0341
Simultaneous Bilateral Knee MR Imaging1Radiology, Stanford University, Stanford, CA, United States, 2Radiology, Erasmus MC, Rotterdam, Netherlands
Synopsis
Osteoarthritis (OA) is commonly a bilateral disease. While long scan time and costs have precluded separate scanning of both knees in clinical MRI, there is evidence that bilateral examinations are beneficial for evaluation of OA changes, especially for longitudinal studies. In this study, we demonstrate that a bilateral coil-array setup can image both knees simultaneously in similar scan times as conventional unilateral knee scans with comparable image quality and quantitative accuracy. This has the potential to improve the value of MRI knee evaluations.
Introduction
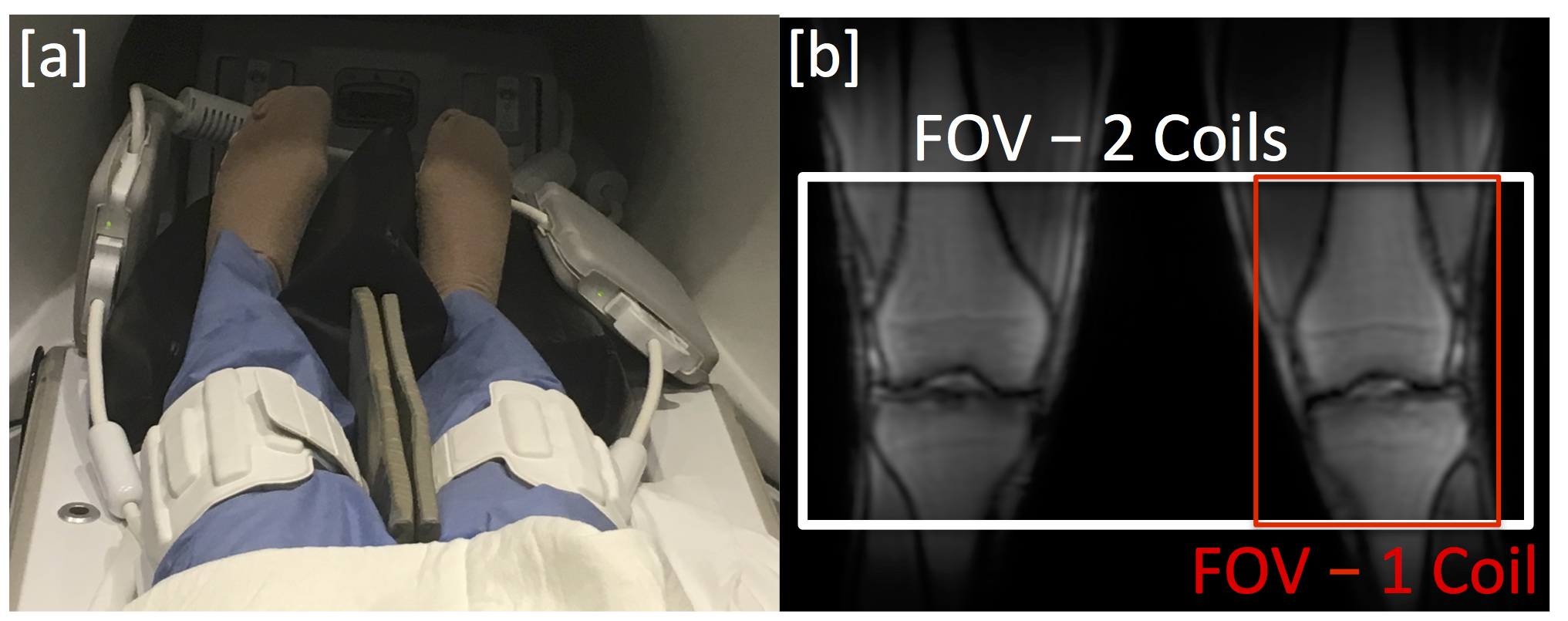
Osteoarthritis(OA) remains a tremendous burden to society, affecting the majority of the population by age 65[1]. OA is commonly a bilateral disease[2]. While long scan time and costs have precluded separate scanning of both knees in clinical MRI, there is evidence that bilateral examinations are beneficial for evaluation of OA changes, especially for longitudinal studies[3]. Simultaneous imaging of both knees without added scan time can drastically reduce scan costs, improve patient comfort and retention, and eliminate potential parameter/sequence differences between scans of each knee. In this work, we describe a bilateral coil setup using two 16-channel flexible coil-arrays to scan both knees simultaneously with similar scan time, image quality, and quantitative accuracy compared to single knee acquisitions.Methods
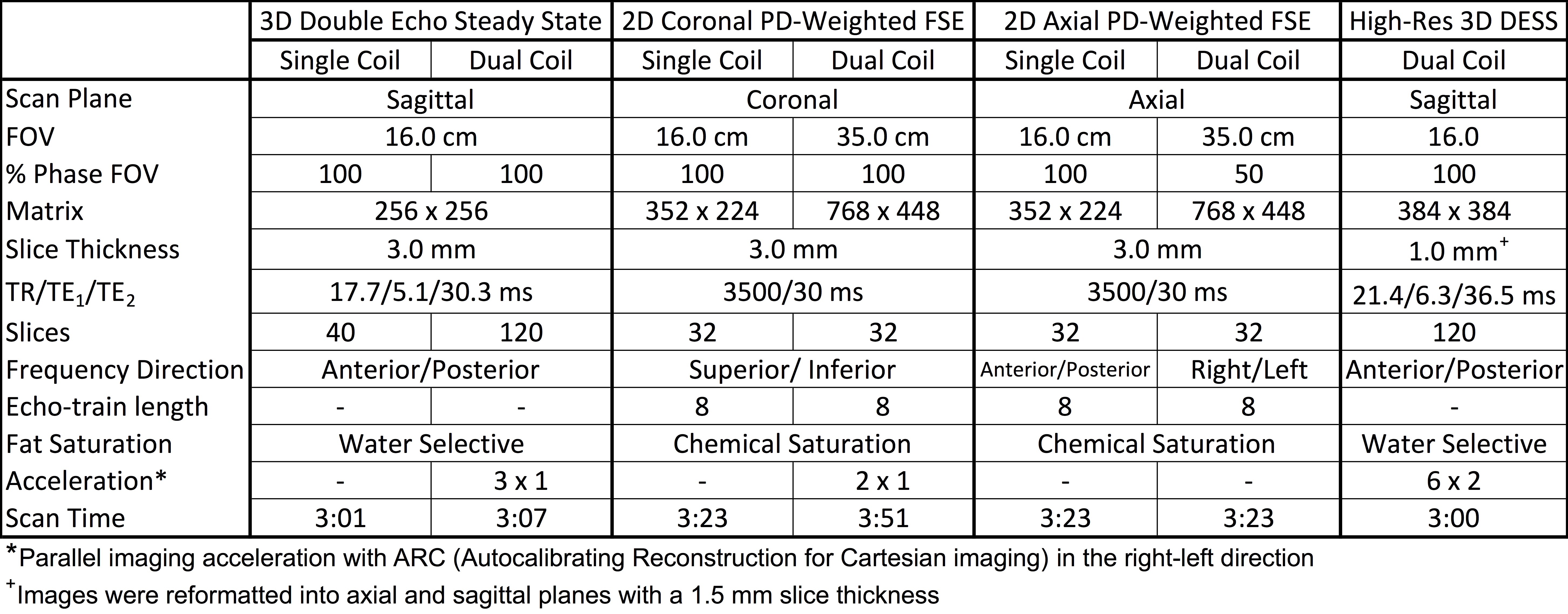
All imaging experiments were performed on a 3.0T scanner (GE Healthcare) with university IRB approval. Hardware modifications and safety testing were performed to enable MR imaging with two 16-channel flexible phased-array, receive only, medium sized extremity coils (NeoCoil, Pewaukee,WI) (Fig. 1). One volunteer was imaged to determine the noise covariance and parallel imaging geometry factors (g-factors) of the dual-coil-array configuration[4,5]. Ten healthy volunteers were then imaged with both dual-coil-array bilateral knee and single-coil-array single-knee configurations(Table 1). Two experienced musculoskeletal radiologists compared relative image quality between blinded and randomized image pairs acquired with each configuration. Differences in T2 relaxation time measurements[6] between dual-coil-array and single-coil-array acquisitions were compared to the standard repeatability of single-coil-array measurements using a Bland-Altman analysis.Results
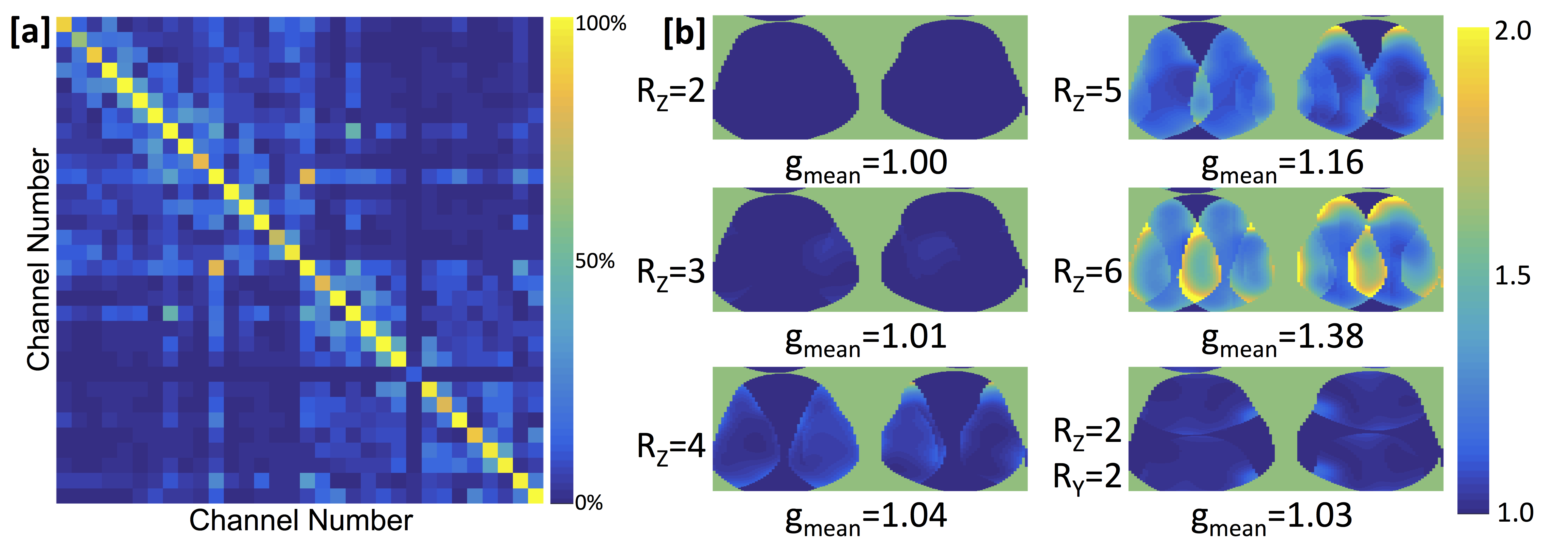
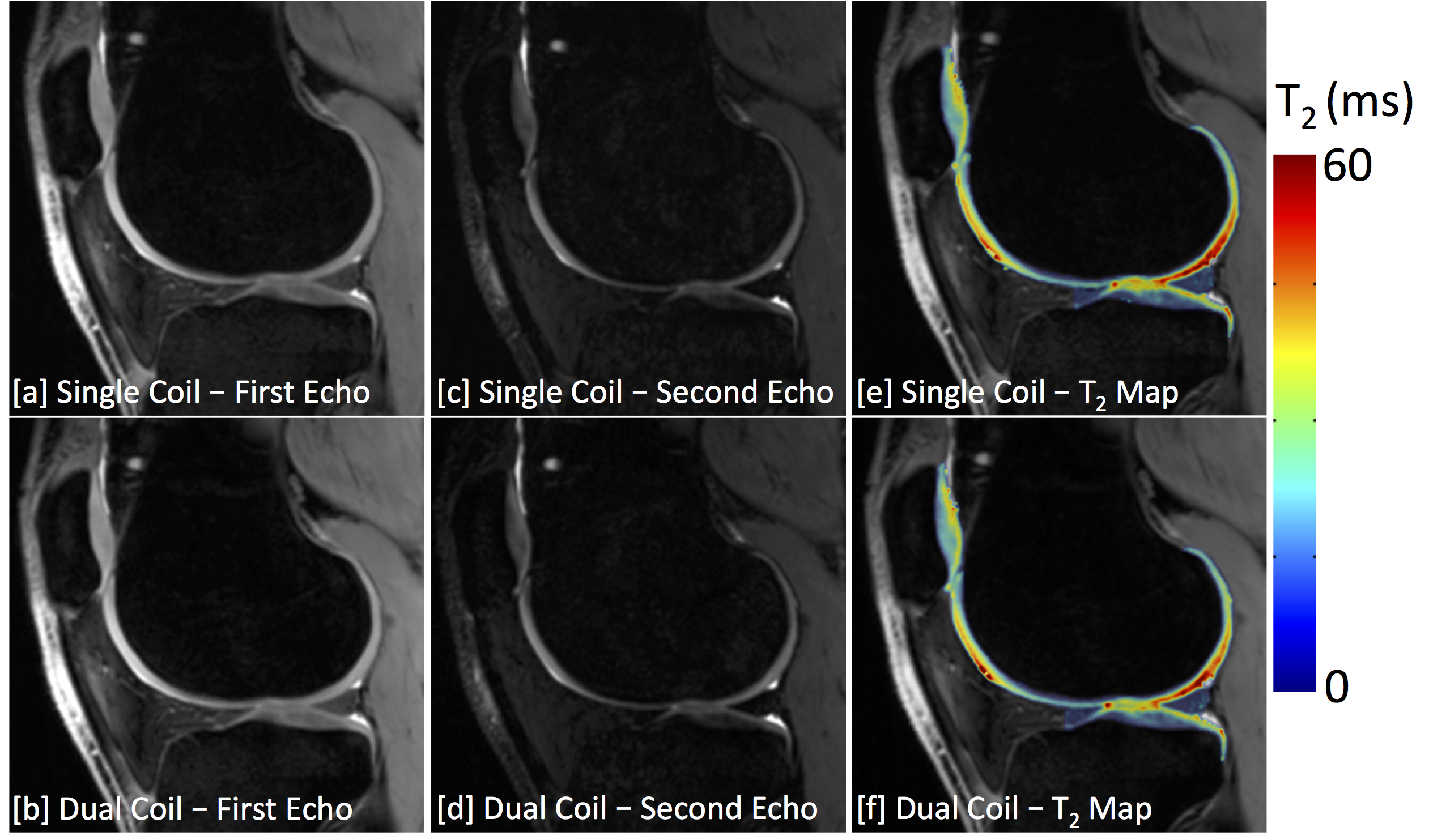
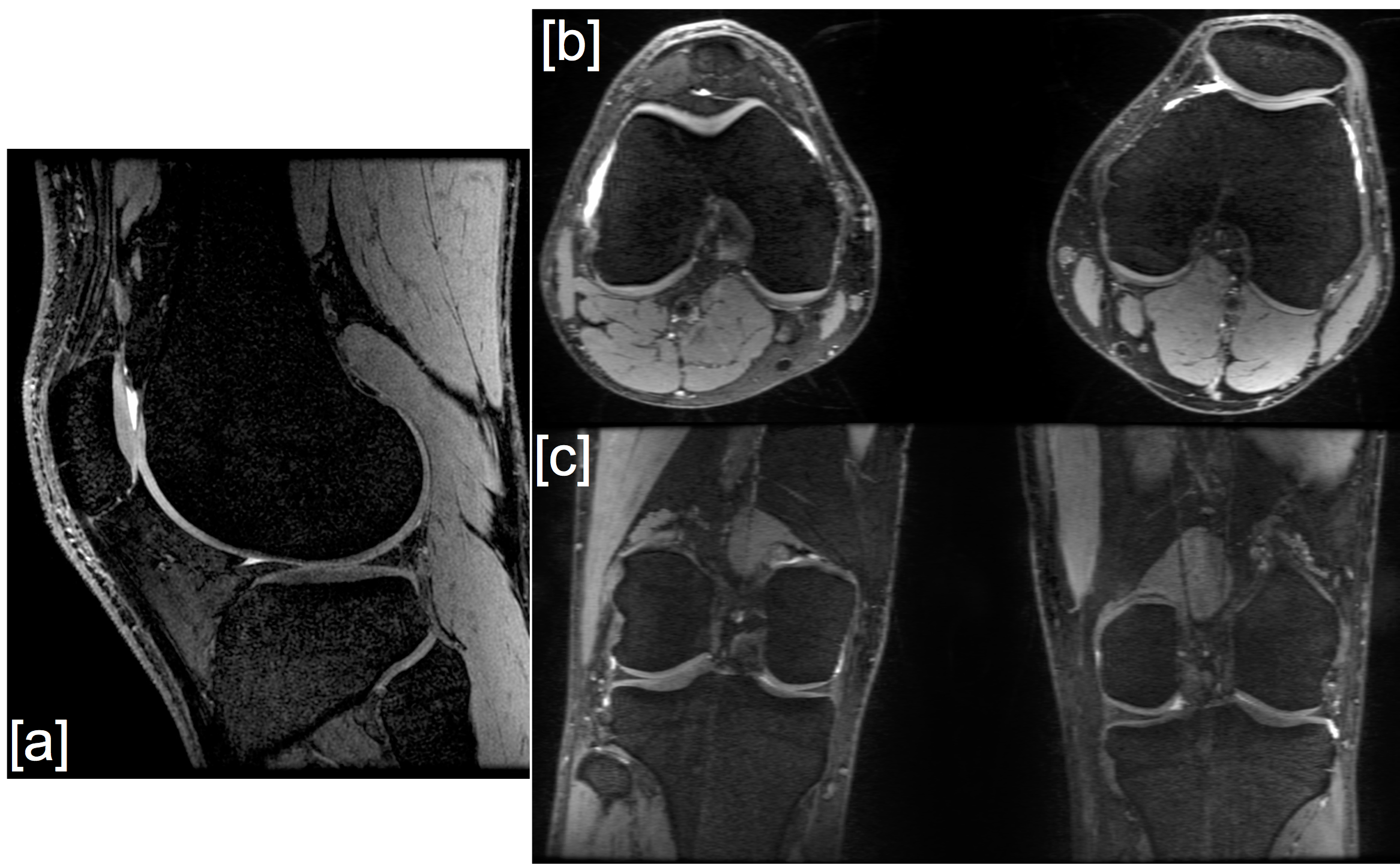
The noise correlation matrix for the 32 channels in the dual-coil-array configuration showed minimal cross-talk between the two coil-arrays (channel numbers 1-16 vs 17-32) (Fig. 2a). Mean g-factors ranged from 1.00 for an acceleration factor, Rz=2, to 1.38 for an acceleration factor Rz=6 (Fig. 2b). Morphologic images show similar image quality between single-coil-array (Figs. 3a,3c) and dual-coil-array acquisitions (Figs. 3b,3d). Image quality ratings of various joint tissues by two blinded reviewers showed mainly no difference between single-coil-array and dual-coil-array acquisitions. Overall, 89% of the ratings were "0" or no difference between the image pairs (95% Confidence Interval (CI): [85%,93%]). There were no ratings of "2"(dual-coil-array much better) or "-2"(dual-coil-array much worse). Bilateral knee MRI acquisitions with the dual-coil-array configuration also maintained quantitative accuracy of measured T2 relaxation times compared with single-knee, single-coil-array acquisitions (Fig. 3e,3f). The mean difference in T2 relaxation time measurements between the dual-coil-array configuration and the single-coil-array configuration was 0.53±0.74 ms (95% limits of agreement: [-0.93 ms,1.99 ms]) with a concordance correlation coefficient of 0.97 (95% CI: [0.96,0.98]). This was similar to the repeatability of the single-coil-array T2 relaxation time measurements, which showed a mean difference of -0.06±1.03 ms (95% limits of agreement: [-2.07 ms,1.96 ms]) and a concordance correlation coefficient of 0.97 (95% CI: [0.95,0.98]). Lastly, higher acceleration factors can also be extended across both knees while maintaining SNR to acquire high-resolution images, which can also be, reformatted to visual multiple scan planes (Fig 4).Discussion
This work demonstrates that a bilateral coil-array setup can image both knees simultaneously in similar scan times to conventional unilateral knee scans, while maintaining image quality and quantitative accuracy. There was nominal cross-talk between each coil-array in the dual-coil-array configuration, which created minimal coil noise amplification (g-factor). Image SNR is inversely proportional to the g-factor as well as the square root of the acceleration factor, R. In 3D DESS scans, data under-sampling by a factor of 3 was offset by a threefold increase in the number of phase encodes in the z-direction to acquire both knees. Thus, due to the low g-factor of the dual-coil-array configuration for RZ=3 (mean g-factor=1.01), this resulted in a negligible change in image SNR compared to fully-sampled single knee acquisitions, with only a 6 second increase in scan time to acquire the ARC (Autocalibrating Reconstruction for Cartesian imaging – similar to GRAPPA) calibration region. Additionally, similar image quality was observed between dual-coil-array and single-coil-array images, as evaluated by blinded pairwise comparison of images from the two configurations by experienced radiologists. Further, bilateral knee T2 relaxation time mapping with the dual-coil-array approach showed similar quantitative T2 values compared to single-knee acquisitions with a single coil-array. Simultaneous imaging of both knees can improve the value of knee MRI in both clinical and research settings; providing an internal control for clinical evaluation of pathology as well as helping reduce costs and improve continuity in research studies.Conclusion
A bilateral coil-array setup can image both knees simultaneous in similar scan times as conventional unilateral knee scans with comparable image quality and quantitative accuracy. Bilateral imaging has the potential to improve the value of MRI knee evaluations.Acknowledgements
This work was funded by GE Healthcare and National Institute of Health (NIH) grants K99EB022634, R01EB002524, R01AR0063643, and K24AR062068.References
[1] Arden N, Nevitt MC. Osteoarthritis: epidemiology. Best Practice & Research Clinical Rheumatology 2006;20(1):3-25.
[2] Metcalfe AJ, Andersson ML, Goodfellow R, Thorstensson CA. Is knee osteoarthritis a symmetrical disease? Analysis of a 12 year prospective cohort study. BMC musculoskeletal disorders 2012;13:153.
[3] Jungmann PM, Brucker PU, Baum T, Link TM, Foerschner F, Minzlaff P, Banke IJ, Saier T, Imhoff AB, Rummeny EJ, Bauer JS. Bilateral cartilage T2 mapping 9 years after Mega-OATS implantation at the knee: a quantitative 3T MRI study. Osteoarthritis Cartilage 2015;23(12):2119-2128.
[4] Uecker M, Lai P, Murphy MJ, Virtue P, Elad M, Pauly JM, Vasanawala SS, Lustig M. ESPIRiT--an eigenvalue approach to autocalibrating parallel MRI: where SENSE meets GRAPPA. Magn Reson Med 2014;71(3):990-1001.
[5] Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P. SENSE: sensitivity encoding for fast MRI. Magnetic Resonance in Medicine 1999;42(5):952-962.
[6] Sveinsson B, Chaudhari AS, Gold GE, Hargreaves BA. A simple analytic method for estimating T2 in the knee from DESS. Magn Reson Imaging 2017;38:63-70.
Figures