0351
Rapid Synthetic MRI of the whole brain using simultaneous multi-slice technique1Global MR Applications & Workflow, GE Healthcare, Menlo Park, CA, United States, 2Global MR Applications & Workflow, GE Healthcare, Waukesha, WI, United States, 3SyntheticMR, Linköping, Sweden
Synopsis
Synthetic MRI enables reconstruction of multiple MRI contrasts from a single scan based on voxel-wise computation of relaxation parameters. This can improvement scan productivity and workflow considerably. The utility of synthetic MRI has recently been demonstrated in clinical settings. However in its current implementation whole brain coverage can be achieved within 5 minutes only if a thick slice prescription (~ 4mm) is used, but this might provide insufficient through-plane resolution for certain clinical protocols and can also lead to partial voluming effects. This work explores the simultaneous multislice approach for more efficient through plane coverage with synthetic MRI.
Purpose:
Synthetic MRI enables reconstruction of multiple MRI contrasts from a single scan based on voxel-wise computation of relaxation parameters such as T1, T2, PD. It can be a very flexible tool for scan productivity and workflow enhancement [1-2]. The benefits of Magnetic Resonance Image Compilation (MAGiC), a synthetic MR based technique in which the parameters are fitted to data from a multi saturation delay multi echo (MDME) 2D fast spin echo (FSE) acquisition [3,4] has been recently demonstrated in clinical settings [5,6]. In its current implementation, whole brain coverage be achieved in around 5 minutes only if a thick slice prescription (slice thickness ~ 4 mm , slice gap ~ 1mm) is used but this might be insufficient in terms of through-plane resolution for certain clinical protocols and might lead to potential partial voluming artifacts. This work explores the simultaneous multislice (SMS) approach [7-8] for more efficient through plane coverage with synthetic MRI.Method:
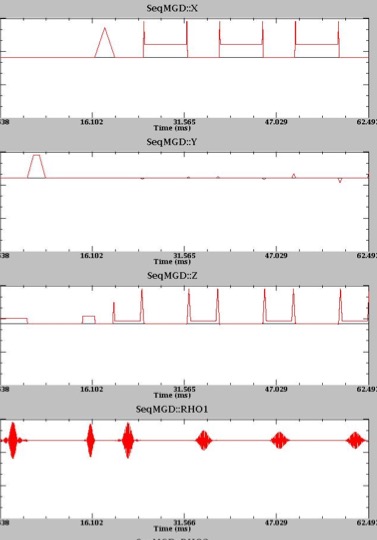
The above mentioned MDME sequence employed in MAGiC is a 2D Fast spin echo (FSE) sequence acquired at multiple saturation delay times and multiple spin echo times, providing a collection of images with different tissue contrast weighting. The saturation delay times are varied between the acquisition phases by changing the offset between the saturated and the excited-then-refocused slice. SMS capability was incorporated into the sequence by modulating the conventional single slice-selective saturation, excitation and refocusing pulses to convert them into multiband. A plot of the sequence waveforms in shown in Figure 1. MAGiC Brain MRI was acquired in 2 volunteers with informed consent in accordance with IRB guidelines of the site on a 3T scanner (GE MR 750 Waukesha, WI) using 32 channel array and the following scan parameters: FOV=24x19.2cm, BW=22.7 KHz, 4 saturation delays, 2 echoes, in-plane resolution: 0.75x0.75 mm2, slice thickness/slice gap: 2.5/1 mm, 42 slices, scan time=5:19 s for SMS factor = 2, and 8’47” for SMS factor = 1. The conventional MDME sequence was also run with the currently used protocol using slice thickness/slice gap: 4/1 mm, 29 slices, scan time = 6’4”. Spin parameters were extracted from the MDME sequence by fitting the T1 recovery curve to the different delay times and T2 decay to the different echo times, and scaling the curves to determine PD, on a voxel by voxel basis and images with multiple different contrast weightings such as T1, T2, T2 FLAIR, Double Inversion Recovery (DIR), phase sensitive IR (PSIR) were synthesized, all through an automated pipeline without user intervention (SyntheticMR Linköping, Sweden) [1].
Results and Discussion:
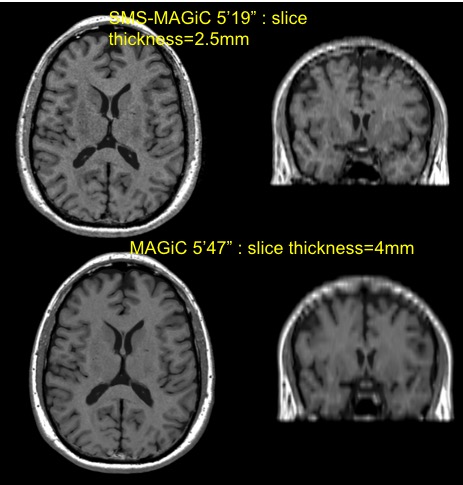
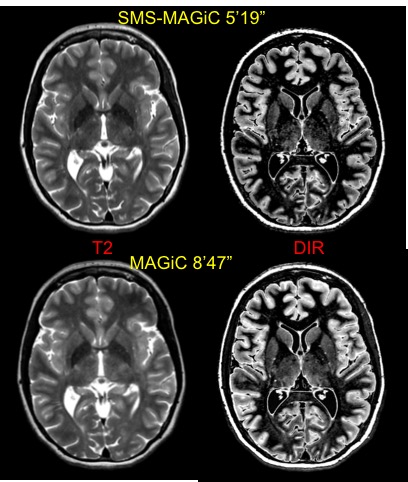
Synthetic T1 images in the acquired axial plane and coronal reformats derived from SMS-MAGiC (slice thickness=2.5mm) and the conventional MAGiC acquisition (slice thickness=4 mm) which had approximately the same scantime are shown in Figure 2. The SMS-MAGiC images are slightly noisier, as would be expected but the higher through-plane resolution of SMS-MAGiC can be appreciated in the coronal reformat. Synthetic images derived from the prescription-matched thin slice conventional MAGiC and the SMS-MAGiC sequences had comparable image quality (Figure 3) even though the scan time was 60% shorter for the SMS acquisition. However, we observed some oscillations in CSF in intermittent slices of the SMS images which will have to be investigated further. This effect was most pronounced in the synthesized T2 FLAIR contrast. We hypothesize that residual aliasing from superimposed slices might be causing the oscillatory signal. Compared to EPI, the adoption of SMS in FSE sequences have been limited [9-10] mostly due to the higher power requirement of SMS RF pulses, FSE being typically SAR-limited. However, MDME is a relatively good SMS candidate since its lower limit of TR is dictated by saturation recovery considerations.Conclusion:
This work incorporated SMS into a 2D Synthetic MRI technique to improve its through-plane coverage efficiency. Previously in plane time-interleaved and other acceleration methods have been explored [4]. Synthetic MRI can be a great scan productivity tool providing radiologists access to additional contrast-weightings from a single scan, and potentially providing an opportunity to classify pathology based on multiple parameters. Any method for further speeding up this technique without compromising the accuracy of parameter fitting or image quality would make it even more useful in clinical settings.Acknowledgements
No acknowledgement found.References
1. Warntjes JB et al, Rapid Magnetic Resonance Quantification on the Brain Optimization for Clinical Usage, Magn Reson Med 2008; 2:320-9. 2. Warntjes JB et al, Novel Method for Rapid, Simultaneous T1, T*2, and Proton Density Quantification, Magn Reson Med 2007, 3. Hwang KP et al, Fat-water separation in a rapid quantitative mapping sequence, ISMRM 22nd Annual Meeting, Milan, Italy, 2014, #3201 4. Banerjee S et al, Single Acquisition multiple contrast spine MRI using accelerated quantitative mapping, ISMRM 24th Annual Meeting, Singapore, 2016, #4393 5. Granberg , Uppman M et al, Clinical Feasibility of Synthetic MRI in Multiple Sclerosis: A Diagnostic and Volumetric Validation Study, AJNR Am J Neuroradiol. 2016;37(6):1023-9. 6. Tanenbaum LN et al, Synthetic MRI for Clinical Neuroimaging: Results of the Magnetic Resonance Image Compilation (MAGiC) Prospective, Multicenter, Multireader Trial, Am J Neuroradiol 2017: Jun;38(6):1103-1110 7. Barth M et al, “Simultaneous Multislice (SMS) Imaging Techniques”, Magn Reson Med 2016; 75:63-81. 8. Setsompop k et al, “Blipped controlled aliasing in parallel imaging for simultaneous multi-slice imaging with reduced g-factor penalty”, Magn Reson Med 2012; 67:1210-1224. 9. Gagoski BA, Bilgic B, Eichner C, Nhat H, Grant PE, Wald LL, Setsompop K, “RARE/turbo spin echo imaging with simultaneous multislice Wave-CAIPI”, Magn Reson Med 2015; 73:929-938. 10. Wang D et al “ Improving slice resolution of knee imaging using multiband slice accelerated TSE”, Proc Intl Soc Mag Reson Med 23 (2015); 4164.Figures