0347
Diagnostic Comparison of Two Rapid Knee MRI Protocols for Comprehensive Whole-Joint Assessment: A Multi-Reader Feasibility Study1Radiology, Stanford University, Palo Alto, CA, United States, 2Harvard Medical School, Stanford, MA, United States, 3Radiology & Nuclear Medicine, Erasmus Medical Center, Rotterdam, Netherlands
Synopsis
There were approximately 1.25 million clinical knee magnetic resonance imaging (MRI) scans performed in the US annually. Most knee MRI protocols require approximately 30 minutes of scan time. However, there is interest in expedited imaging protocols, especially under the ISMRM Value Initiative. Through a study involving 35 patients and 5 readers, we have demonstrated the feasibility of (1) a single 5-minute DESS sequence and (2) a 5-minute DESS sequence paired with a 2-minute coronal PDFS sequence, as two potential methods for accurate, rapid, and comprehensive diagnostic whole-joint knee MRI.
Introduction
There are approximately 1.25 million clinical knee magnetic resonance imaging (MRI) scans performed in the US annually1-2. Most knee MRI protocols require approximately 30 minutes of scan time. However, there is interest in expedited imaging protocols, especially under the ISMRM Value Initiative. This exploratory study compared the whole-joint diagnostic performance of (1) a single 5-minute 3D double-echo in steady-state (DESS) sequence, and (2) a 5-minute DESS sequence paired with a 2-minute coronal proton-density fat-saturated (PDFS) sequence, to that of a routine knee MRI protocol.Methods
The DESS sequence samples two 3D echoes. The first echo (S+) has a T1/T2 weighting (similar to a proton-density (PD) weighting), while the second echo (S-) has an additional T2 weighting4–6. While many DESS methods (most commonly the Siemens product) combine these echoes into a single image, the sequence in this work reconstructs echoes separately, generating multiple contrasts and simultaneous T2 maps generation7,8. The high SNR-efficiency of DESS enables high-resolution multi-planar reformatting (MPR) in rapid scan times9,10.
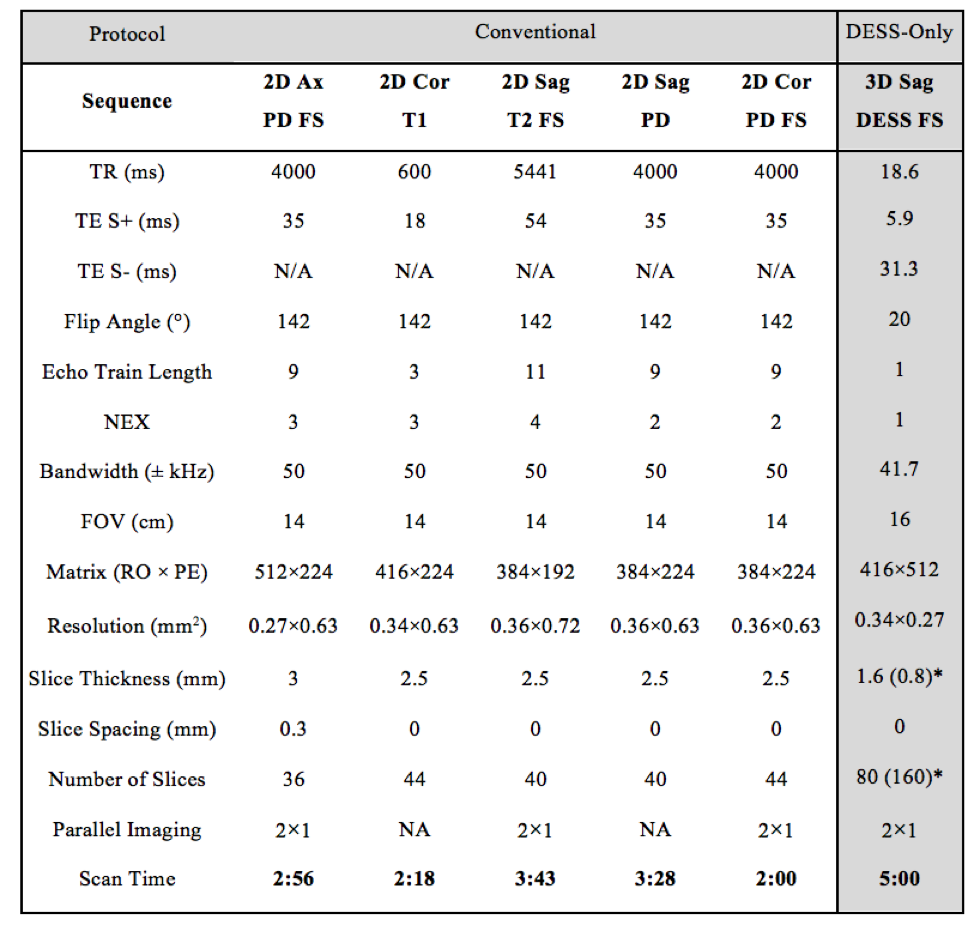
Thirty-five symptomatic patients (18 male, 17 female, age 43±19 years) referred for a routine knee MRI were scanned on one of two identical Discovery MR750 3.0T MRI scanners (GE Healthcare, Waukesha, Wisconsin) with an 8-channel transmit-receive knee coil (InVivo, Gainesville, Florida). A water-excitation sagittal 3D DESS sequence was added to the routine knee protocol (scan parameters in Fig. 1).
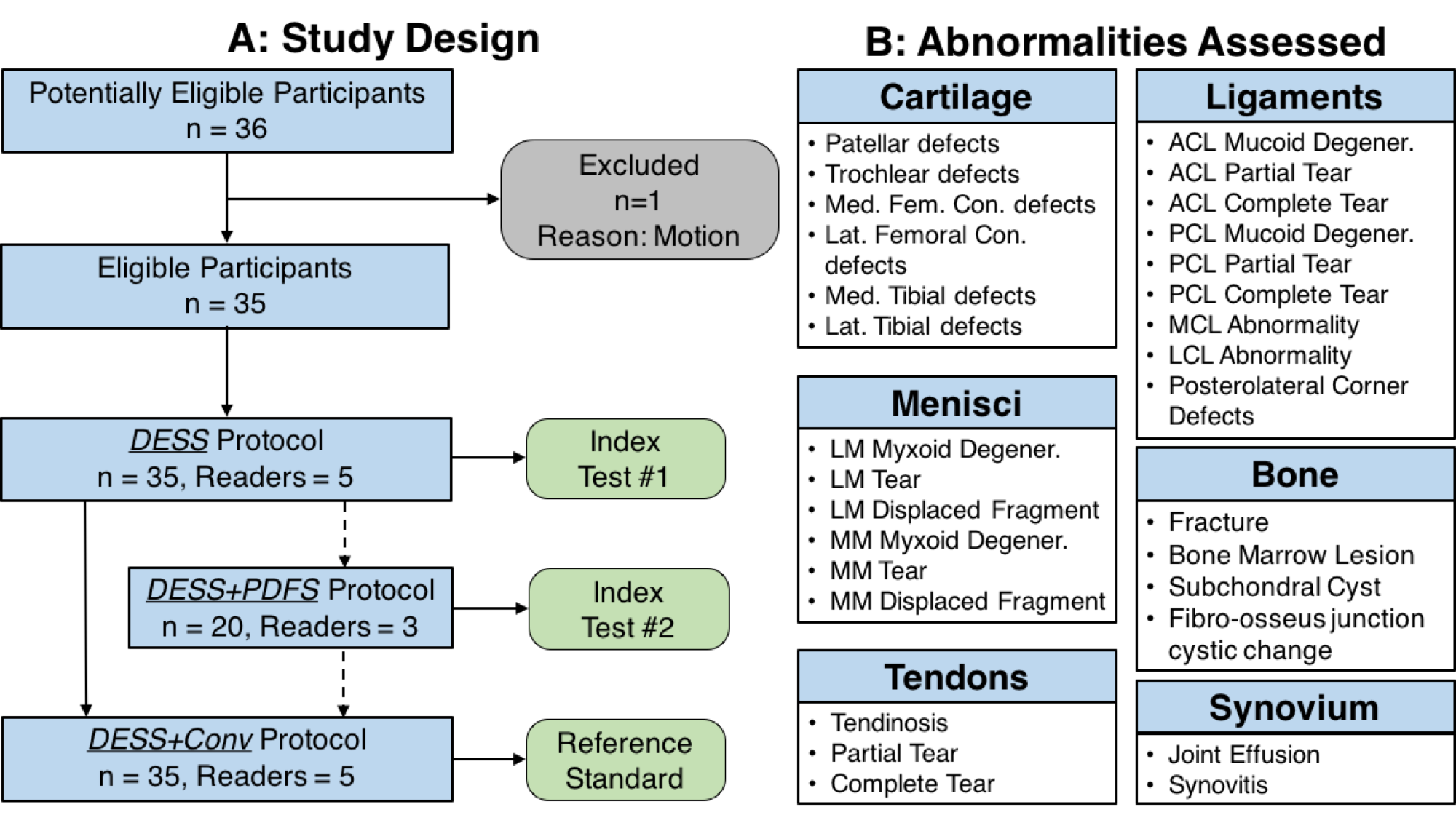
Four experienced musculoskeletal radiologists and one musculoskeletal fellow evaluated all images for the presence of thirty common imaging findings in internal derangements of the knee, sub-divided into categories of bone, cartilage, ligaments, menisci, synovium, and tendons (Fig. 2). The readers recorded the presence of all findings (Yes/No) and scored the diagnostic confidence of the protocol used (0=No Confidence, 1=Low Confidence, 2=Moderate Confidence, and 3=High Confidence).
All readers first scored the DESS-only protocol, and subsequently, scored DESS combined with the conventional (DESS+Conv) protocol. In a subset of 20 patients, three of the five readers scored the DESS protocol first, then DESS with an additional coronal PDFS sequence (DESS+PDFS protocol), and finally with DESS+Conv (study schematic in Fig. 2). The DESS+Conv protocol was chosen as the gold-standard over arthroscopy, as few patients receive diagnostic arthroscopies and because this study aimed at investigating non-inferiority of the rapid protocols.
The percentage of observations where DESS or DESS+PDFS had equivalent confidence ratings as DESS+Conv were tested with exact symmetry tests. Krippendorff's alpha (KA) coefficients evaluated inter-observer agreement11. The sensitivity, specificity, and their confidence intervals (CI) for the DESS/DESS+PDFS protocols were calculated and differences between the DESS and DESS+PDFS measurements were tested by exact McNemar tests.
Results
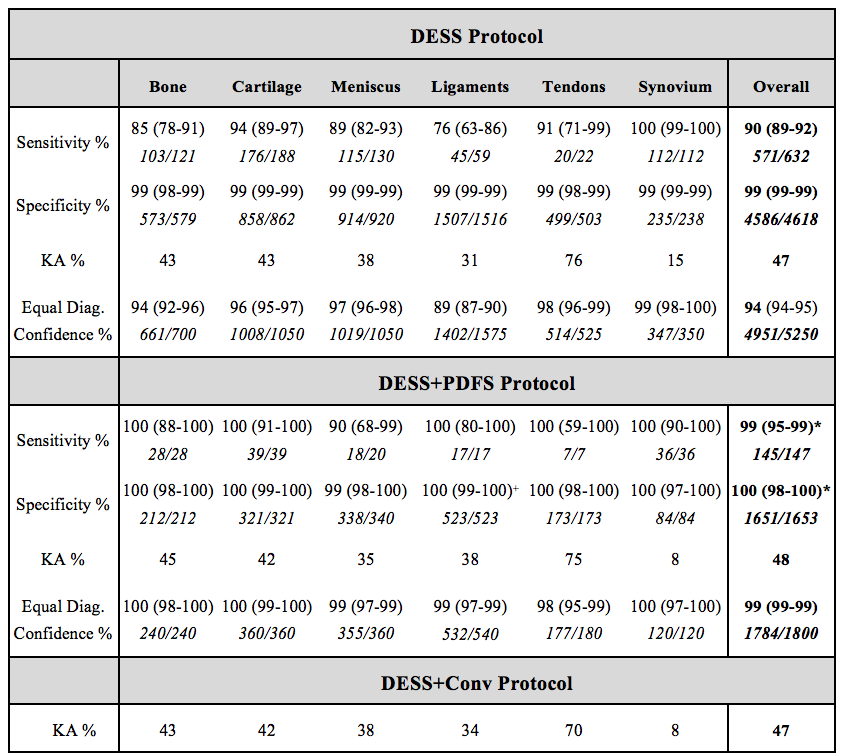
DESS had equivalent diagnostic confidence as DESS+Conv in 94% of findings whereas DESS+PDFS had equivalent diagnostic confidence in 99% of findings (significantly higher than DESS alone, p<0.001). KA values of 47-48% for all three protocols (Fig. 3) indicated moderate inter-reader agreement12.
The DESS protocol had a sensitivity of 90% (88-92% CI) and specificity of 99% (99-99% CI) in assessing the 30 abnormalities (Fig. 3). DESS+PDFS significantly increased sensitivity to 99% (95-99% CI) and the specificity to 100% (99-100% CI) compared to DESS alone (both p<0.001).
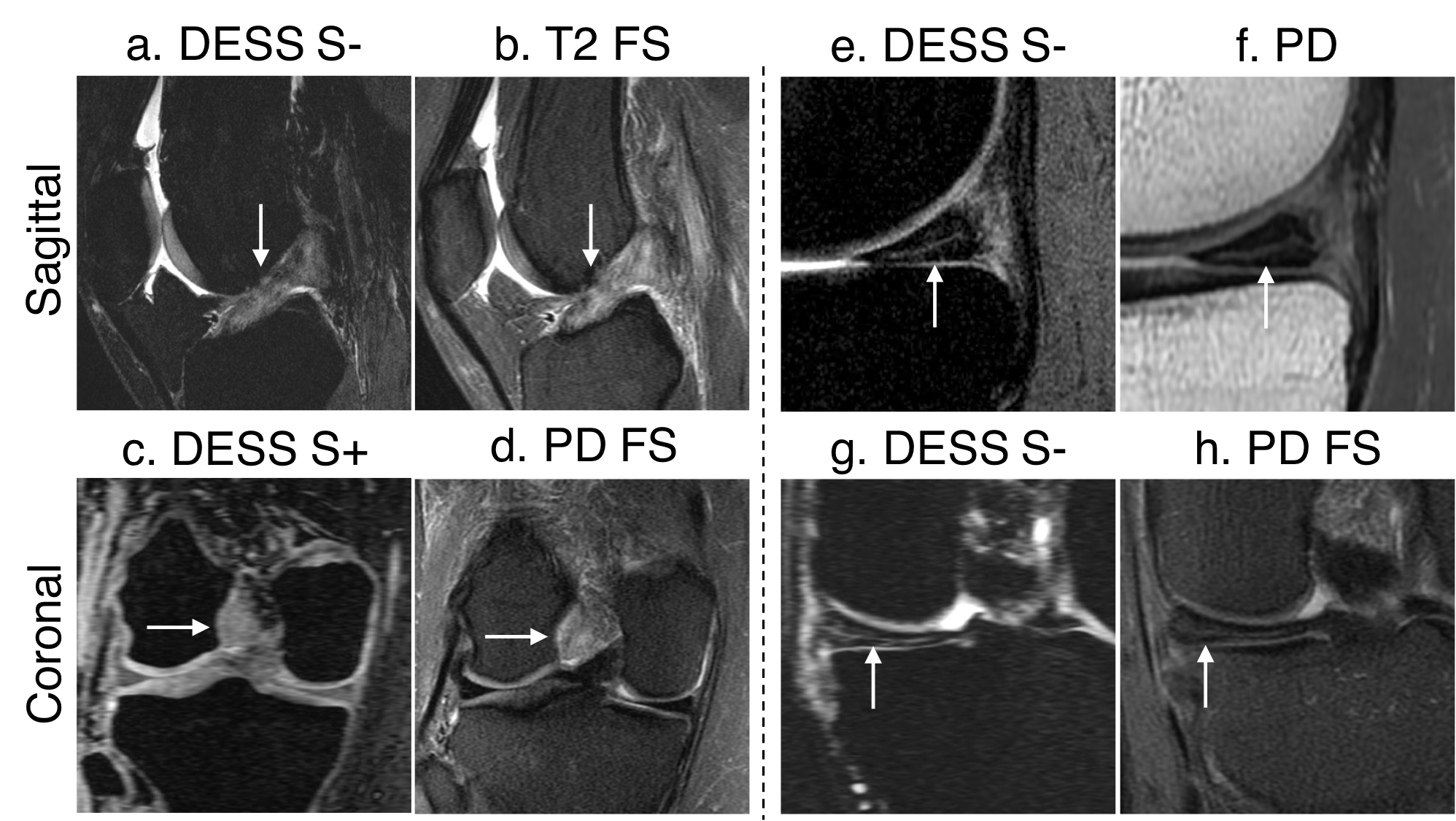
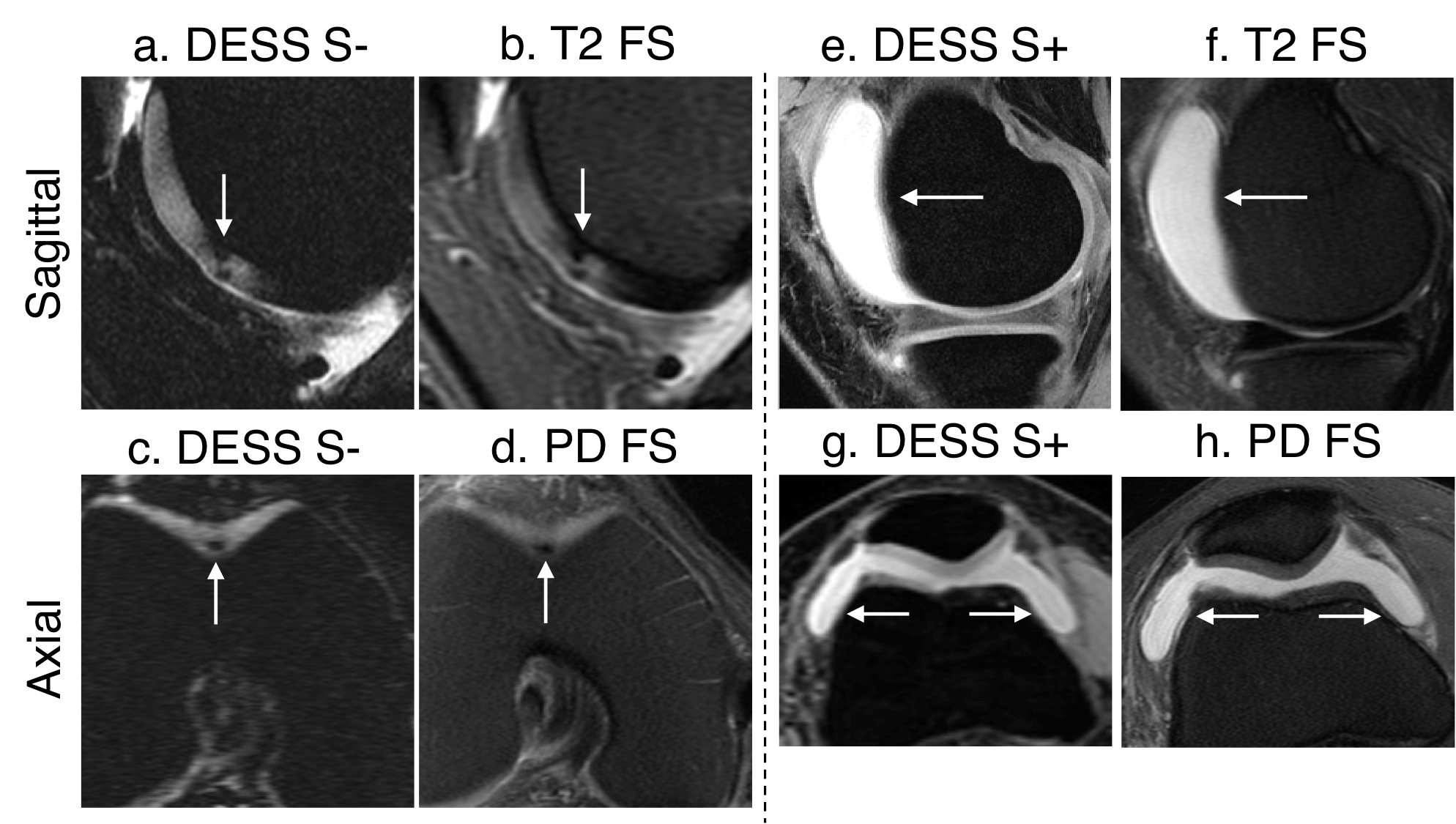
A full-thickness ACL tear appeared similarly on both the DESS S- image and the T2-weighted FS sequence, with disruption of fibers in the mid-portion of the ligament (Fig. 4a-d). A radial tear of the medial meniscus appeared similarly in the DESS S- image and the PD-weighted image, with an increased signal in the posterior horn of the meniscus extending to the tibial articular surface (Fig. 4e-h). Cartilage lesions in the femoral trochlea appeared similarly on DESS images and the conventional images (Fig 5a-d). The bright signal of joint effusion was visible in the DESS images, with comparable size and texture to the conventional sequences (Fig. 5e-h). The availability of high-resolution coronal and axial DESS reformations helped confirm all findings above.
Discussion
Overall, DESS had high diagnostic performance and confidence. Pairing DESS with a coronal PDFS sequence eliminated tiny drawbacks such as MPR-induced blurring of collateral ligaments and underestimation of bone marrow lesion sizes. This study continued previous work but with additional patients and readers for added statistical power3. Reading all scans together for DESS+Conv may provide the most diagnostic information, but may also introduce memory biases as a study limitation. Future studies could include thinner slices with slice-direction parallel imaging and investigate the utility of the automatic T2 maps.Conclusion
We have demonstrated the feasibility of (1) a single 5-minute DESS sequence and (2) a 5-minute DESS sequence paired with a 2-minute coronal PDFS sequence, as two accurate and rapid methods for comprehensive diagnostic whole-joint knee MRI.Acknowledgements
Research support provided by NIH AR0063643, NIH EB002524, NIH AR062068, NIH EB017739, NIH EB015891, and GE Healthcare.References
1. Hing E, Rui P, Palso K. National Ambulatory Medical Care Survey: 2013 State and National Summary Tables. 2013;1:Table 21.
2. Rinck P. What is the Organ Distribution of MRI Studies? Eur Magn Reson Forum – EMRF. 2005.
3. Chaudhari A, Sveinsson B, Wood J, et al. 5 Minute Comprehensive Knee MRI with 3D Double-Echo Steady-State (DESS). Proc Int Soc Magn Reson Med Honolulu. 2016:230.
4. Bruder H, Fischer H, Graumann R, Deimling M. A new steady-state imaging sequence for simultaneous acquisition of two MR images with clearly different contrasts. Magn Reson Med. 1988;42(7):35-42.
5. Redpath TW, Jones RA. FADE--a new fast imaging sequence. Magn Reson Med. 1988;6(2):224-234.
6. Lee SY, Cho ZH. Fast SSFP gradient echo sequence for simultaneous acquisitions of FID and echo signals. Magn Reson Med. 1988;8(2):142-150.
7. Welsch GH, Mamisch TC, Domayer SE, et al. Cartilage T2 assessment at 3-T MR imaging: in vivo differentiation of normal hyaline cartilage from reparative tissue after two cartilage repair procedures--initial experience. Radiology. 2008;247(1):154-161. doi:10.1148/radiol.2471070688.
8. Staroswiecki E, Granlund KL, Alley MT, Gold GE, Hargreaves BA. Simultaneous estimation of T2 and apparent diffusion coefficient in human articular cartilage in vivo with a modified three-dimensional double echo steady state (DESS) sequence at 3 T. Magn Reson Med. 2012;67(4):1086-1096. doi:10.1002/mrm.23090.
9. Friedrich KM, Reiter G, Kaiser B, et al. High-resolution cartilage imaging of the knee at 3T: Basic evaluation of modern isotropic 3D MR-sequences. Eur J Radiol. 2011;78(3):398-405. doi:10.1016/j.ejrad.2010.01.008.
10. Hunter DJ, Guermazi A, Lo GH, et al. Evolution of semi-quantitative whole joint assessment of knee OA: MOAKS (MRI Osteoarthritis Knee Score). Osteoarthr Cartil. 2011;19(8):990-1002. doi:10.1016/j.joca.2011.05.004.
11. Krippendorf K. Reliability in content analysis: Some common misconceptions and recommendations. Hum Commun Res. 2004;30(3):411-433. doi:http://dx.doi.org/10.1111/j.1468-2958.2004.tb00738.x.
12. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-174.
Figures