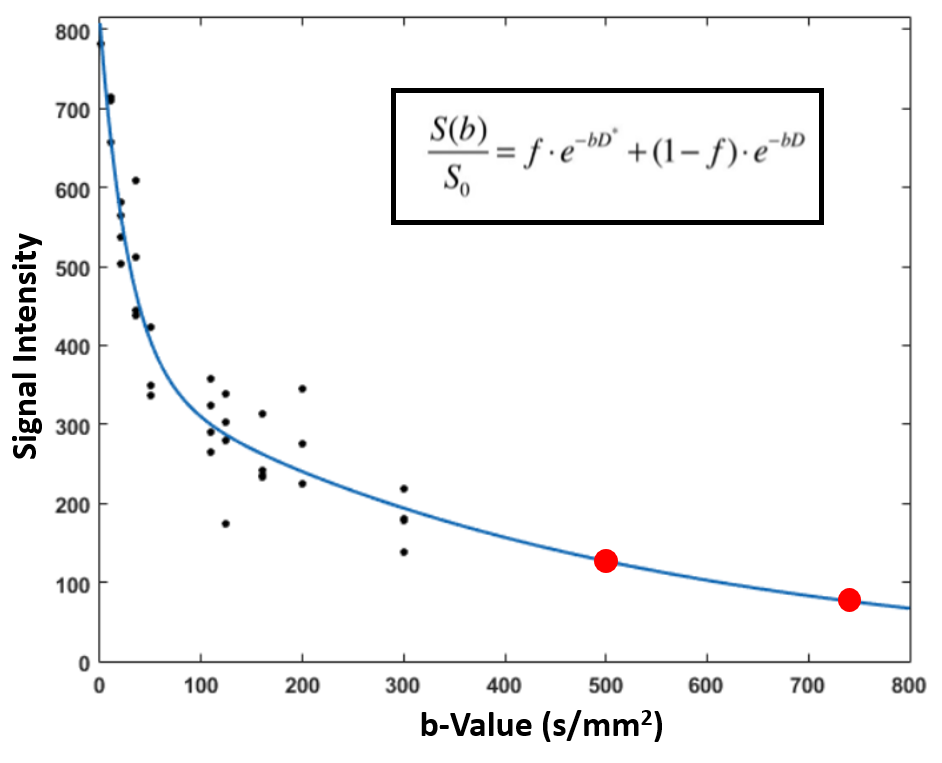
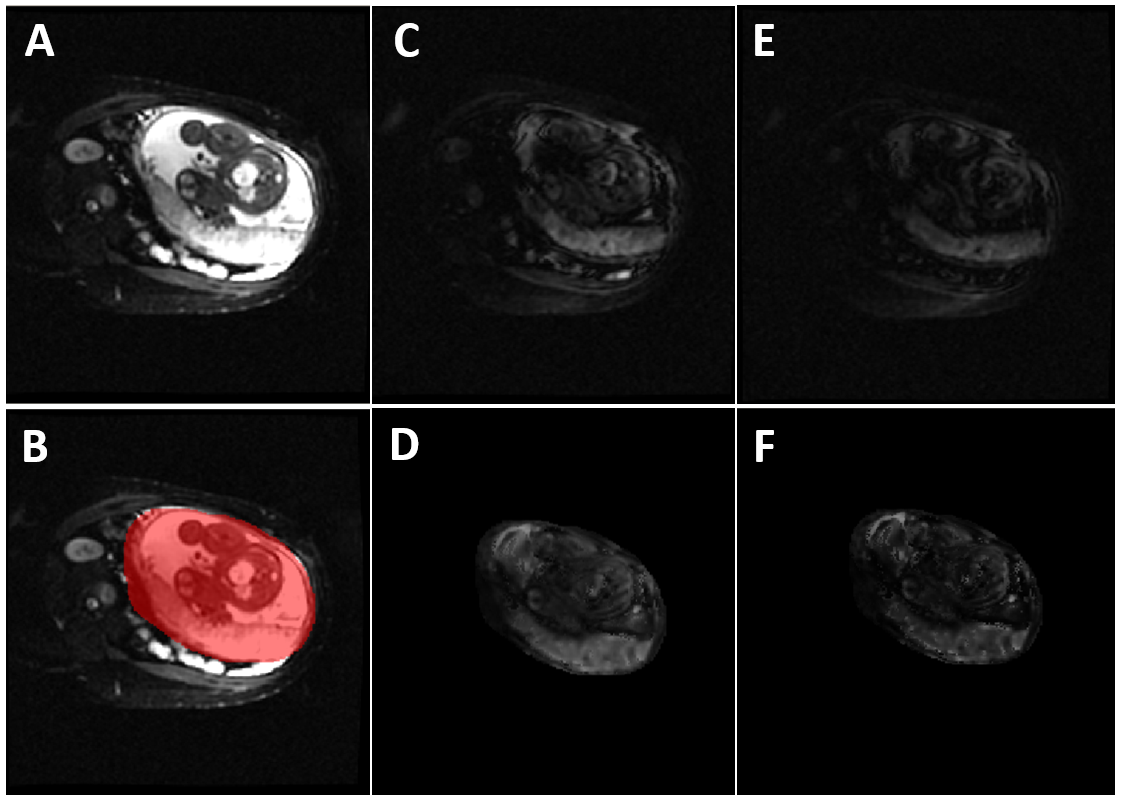
With approval of our local research ethics board, 3 pregnant volunteers (31.6yo, 29-36; gestational age 33.9 wks; 31.1-36.4) were scanned free-breathing at 1.5T (GE Optima MR450W, Milwaukee, WI) using a 32-coil body array. The IVIM dataset (TR/TE: 7000/71.4 ms, axial, FOV 50cm, 128x128 matrix, 5mm slice, A-P direction, 11 b-values 0-750 s/mm2, 3-4 acquisitions each) was motion-corrected by aligning each b>0 volume to the b=0 volume using a rigid-affine-nonlinear (B-spline) processing stream with Mattes mutual information cost function within Elastix3,5. A voxel-wise biexponential fit was performed with 10 b-values 0-300 s/mm2, each with 3-4 data points, using Matlab (2015a, The Mathworks, Natick, MA) (Fig. 1). The biexponential fit at each voxel location was then extrapolated from the b=0 volume to estimate the signal decay at higher b-values (b=500 and 750 s/mm2), producing a “pseudo” volume for each in the reference space of the b=0 (Fig. 1). The acquired high b-value volumes were then registered to the “pseudo” volumes. Regions-of-interest (ROIs) representing the placental boundary were drawn on 3 slices per volume representing the ¼, ½, and ¾ planes in a stack of axial images for the b=0 reference volume, the b=50,300,500,750 volumes post-registration to original b=0, and the b=500,750 volumes post-registration respective to their “pseudo” volumes. ROI drawing and calculation of ROI overlap between registered and reference volumes was performed with FSL6. The Dice coefficient7 was used to assess the overlap of b=0-registered and “pseudo”-registered volumes relative to the b=0 reference volume. A one-way ANOVA and Tukey’s test for multiple comparisons were performed between the Dice coefficients of each b-value and registration strategy using Prism (v7.03, GraphPad, San Diego, CA).Results
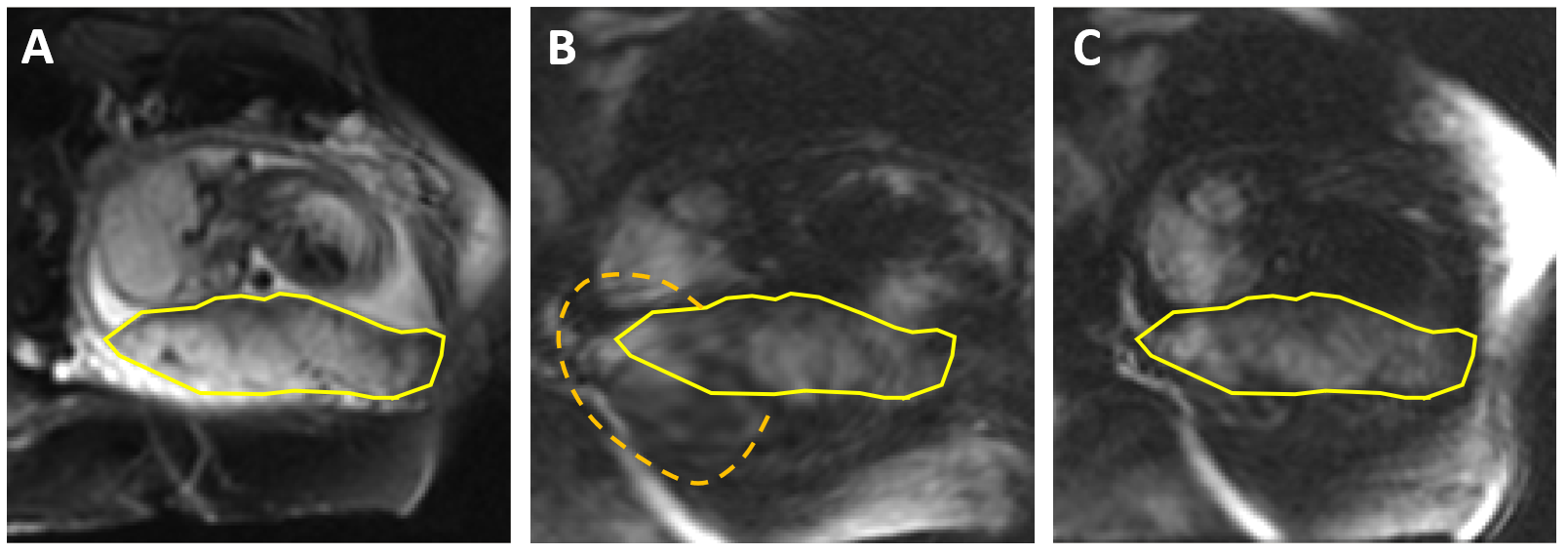
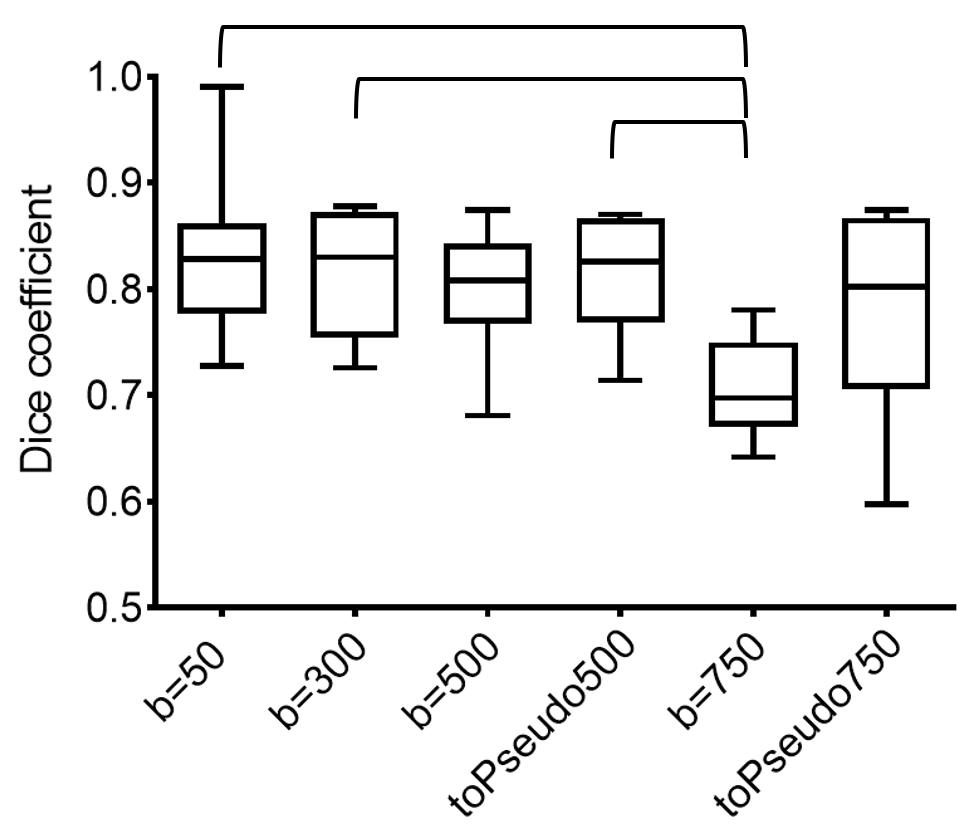
The “pseudo” volumes show more visual similarity to the high b-dependant tissue features than the b=0 image originally used as a registration reference (Fig. 2). Final registrations to the “pseudo” volumes show improvement in alignment to the reference space compared to registering directly to the b=0 reference image (Fig. 3). The mean Dice coefficients when using the b=0 reference image were 0.83+/-0.07, 0.81+/-0.06, 0.80+/-0.06, and 0.71+/-0.05 for b=50, 300, 500, and 750, respectively (Fig. 4). The mean Dice coefficient when using the “pseudo” reference image was 0.82+/-0.06 for b=500 and 0.78+/-0.09 for b=750. The ANOVA was significant (p<0.005), and Tukey’s test revealed that b=750, when registering to the original b=0, achieved a significantly worse Dice coefficient than b=50 or b=300.Discussion
Alignment of the human placenta across multiple MRI volumes during a free-breathing acquisition continues to be a challenge for available registration methods. The proposed technique of using a “pseudo”-reference image significantly improved the registration accuracy in high-b-value, low-SNR diffusion volumes to the level of accuracy obtained with higher SNR volumes. Calculation of the “pseudo”-reference relies upon the accuracy of registration and subsequent biexponential fit of b-values 0-300 s/mm2, and thus could be corrupted in cases of extreme motion artifact within these volumes.Conclusion
A registration reference volume was created with signal intensities and tissue features appropriate to high diffusion-weighted volumes of the uterus and placenta, and demonstrated an improvement in registration of these images compared to use of the full signal b=0 reference volume. This technique shows promise in alleviating some of the challenges involved in quantification of the human placenta in utero using intra-voxel incoherent motion.Acknowledgements
Grant support from the Children’s Health Research Institute, National Institutes of Health, U01 HD087181-01 and Canadian Institutes of Health Research, MOP-209113.References
1. Le Bihan et al. (1986). Radiol 161:401-407.
2. Mandruzzato, G (2008). Arch Perinatal Med 14:7-8.
3. Klein et al. (2010). IEEE Trans Med Imaging 29(1):196-205.
4. Ben-Amitay et al. (2012). Magn Reson Med 67:1694-1702.
5.Turk et al. (2017). J Magn Reson Imaging 46(2):403-412.
6. Jenkinson et al. (2012). NeuroImage 62:782-290.
7. Dice et al. (1945). Ecology 26:297-302.
Figures