0476
3D non-rigid motion-corrected dynamic contrast enhanced MRI of the liver with high isotropic resolution1Department of Radiology, Charité, Berlin, Germany, 2Division of Imaging Sciences and Biomedical Engineering, King’s College London, London, United Kingdom, 3Physikalisch-Technische Bundesanstalt (PTB), Braunschweig and Berlin, Germany
Synopsis
Dynamic Contrast Enhanced (DCE) MRI of the liver is an important diagnostic tool. The main challenge is complex respiratory motion of the abdomen. Here we present a motion correction approach for DCE-MRI. Golden Radial Phase Encoding data was acquired continuously in a patient after contrast injection during free-breathing. In a first step, non-rigid respiratory motion was estimated from the data. The motion information was then used to reconstruct 3D motion corrected dynamic images with a temporal resolution of 13s and an isotropic spatial resolution of 1.5mm3. The proposed technique strongly reduced motion artefacts and ensured high image quality.
Introduction
Dynamic Contrast Enhanced (DCE) MRI of the liver is an important diagnostic tool to detect and assess liver tumors. The main challenge is the complex respiratory motion of the organs in the abdomen. Commonly these scans are obtained during multiple breath holds at fixed time points after contrast injection 1. Although this ensures high image quality, it strongly limits the number of acquisition during contrast uptake and also limits the achievable resolution. Respiratory motion correction has been proposed to overcome this problem but current techniques only achieved small coverage along the slice encoding direction and did not achieve high isotropic image resolution 1-4.
Here we present a novel approach which provides dynamic contrast enhancement MR images with isotropic resolution of 1.5mm3 and full coverage of the entire abdomen with temporal resolution of 13s. Respiratory motion information is obtained from the data itself and used in a motion-compensated image reconstruction to minimize respiratory motion artefacts.
Methods
Data acquisition: A 3D fat-suppressed GRE acquisition (TE/TR/FA: 1.36ms/2.1ms/12°) was carried out continuously after contrast injection using Golden Radial Phase Encoding (GRPE)5. A partial Fourier factor was applied along the radial phase encoding direction and 512 GRPE lines were obtained. That led to a matrix size of 192x120x512 and a total scan time of 4min. The preliminary study was carried out in one patient after injection of a Gadolinium-based contrast agent (49 years, female, 7 mL dose, 57 kg).
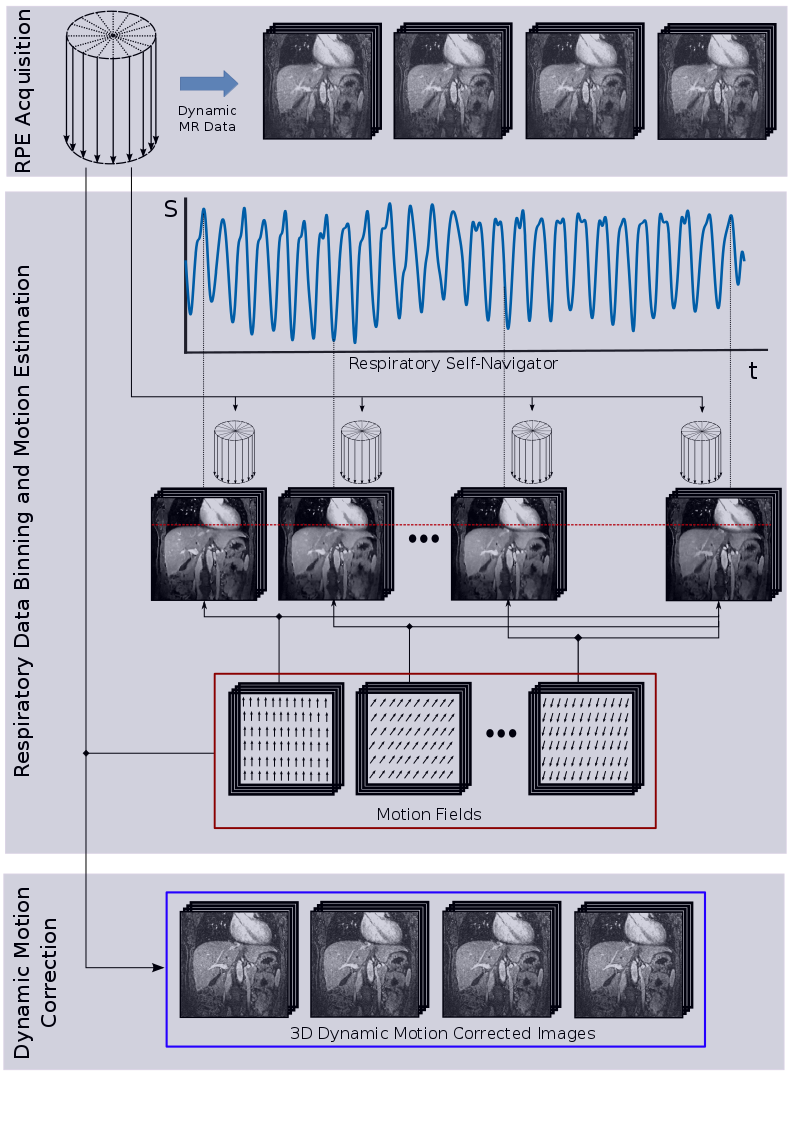
Motion estimation: In a first step a 1D navigator along the foot-head direction was extracted from the k-space data which was then used to bin the data into six different respiratory phases. Because GRPE provided not just a simple self-navigator signal from the k-space centre but a full 1D projection along foot-head direction, the temporal changes due to contrast uptake and respiratory motion could be easily separated. 3D images for each respiratory image was reconstructed using an iterative SENSE approach with spatial and temporal regularization. All image reconstruction was carried out offline using Matlab. 3D non-rigid respiratory motion was then estimated using a spline-based image registration with normalized mutual information metric (NIFTYREG) 6.
Motion correction: The motion information was then incorporated directly into the image reconstruction of the dynamic motion corrected images. 18 dynamic phases were reconstructed using a kt-SENSE approach8 leading to a temporal resolution of 13s. The regularization image required for kt-SENSE was obtained by a dynamic 3D low resolution image from the fully sampled k-space centre of the GRPE data. Figure 1 gives an overview of the method.
Results
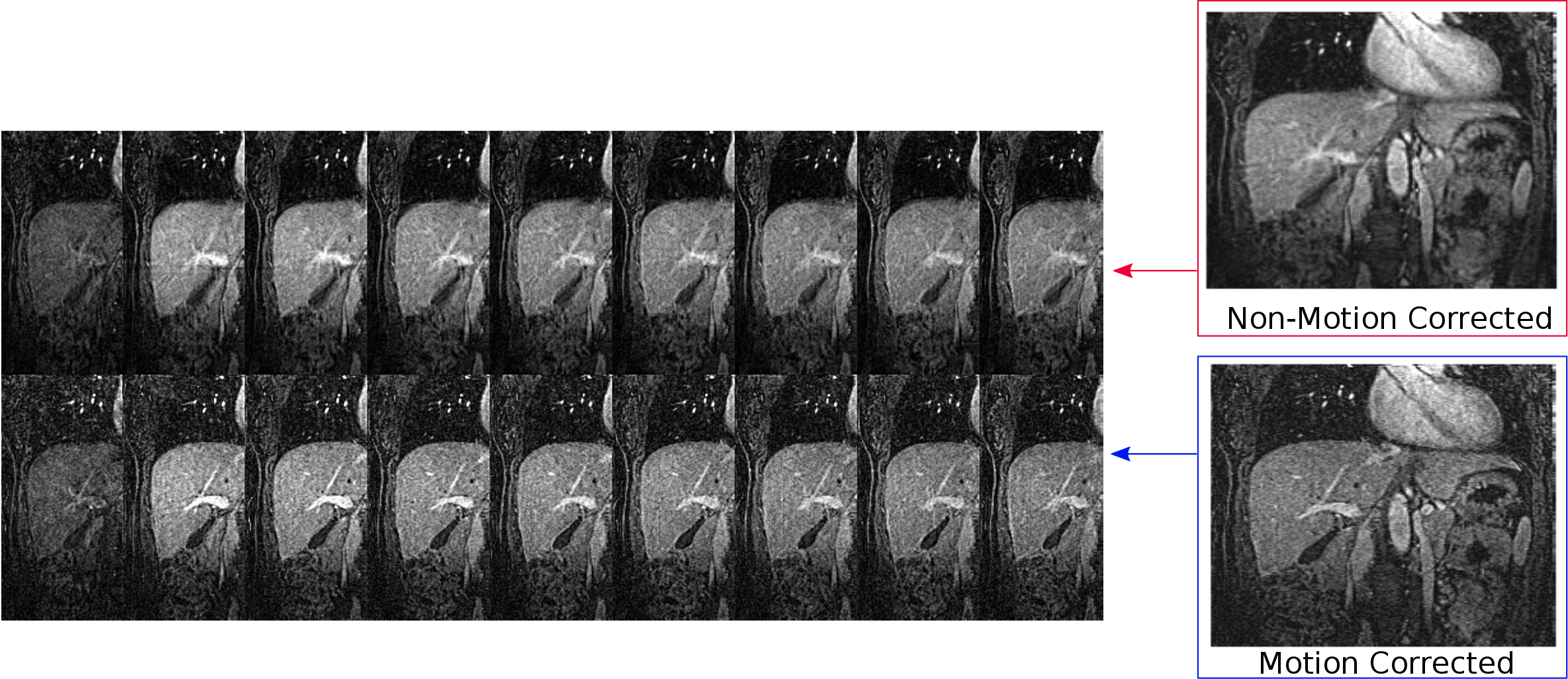
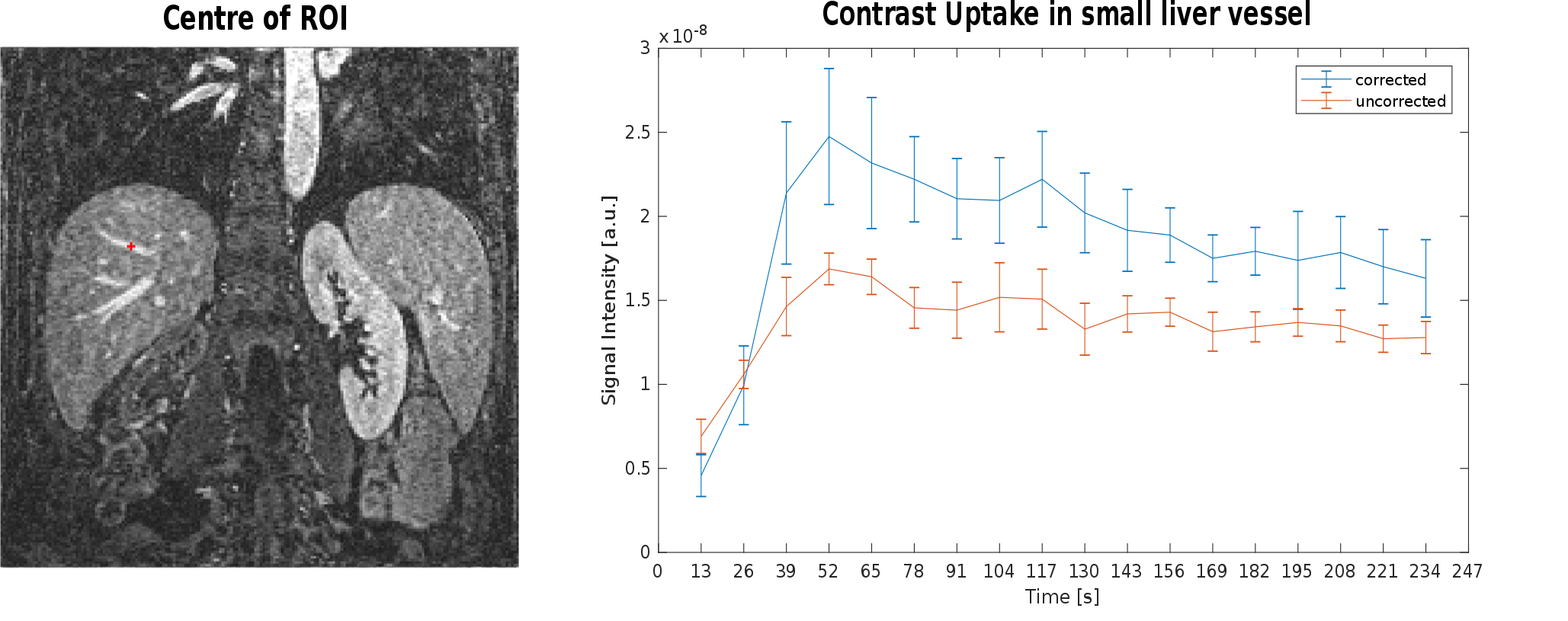
The respiratory resolved 3D images are shown in Fig. 2. The motion fields accurate describe the motion and deformation of the organs in the abdomen during respiration. Figure 3 compares the dynamic motion-corrected and the dynamic non-corrected images (abdominal coronal view). The motion-corrected images show a strongly improved contrast of vessels, small features and tissue interfaces compared to the non-corrected images. Figure 4 shows the dynamic contrast uptake of a ROI taken in a small liver vessel. The signal uptake in the motion corrected images is higher than the signal in the non-corrected images due to reduced motion-induced image blurring.Conclusion
The proposed motion correction technique provides dynamic 3D contrast enhanced images with high image quality, full abdominal coverage and high isotropic image resolution. The high temporal resolution could also allow for a fit of uptake parameters to obtain quantitative diagnostic information from the data. Respiratory self-navigator, 3D non-rigid motion information and kt-regularisation required for image reconstruction are all obtained from the same scan, making this approach highly efficient and easily applicable in clinical routine.Acknowledgements
No acknowledgement found.References
- Lin W, Guo J, Rosen MA, Song HK. Respiratory Motion-Compensated Radial Dynamic Contrast-Enhanced (DCE)-MRI of Chest and Abdominal Lesions. Magn Reson Med 2008;60:1135–1146.
- Zheng X, Xiao L, Fan X, Huang N, Su Z, Xu X. Free breathing DCE-MRI with motion correction and its values for benign and malignant liver tumor differentiation. Radiol Infect Dis 2015;2:65-71.
- Johansson A, Balter J, Cao Y. Motion-corrected image reconstruction of abdominal DCE-MRI images. Proc Intl Soc Magn Reson Med 2017;25:1295.
- Chandarana H, Feng L, Ream J, Wang A, Babb JS, Block KT, Sodickson DK, Otazo R. Respiratory Motion-Resolved Compressed Sensing Reconstruction of Free-Breathing Radial Acquisition for Dynamic Liver MRI. Invest Radiol 2015;50:749-756.
- Prieto C, Uribe S, Razavi R, Atkinson D, Schaeffter T. 3D Undersampled Golden-Radial Phase Encoding for DCE-MRA Using Inherently Regularized Iterative SENSE. Magn Reson Imaging 2010;64:514–526.
- Rueckert D, Sonoda LI, Hayes C, Hill DLG, Leach MO, Hawkes DJ. Nonrigid registration using free-form deformations: application to breast MR images. IEEE Trans Med Imaging 1999;18:712–721.
- Cruz G, Atkinson D, Buerger C, Schaeffter T, Prieto C. Accelerated motion corrected three-dimensional abdominal MRI using total variation regularized SENSE reconstruction. Magn Reson Med 2016;75:1484–1498.
- Tsao J, Boesiger P, Pruessmann KP. {k-t BLAST} and {k-t SENSE}: dynamic {MRI} with high frame rate exploiting spatiotemporal correlations. Magn Reson Imaging 2003;50:1031–1042.
Figures