0364
Subtle changes in hyperelastic properties of myocardium with cardiotoxicity remodeling from CMR1Mechanical Engineering, Polytechnique Montreal, Montreal, QC, Canada, 2Biomedical Engineering, University of Auckland, Auckland, New Zealand, 3Anatomy with Radiology, University of Auckland, Auckland, New Zealand, 4Kinesiology, University of Montreal, Montreal, QC, Canada
Synopsis
The aim of this study was to assess subtle changes in 3D geometrical and mechanical properties of left ventricle in childhood acute lymphoblastic leukemia survivors. Global 3D volume or ejection fraction were not sensitive enough while time dependent 3D geometrical parameters over the cardiac cycle showed that early diastole is more affected than systole or late diastole. Smaller hyper-elastic properties were found in the high risk group than in the standard risk, high risk with cardioprotective agent or healthy volunteers group. High temporal resolution and local parameters would improve the detection of these subtle changes.
Introduction
Doxorubicin-based chemotherapy is
effective and widely used to treat acute lymphoblastic leukemia (ALL). However,
its effectiveness is hampered by a wide spectrum of dose-dependent
cardiotoxicity [1], including both morphological and functional changes
affecting the myocardium. The feasibility of cardiac magnetic resonance (CMR)
has been established and several software for 3D geometrical modeling of the
left ventricle were developed to assess ejection fraction, end-systolic and
end-diastolic volumes, and wall thicknesses [2]. Finite element models and
inverse material parameters identification strategies
were then introduced
to take into account the passive or active mechanical behavior of the
myocardial tissue [3]. The objective of this study was to assess the subltle
changes in 3D geometrical and mechanical properties of left ventricle in
childhood ALL survivors.Methods
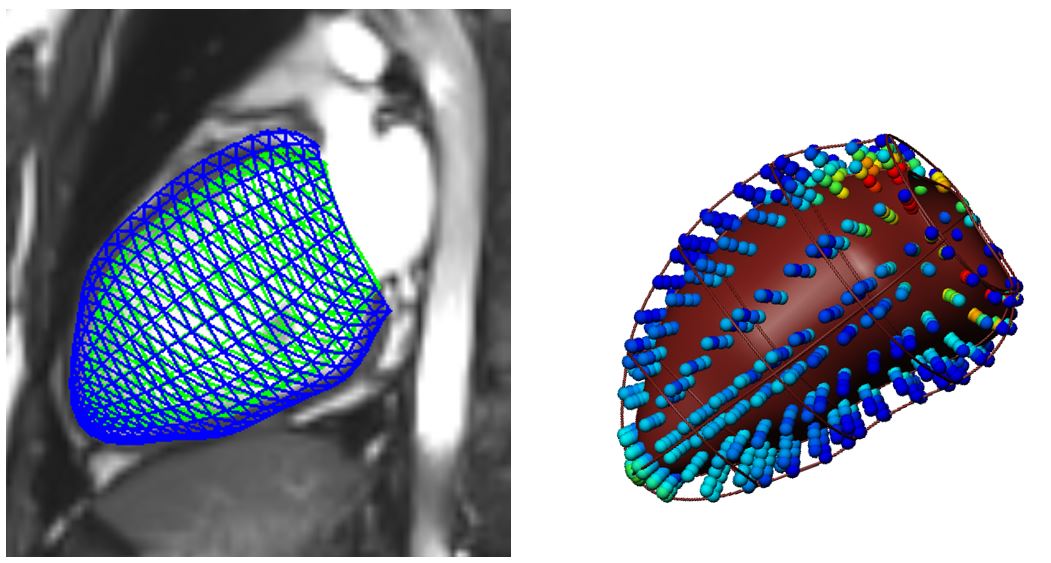
Eighty-six ALL survivors (23±7 years old) were prospectively included and divided into 3 groups according to their prognostic risk: standard risk (SR, n=19), high risk (HR, n=31) and high risk group who received dexrazoxane, a cardioprotective agent (HRdex, n=36). Healthy subjects (n=10, 22±4 years old) from an in-house study were also included. They all underwent a CMR acquisition including an ECG-gated cine TruFISP sequence at 3T (Siemens SkyraTM) using a 18-channel phased array body matrix coil. Sequence parameters were slice thickness 8mm, repetition time 34.6ms, effective echo time 1.2ms, flip angle 38°, iPAT factor 3, matrix 208x210 and in-plane pixel size 1.25x1.25 mm. Approximately 14 slices were acquired in short axis and 3 to 4 slices in long axis. For each slice, 25 phases of the cardiac cycle were acquired during multiple breath-holds. The left ventricle contours were semi-automatically drawn from six points located by the operator (apex, base center, right ventricular insertions and baseplane markers) and manually corrected for mis-registration (CIM v8.1, University of Auckland, [4]). Repeatability was quantified by intra-class coefficients (ICC) on 3 reconstructions of 15 subjects, each by 4 operators. For half of the volunteers from each group, a 3D finite element model [5] was used to calculate the hyper-elastic property (C1) from inverse materials parameters identification strategies based on the CMR ventricle geometry at diastasis (Figure 1). Three simulations were proposed with 3 different applied pressures (0.75, 1 and 1.25kPa). C1 was reported and compared between groups for each applied pressure. The comparison between groups was done using one-way ANOVA on global parameters and two-ways ANOVA for repeated measures on time dependent parameters.Results
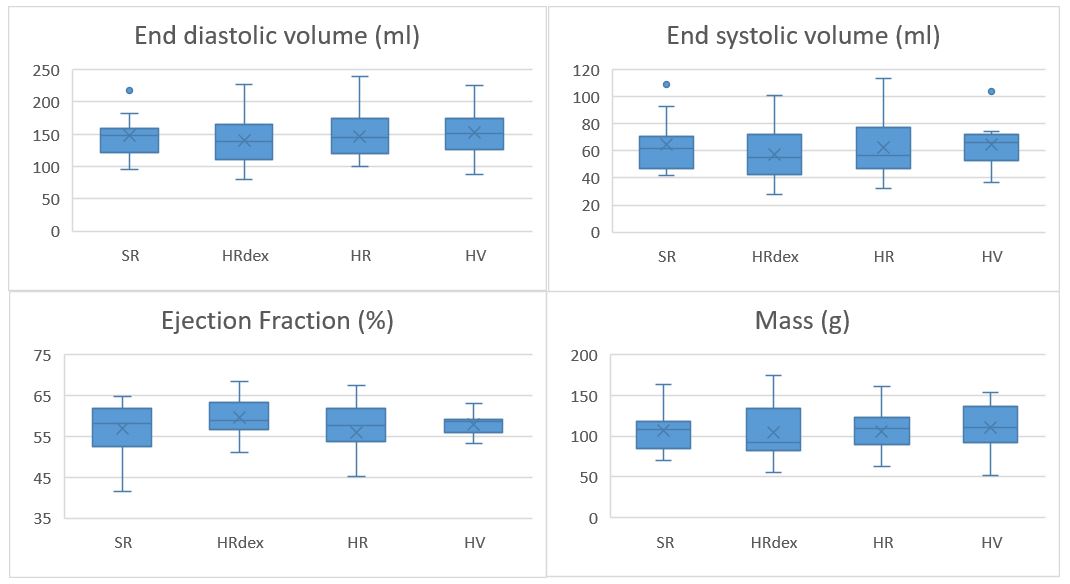
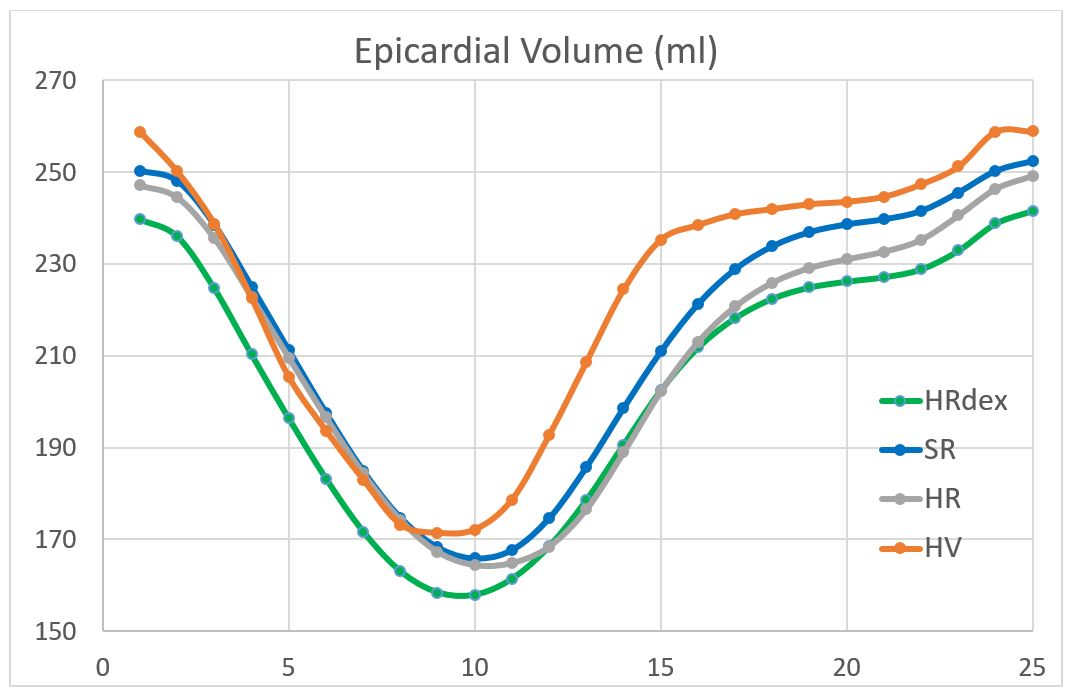
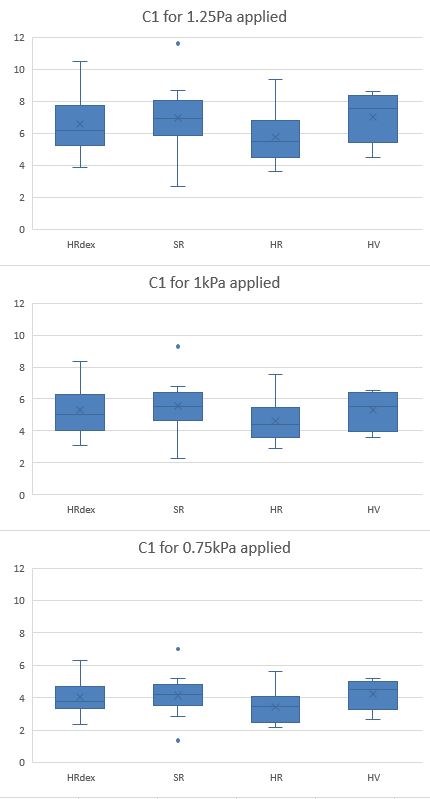
Inter-observer repeatability was good (ICC 0.60-0.74) for 3D regional parameters and excellent (ICC 0.75-1.00) for 3D global parameters while intra-observer repeatability was excellent for both regional and global parameters (ICC 0.75-1.00). No differences were observed on end-systolic or end-diastolic volumes, stroke volume, ejection fraction nor mass (Figure 2, p>0.4). Some differences were observed on epicadium volume only between end systole and diastasis (frames 11-16 on Figure 3, p<0.01) between HRdex and HV or SR, and between HV and HR. The hyper-elastic property C1 was slightly smaller (p=0.041) for the HR group as compared to the HRdex or SR group, and also as compared to the HV group (Figure 4).Discussion
The global 3D parameters such as volume or ejection fraction are not sensitive enough to the subtle changes due to doxorubicin induced cardiotoxicity. However, the time dependent 3D geometrical parameters over the cardiac cycle suggested that early diastole is more affected by doxorubicin induced cardiotoxicity than systole or late diastole. The smaller hyper-elastic property in the HR group suggested a myocardium tissue more prone to dilatation if increased intra-ventricular pressure is applied than the HV, SR or HRdex groups, in agreement with well-known observed late cardiotoxicity effects for large doses of doxorubicin in adults. However, the real intra-ventricle pressure was not included in the 3D finite element model as the direct measure is invasive and not feasible on young clinically healthy adults. Thus the mechanical behavior quantified in this study is limited to geometrical effects. Although, the finite element simulations on the healthy subjects presented higher mean standard errors in the optimization process due to less CMR slices acquired than for the cancer survivors.Conclusion
Subtle changes in myocardium remodeling due to childhood cardiotoxicity can be assessed from the mechanical behavior analysis of the left ventricle on CMR images. Temporal resolution should be improved in CMR of cancer survivors to detect these subtle changes, and local geometrical parameters should be included in the analysis. The next step will be to evaluate the real applied intra-ventricle pressure from incremental exercise tests and a numerical lumped parameter model.Acknowledgements
NSERC and Polytechnique Montreal for the financial support, researchers from the PETALE study for the opportunity to do this complementary analyses on the cancer survivors.References
1- Migrino RQ, Aggarwal D, Konorev E, Brahmbhatt T, Bright M, Kalyanaraman B. (2008). Early detection of doxorubicin cardiomyopathy using two-dimensional strain echocardiography. Ultrasound Med Biol. 34(2):208-14.
2- Suinesiaputra A, Cowan BR, Al-Agamy AO, AlAttar MA, Ayache N, Fahmy AS, Khalifa AM, Medrano-Gracia P, Jolly M-P, Kadish AH, Lee DC, Margeta J, Warfield SK, Young AA. 2014. A Collaborative Resource to Build Consensus for Automated Left Ventricular Segmentation of Cardiac MR Images. Med Image Anal. 18(1). doi:10.1016/j.media.2013.09.001.
3- Wang VY, Nielsen PMF, Nash MP. Image-Based Predictive Modeling of Heart Mechanics. Annu. Rev. Biomed. Eng. 2015. 17:351–83.
4- Li B, Liu Y, Cowan BR, Young AA. (2010) In-line automated tracking for four dimensional ventricular function with magnetic resonance imaging. J Am Coll Cardiol Img 3, 860-866.
5- Wang VY, Lam HI, Ennis DB, Cowan BR, Young AA, Nash MP. Modelling passive diastolic mechanics with quantitative MRI of cardiac structure and function. Med Image Anal. 2009 Oct;13(5):773-84.
Figures