0374
Clinical Feasibility Study of an Accelerated 3D Intracranial Magnetic Resonance Angiography Using Compressed-Sensing Algorithm1Department of Radiology, Peking University First Hospital, Beijing, China, 2Philips Healthcare, Beijing, China
Synopsis
Accelerated 3D intracranial magnetic resonance angiography(MRA) using Compressed-Sensing algorithm could be clinically valuable not only for improving the image quality and having almost the same diagnostic performance compared to conventional intracranial MRA, but also for reducing the scanning time which could improve the overall workflow of MRA imaging. It is a feasible protocol in intracranial MRA imaging.
Introduction
Magnetic resonance angiography (MRA) without contrast enhanced has been widely applied in clinical practice because of its completely noninvasive nature and detailed characterization of intracranial arterial diseases1-6. However, the relatively long scanning time (7~9 minutes in average) is the challenge for MRA so far. Therefore, more rapid time with high resolution of vascular visualization is needed for the MRA technique improvement. Recently, the application of a Compressed-Sensing (CS) algorithm7-8, which could improve the speed of MR imaging, has been attempted in some 3D examinations, such as magnetic resonance cholangiopancreatography (MRCP)9, knee joint10, and MRA11-13. Our purpose is to evaluate the clinical feasibility of 3D intracranial MRA using CS algorithm in intracranial arterial diseases.
Methods
From June 2017 to July 2017, 49 consecutive patients (19 males, 30 females, mean age: 52±18, age range: 10-84) with suspected intracranial arterial disease who had been referred for MRA examination in our hospital were included in our study. All the patients were examined utilizing both conventional MRA (Con-MRA) and CS accelerated 3D-MRA (CS-MRA) of intracranial artery on 3T MR system (Achieva TX; Philips, Best, the Netherlands) with a 32-channel head coil. Two radiologists (3 and 10 years of experience in neuroradiology, respectively) independently rated the image quality and assessed intracranial arterial lesions and variants of both CS-MRA and Con-MRA, respectively. Scores of 1, 2, 3, 4 and 5 were assigned to non-diagnostic, poor, fair, good, and excellent image quality respectively. The discrepancies of image quality and diagnosis between the two radiologists were resolved in consensus reading. In addition, the signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) of left middle cerebral artery (MCA) and basal artery in all patients were calculated for comparing the two techniques. The definition of external carotid artery system between Con-MRA and CS-MRA was also compared. Nonparametric test (Wilcoxon test) was performed to compare the image quality between Con-MRA and CS-MRA. The diagnostic agreement between Con-MRA and CS-MRA was evaluated by Kappa analysis. Paired-t-tests for SNR and CNR calculation were conducted to compare Con-MRA and CS-MRA. Nonparametric test (Wilcoxon test) was also performed to compare the definition of external carotid artery system between Con-MRA and CS-MRA.Results
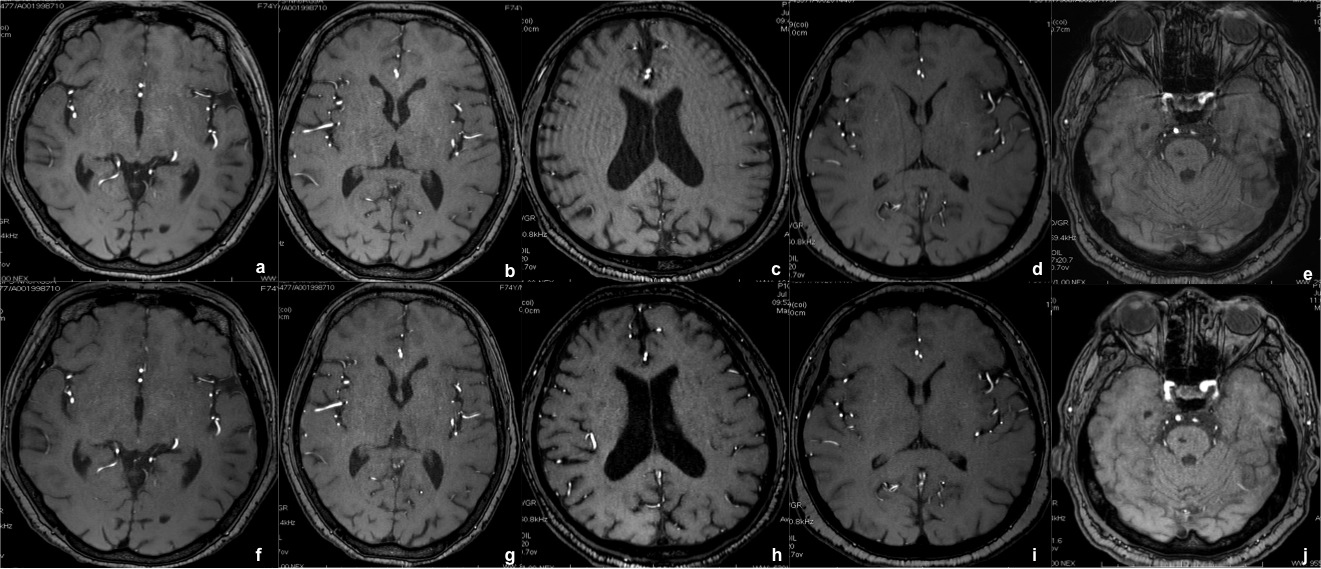
- The average scores for image quality gained significantly higher in CS-MRA compared to Con-MRA (4.51±0.58 for Con-MRA, 4.86±0.36 for CS-MRA, Z = -3.7, p < 0.001) (Figure 1).
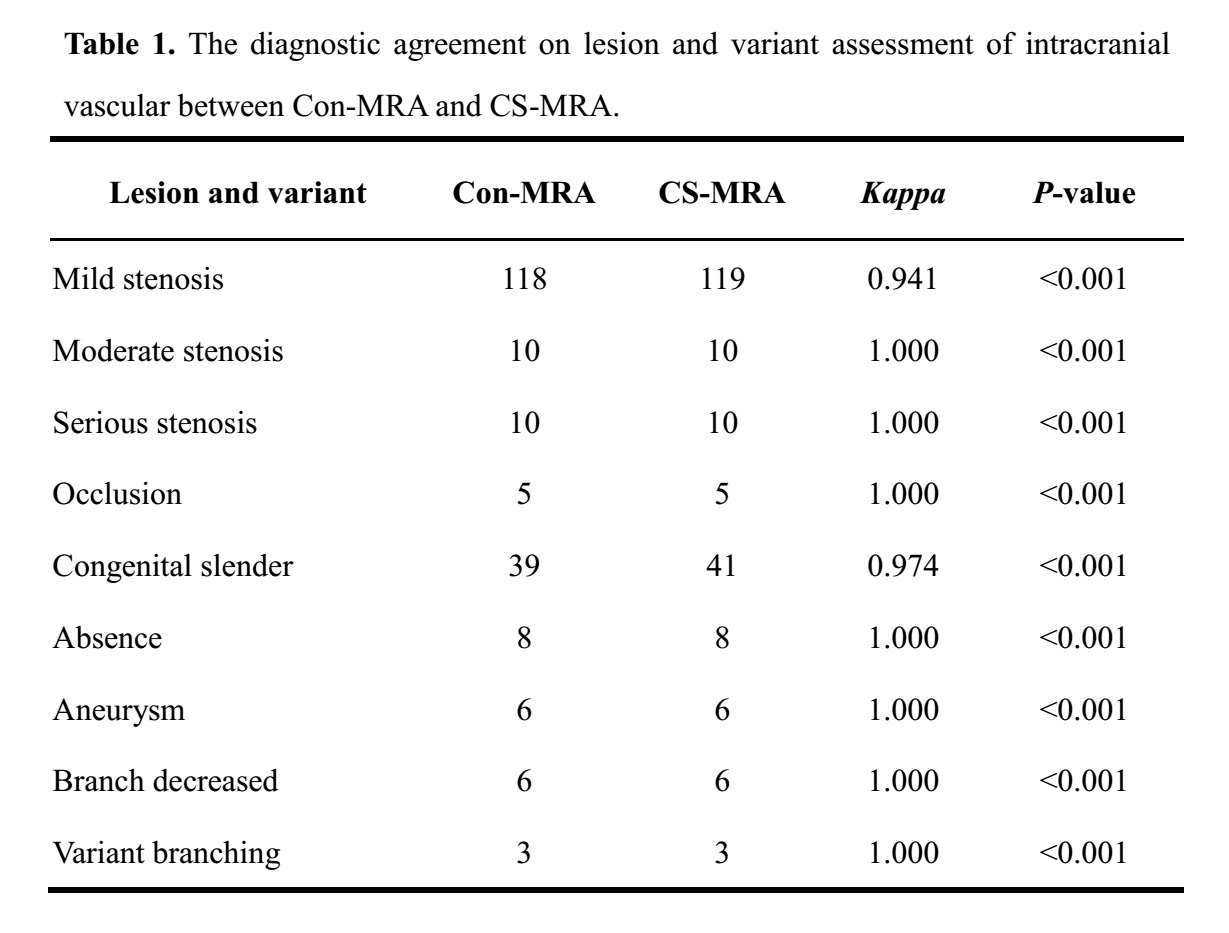
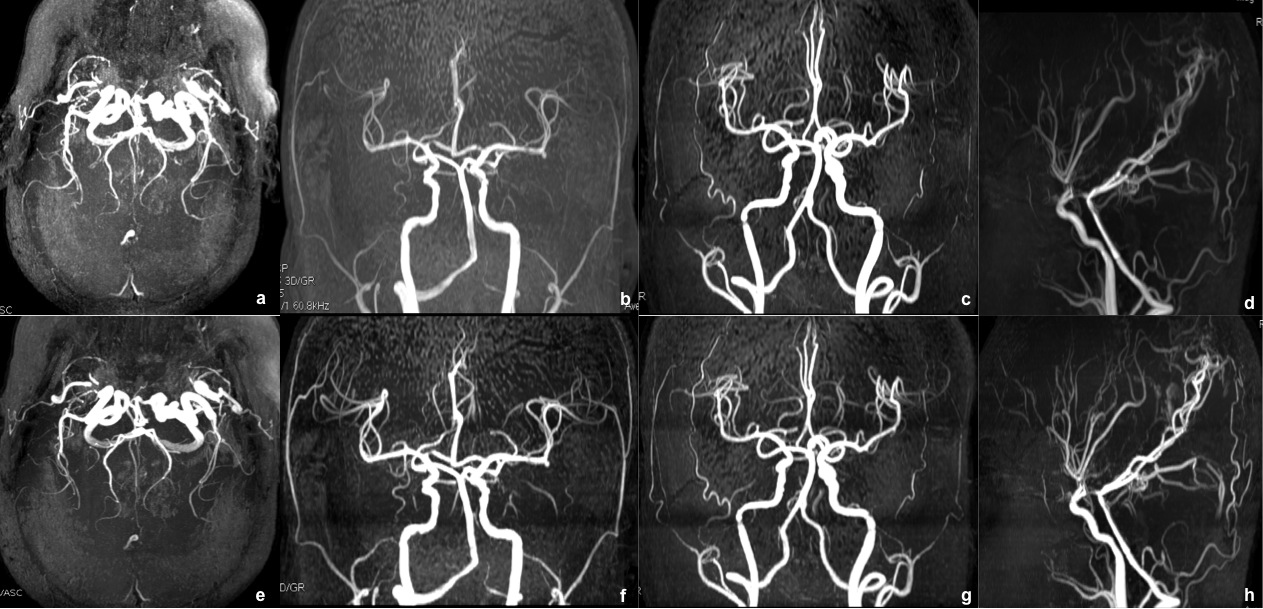
- The diagnostic agreement of intracranial arterial diseases between Con-MRA and CS-MRA showed a good (Kappa is above 0.9) agreement on lesion and variant assessment (Table 1 and Figure 2).
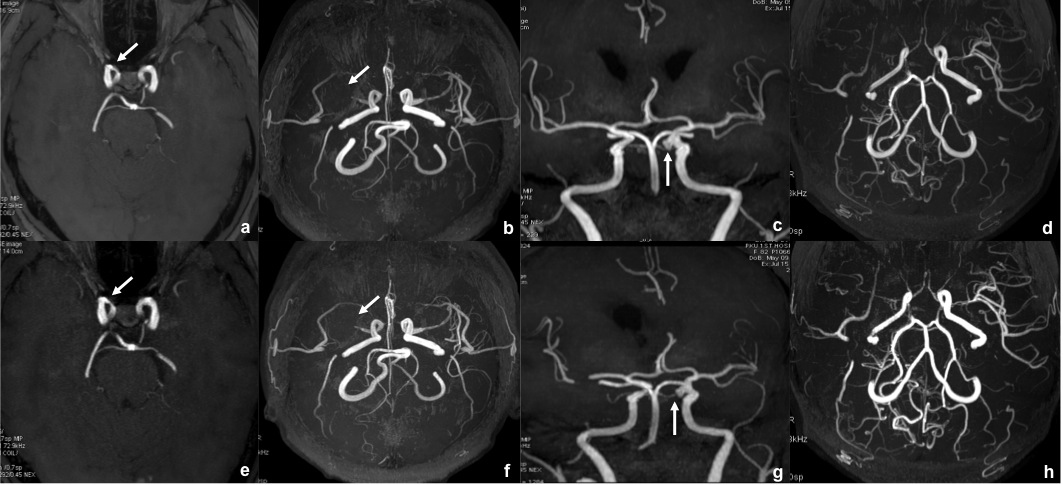
- The SNR and CNR of both left MCA and basal artery showed significantly higher in CS-MRA than Con-MRA (p < 0.001) (Figure 3).
- The definition of external carotid artery system was significantly better on CS-MRA images than on Con-MRA images (Con-MRA = CS-MRA: n=25; Con-MRA > CS-MRA: n=0; Con-MRA < CS-MRA: n=24; Z = -4.9, p < 0.001) (Figure 4).
Discussion
Our study showed the image quality, SNR and CNR of CS-MRA were preferable than those of Con-MRA with larger sample enrolled, and demonstrated that CS-MRA has a promising application in intracranial artery assessment. However, in our study, it was also vital that CS-MRA could offer almost the same diagnostic performance as Con-MRA in lesion and variant of intracranial artery. In addition, our study results found that CS-MRA could provide better images for detecting external carotid artery system, with more vascular structure visualized compared with Con-MRA. In our study, the mean acquisition time of CS-MRA in our study was less than 3min, whereas Con-MRA took nearly 6min. Scanning time was nearly 50% saved with CS-MRA. Moreover, CS-MRA was conducted successfully in all the patients enrolled in our study without any technical problem, which demonstrated its feasibility and stability, which was in accordance with previous studies11.Conclusion
In our study, CS-MRA showed significantly higher image quality with less image blurring, a comparable image diagnostic performance of internal carotid artery and vertebrobasilar artery system, and better visualization of external carotid artery system than Con-MRA. Moreover, CS-MRA with more rapid scanning time may be clinically valuable not only for improving the image quality but also for improving the overall workflow of intracranial MRA imaging.
Acknowledgements
No acknowledgement found.References
- Yan L, Wang S, Zhuo Y, Wolf RL, Stiefel MF, An J, Ye Y, Zhang Q, Melhem ER, Wang DJ. Unenhanced dynamic MR angiography: high spatial and temporal resolution by using true FISP-based spin tagging with alternating radiofrequency. Radiology 2010; 256: 270–279.
- Bi X, Weale P, Schmitt P, Zuehlsdorff S, Jerecic R. Non-contrastenhanced four-dimensional (4D) intracranial MR angiography: a feasibility study. Magn Reson Med 2010; 63: 835–841.
- Lanzman RS, Kropil P, Schmitt P, Wittsack HJ, Orzechowski D, Kuhlemann J, Buchbender C, Miese FR, Antoch G, Blondin D. Nonenhanced ECG-gated time-resolved 4D steady-state free precession (SSFP) MR angiography (MRA) of cerebral arteries: comparison at 1.5T and 3T. Eur J Radiol 2012;81:e531–e535.
- Raoult H, Bannier E, Robert B, Barillot C, Schmitt P, Gauvrit JY. Time-resolved spin-labeled MR angiography for the depiction of cerebral arteriovenous malformations: a comparison of techniques. Radiology 2014; 271: 524–533.
- Wu H, Block WF, Turski PA, Mistretta CA, Johnson KM. Noncontrast- enhanced three-dimensional (3D) intracranial MR angiography using pseudocontinuous arterial spin labeling and accelerated 3D radial acquisition. Magn Reson Med 2013; 69: 708–715.
- Willinsky RA, Taylor SM, TerBrugge K, Farb RI, Tomlinson G, Montanera W. Neurologic complications of cerebral angiography: prospective analysis of 2,899 procedures and review of the literature. Radiology 2003; 227: 522–528.
- Feng L, Benkert T, Block KT, Sodickson DK, Otazo R, Chandarana H. Compressed sensing for body MRI. J Magn Reson Imaging 2017; 45(4):966-987.
- Jaspan ON, Fleysher R, Lipton ML. Compressed sensing MRI: a review of the clinical literature. Br J Radiol. 2015; 88(1056): 20150487.
- Yoon JH, Lee SM, Kang HJ, Weiland E, Raithel E, Son Y, Kiefer B, Lee JM. Clinical Feasibility of 3-Dimensional Magnetic Resonance Cholangiopancreatography Using Compressed Sensing: Comparison of Image Quality and Diagnostic Performance. Invest Radiol. 2017; 52(10): 612-619.
- Garwood ER, Recht MP, White LM. Advanced Imaging Techniques in the Knee: Benefits and Limitations of New Rapid Acquisition Strategies for Routine Knee MRI. AJR Am J Roentgenol. 2017;209(3):552-560.
- Zhou Z, Han F, Yu S, Yu D, Rapacchi S, Song HK, Wang DJJ, Hu P, Yan L. Accelerated noncontrast-enhanced 4-dimensional intracranial MR angiography using golden-angle stack-of-stars trajectory and compressed sensing with magnitude subtraction. Magn Reson Med. 2017 May 7.
- Dautry R, Edjlali M, Roca P, et al. Interest of HYPR flow dynamic MRA for characterization of cerebral arteriovenous malformations: comparison with TRICKS MRA and catheter DSA. Eur Radiol. 2015; 25(11): 3230–3237.
- Stalder AF, Schmidt M, Quick HH, et al. Highly undersampled contrast-enhanced MRA with iterative reconstruction: Integration in a clinical setting. Magn Reson Med. Dec.2014
Figures