0371
ASL imaging and 31P/1H-MRS during prolonged breath-hold among experienced freedivers: Insights into cerebrovascular and metabolic responses1Department of Radiology, University Hospital Bonn, Bonn, Germany, 2Department of Radiology, University Medical Center Utrecht, Utrecht, Netherlands, 3Sunnybrook Research Institute, University of Toronto, Toronto, ON, Canada, 4Radiology Department, Amsterdam Medical Center, Amsterdam, Netherlands, 5Department of Anesthesiology, University Hospital Bonn, Bonn, Germany, 6Philips Healthcare, Bonn, Germany, 7Philips Healthcare, Best, Netherlands, 8Spinoza Centre for Neuroimaging, Amsterdam, Netherlands, 9Institute of Radiopharmaceutical Cancer Research, Helmholtz-Zentrum Dresden-Rossendorf, Dresden, Germany
Synopsis
This pCASL and 31P/1H-MRS study explored the cerebrovascular reactivity (CVR) and its efficacy on brain metabolic stability during a five-minute breath-hold in fifteen experienced freedivers. Cerebral blood flow (CBF) increase occurred later than the decrease of the recently discovered arterial transit time correlate, spatial CoV. The latter may thus be an early CVR biomarker. CBF varied between vessel territories, gray and white matter and usually lowered with more experience. MRS showed near stable physiological cerebral pCr, ATP and pH concentrations despite peripheral lactate acidosis. In conclusion, this trial revealed that CVR sufficiently compensates the metabolic challenge of a five minute breath-hold.
In conclusion, this trial revealed that cerebral perfusion increase sufficiently compensates the metabolic challenge of a five-minute breath-hold.
Introduction
Due to training and adaptive physiology, experienced freedivers can perform breath-holds of several minutes1,2, yielding hypoxemia conditions. They are therefore ideal subjects to investigate the physiological cerebrovascular reactivity (CVR) needed to maintain brain energy metabolism in breath-hold. Detailed knowledge on this topic is scarce, despite frequent clinical circumstances such as failing intubation. Arterial spin labeling (ASL) allows an absolute cerebral blood flow (CBF) imaging. Use of the spatial coefficient of variation of CBF (ASL-sCoV) parameter may be used to estimate the arterial transit time (ATT), as described recently3. Prolonged breath-hold responses can also be assessed by 31P- and 1H-MR spectroscopy (MRS), which provide cerebral ATP, pH and lactate data. The present study explores the perfusion response and its efficacy during prolonged breath-hold in an experienced freediver cohort with special regard to the influence of chronic adaptation.Methods
Fifteen male freedivers (mean age 39.9±12.4 years) participated (Fig. 1). Lifetime experience with prolonged breath-hold was estimated by interview. Oxygen saturation (SpO2) and heart rate (HR) were continuously monitored. Venous pH, lactate, O2 and CO2 were determined before, during and after breath-hold. The 3T MRI protocol consisted of a structural 1mm3 3D T1w sequence followed by five pseudo-continuous ASL scans of 2.5 mins. each (FOV 240x240x96 mm3, TE/TR 8ms/4280ms, LD 1800ms, PLD 2000ms): a baseline scan before breath-hold, early and late phases during a 5 min. breath-hold, early and late phases of immediately following 5 min. recovery. Data was processed by ExploreASL software described elsewhere4,5. ASL-sCoV was defined as the standard deviation of CBF divided by the mean CBF, within the total gray matter (GM; pGM>0.7)3 :
ASL-sCoVROI = σ (CBFGM)/µ(CBFGM)* 100%
After 1h rest 11/15 freedivers underwent volume-selective 31P-MRS (25mm axial slice of basal ganglia) before, during, and after a 5 min. breath-hold (dual-tunable 31P/1H birdcage transmit/receive head coil, TR 4s, 4 signal averages). MRS data were processed with AMARES algorithm quantifying phosphocreatine (PCr), inorganic phosphates (Pi) and nucleotide triphosphates (ATP) peaks. pH was determined from the frequency separation between Pi and PCr. The time course of pH and ratios Pi/PCr, Pi/ß-ATP, PCr/ß-ATP were analyzed. Later a single-volume 1H-MRS measurement (TR/TE 2000/140ms) in the basal ganglia of 8/11 divers was performed before and during breath-hold for lactate detection (only detectable if pathologically elevated). Statistics involved paired t-tests and mixed linear models with subject as a random factor.
Results
CBF increase from baseline increased during the second 2.5 minutes of breath-hold (mean +51.8% late phase/baseline vs. +17.8% during early phase; p<.0001; Fig. 2). CVR of the anterior circulation was consistently higher than in the posterior circulation (p=.001). CVR differed between GM and white matter (WM; p=.0001). Different from CBF, ASL-sCoV decreased by >25% during early breath-hold (mean: -30.0±21.6%; p=.002). It remained reduced until recovery. The between-subject range of GM ASL-sCoV was smaller during breath-hold, than during breathing (baseline: mean 2.8±1.0%; vs. early breath-hold: mean 1.8±0.4; p=.02). SpO2 was correlated to CVR (p=.0001), while HR and age were not. For 13/15 cases a relationship between greater previous apnea experience and lower CBF was identified (p=.01). ASL-sCoV was not linked with SpO2, HR, age or experience. Cerebral pH and lactate did not significantly shift towards pathological values (Fig. 3A), while blood analysis showed lactic acidosis and hypoxemia/hypercapnia (Fig. 3B). However, minor PCr and ß-ATP differences to baseline were positively correlated to differences in pH (R=0.44, p=.003 for PCr, and R=0.47, p=.002 for ß-ATP; Fig. 3C).Discussion and Conclusion
This
combined ASL and MRS trial revealed that breath-hold induced CVR is not only
selective for GM to WM, but the adaptive response appears to cerebral metabolic
markers stable despite extreme respiratory distress. These findings under
room air conditions have relevance for patient safety in clinical emergency
situations. ASL-sCoV further showed dynamics suggestive of its capacity to
monitor ATT in breath-hold experiments. The lower maximum CBF increase in this
study compared to results in similar Doppler ultrasonography experiments
confirm a limited comparability of these techniques6,7. This trial also
revealed an association of lower CBF with greater previous breath-hold
experience, which can plausibly be explained by adaptation of the
cerebrovascular system, but needs further evaluation in larger cohorts.
Acknowledgements
No acknowledgement found.References
1. AIDA World records. https://www.aidainternational.org/AthleteDetails?athleteId=00000000-0000-0000-0000-000000000013. Accessed Nov 2, 2017
2. Eichhorn L, Erdfelder F, Kessler F, et al. Evaluation of near-infrared spectroscopy under apnea-dependent hypoxia in humans. J Clin Monit Comput. 2015;29(6):749-757.
3. Mutsaerts HJ, Petr J, Vaclavu L, et al. The spatial coefficient of variation in arterial spin labeling cerebral blood flow images. J Cereb Blood Flow Metab. 2017:271678X16683690.
4. Ashburner J. A fast diffeomorphic image registration algorithm. Neuroimage. 2007;38(1):95-113. 5.
5. Mutsaerts HJ, Lysvik E, Schrantee A, et al. ExploreASL: image processing toolbox for multi-center arterial spin labeling population analyses. Paper presented at: ESMRMB2017; Barcelona, Spain.
6. Cross TJ, Kavanagh JJ, Breskovic T, et al. Dynamic cerebral autoregulation is acutely impaired during maximal apnoea in trained divers. PLoS One. 2014;9(2):e87598.
7. Willie CK, Ainslie PN, Drvis I, et al. Regulation of brain blood flow and oxygen delivery in elite breath-hold divers. J Cereb Blood Flow Metab. 2015;35(1):66-73.
Figures
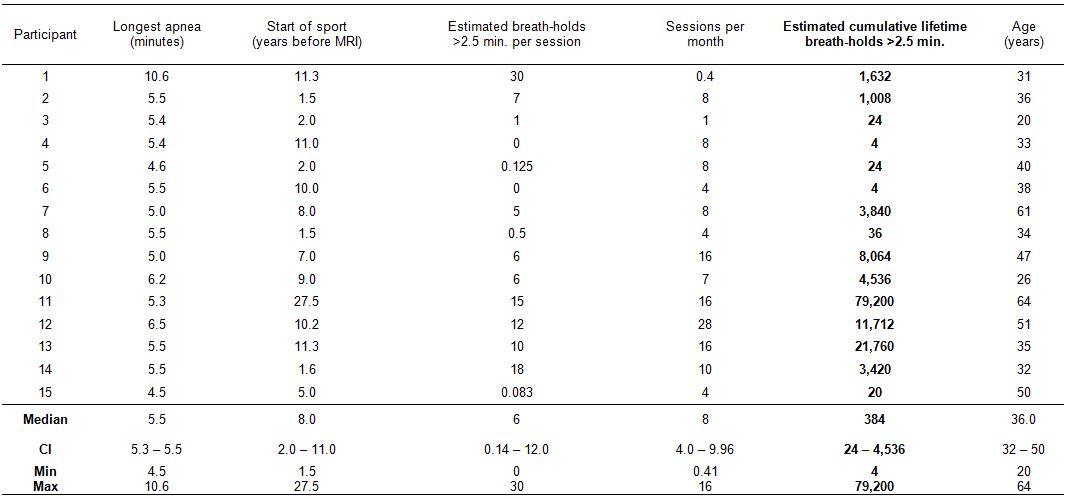
Table 1 Data of freediver cohort
Participants were interviewed concerning the duration (start of sport) and intensity (sessions per month) and the estimated frequency they keep breath for longer than 2.5 minutes per session. The latter could be below 1 if prolonged apnea only occurred very infrequently. Some participants held breath for longer than 2.5 minutes only as a qualification for this study, hence their cumulative lifetime breath-holds longer 2.5 minutes before MRI was four, while others very frequently underwent prolonged apnea.
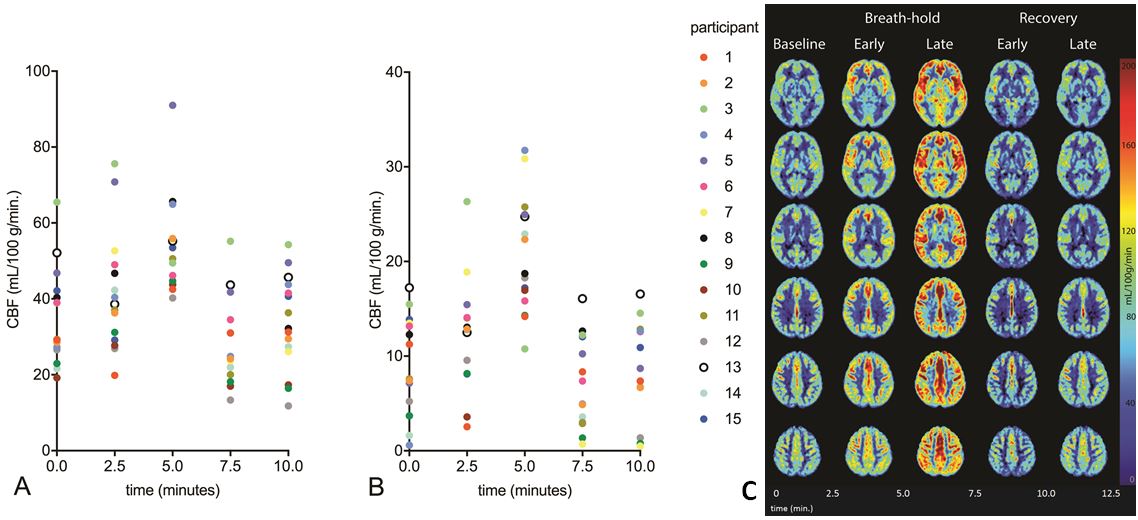
Fig. 2 Cerebral blood flow dynamics in gray and white matter
A: CBF measured for the five different time points, of which the second and third being during breath-hold. Gray matter voxels only (n=15 participants; each represented by a color dot).
B: The same for white matter voxels only.
C: False color map illustration of CBF dynamics in selected transverse brain sections of the cohort mean CBF before, during and after the five minute breath-hold challenge.
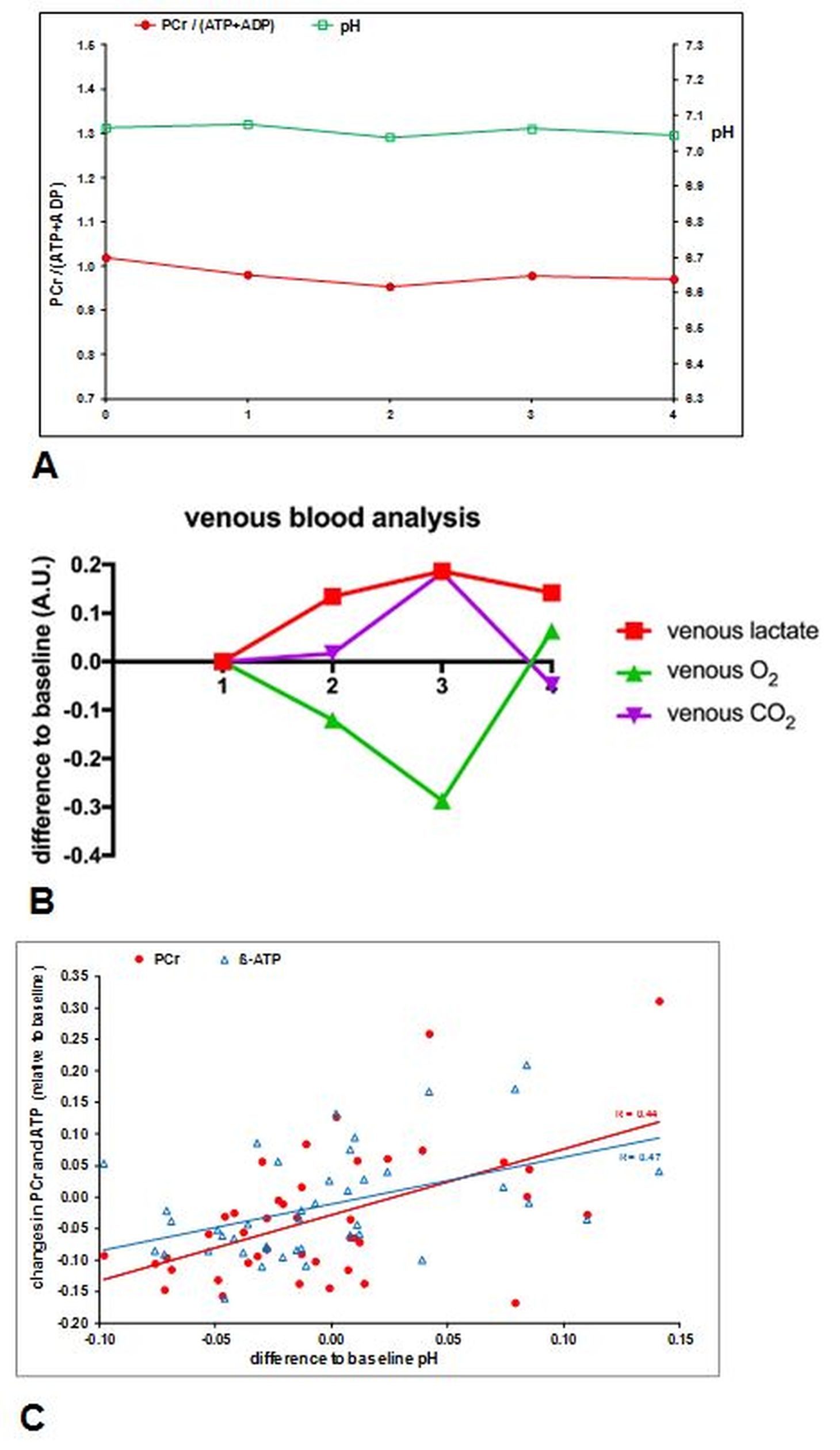
Fig. 3 Comparison of metabolic dynamics in brain (MRS) and periphery (venous blood gas)
A: MR spectroscopy revealed that cerebral high-energy metabolites (here expressed by PCr/(ATP+ADP)) and pH remained physiologically constant during 5-minute breath-hold
B: On the other hand peripheral venous lactate accumulation as well as hypoxemia and hypercarbia were observed during breath-hold.
C: The comparison of the minor differences to baseline values however revealed significant correlations between PCr and pH and between ATP and pH