0323
High Resolution Diffusion Tensor Imaging of the Hippocampus in Temporal Lobe Epilepsy1Biomedical Engineering, University of Alberta, Edmonton, AB, Canada, 2Neurology, University of Alberta, Edmonton, AB, Canada
Synopsis
Diffusion tensor imaging of the hippocampus in temporal lobe epilepsy (TLE) has previously relied on very low spatial resolution acquisitions, limiting localization of hippocampal substructure and leading to partial volume effects in diffusion parameter quantification. This study uses a high resolution (1x1x1 mm3) single-shot diffusion protocol to yield excellent quality mean diffusion weighted images (DWIs) that allow for visualization of hippocampal substructure (e.g. presence/absence of the stratum lacunosum moleculare). Improved delineation of structure allows for segmentation of the hippocampus in native space (without co-registration to anatomical images), revealing elevated MD and loss of internal architecture in TLE subgroups.
Introduction
Ex-vivo diffusion tensor imaging (DTI) of resected hippocampi from patients with temporal lobe epilepsy (TLE) has demonstrated aberrant intra-hippocampal connections1, loss of laminar structure2, and microstructural variation corresponding to histology3. In-vivo DTI in TLE patients has demonstrated elevated hippocampal mean diffusivity (MD)4; however, low spatial resolution acquisitions used previously (e.g. 2x2x2 = 8 mm3 voxels) require co-registration with T1 images for extraction of diffusion parameters, limiting accuracy and precluding evaluation of hippocampal substructure. This study uses high resolution (1x1x1 mm3) DTI to identify potential anomalies in hippocampal sub-structure, diffusion parameters and volume in TLE patients with and without mesial temporal sclerosis (MTS).Methods
19 controls (ages 42 ± 14 years; 14 females) and 18 patients with TLE (44 ± 14 years; 11 females) were scanned on a 3T Siemens Prisma. Diffusion images were acquired via single shot 2D EPI (GRAPPA R=2; 6/8 PPF; A/P phase encode), FOV=220x216 mm2, matrix= 220x216, 20 1 mm slices with no gap, 1x1x1 mm3 with no interpolation, TE=72 ms, TR=2800 ms, 10 averages of 10 gradient directions at b=500 s/mm2 and 10 b0s in 5:18 min. Images were acquired in an axial-oblique plane aligned along the length of the hippocampus to limit the number of slices and scan time. Gibbs ringing, motion/distortion correction and tensor calculation was performed in ExploreDTI. Hippocampi were manually segmented in native space on mean diffusion weighted images (DWIs) in ITK-snap to yield hippocampal volume and MD.
The TLE group was sub-divided into unilateral MTS (n=8), bilateral MTS (n=3), non-lesional TLE (n=5) and TLE with non-MTS pathology (n=2; low grade tumor and cavernous hemangioma) according to previously acquired clinical imaging. Mean and standard deviation (SD) values were calculated for each variable in the control group, and a cut-off of 2 SD was used to determine clinically significant differences in individual participants. In addition to quantitative metrics, mean DWIs were qualitatively evaluated by a single blinded rater to independently classify subjects as normal, left, right or bilateral MTS based on gross structure (e.g. atrophy) and internal substructure (e.g. presence/absence of the stratum lacunosum moleculare). Groupings from this evaluation were then compared to classifications assigned independently from clinical imaging.
Results
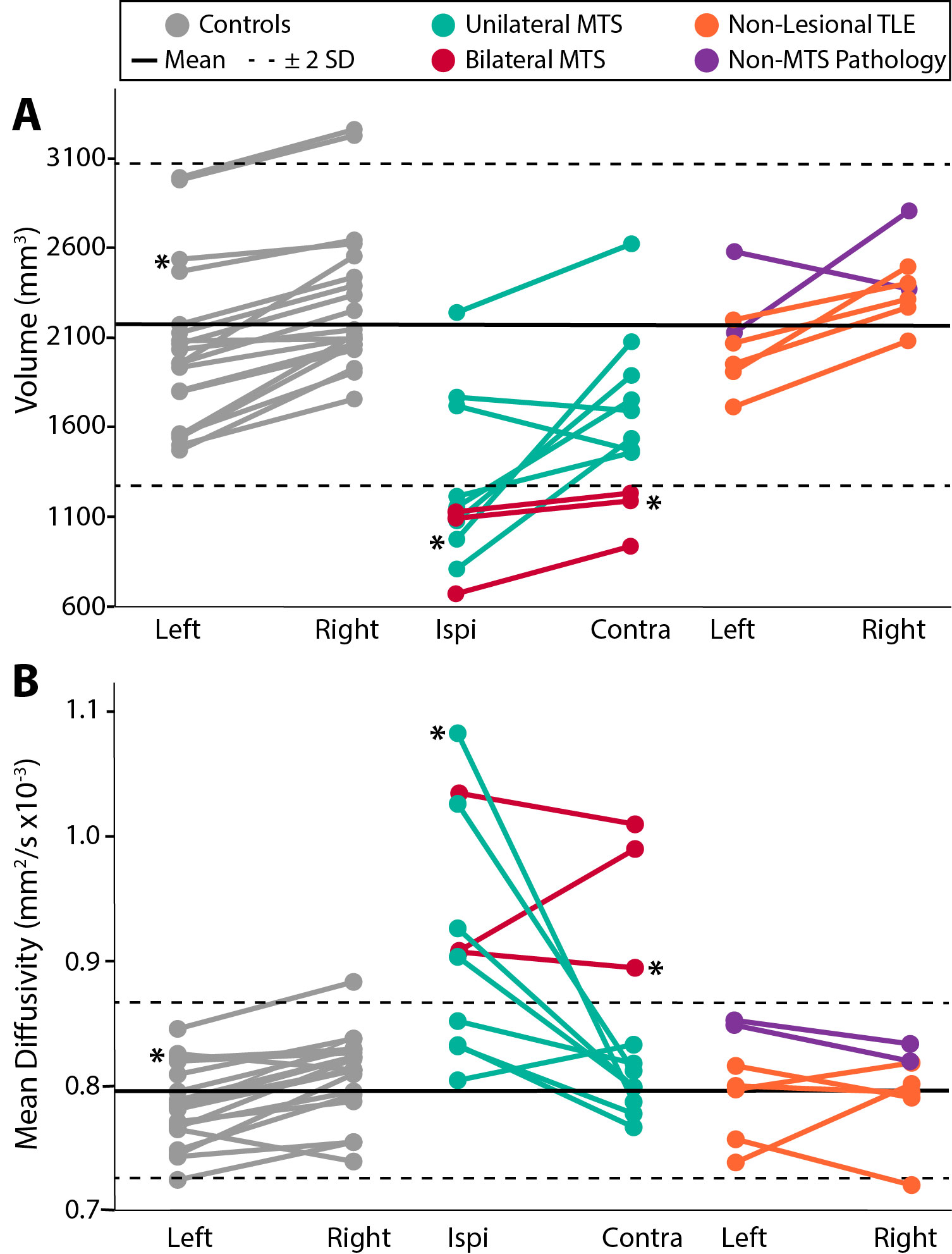
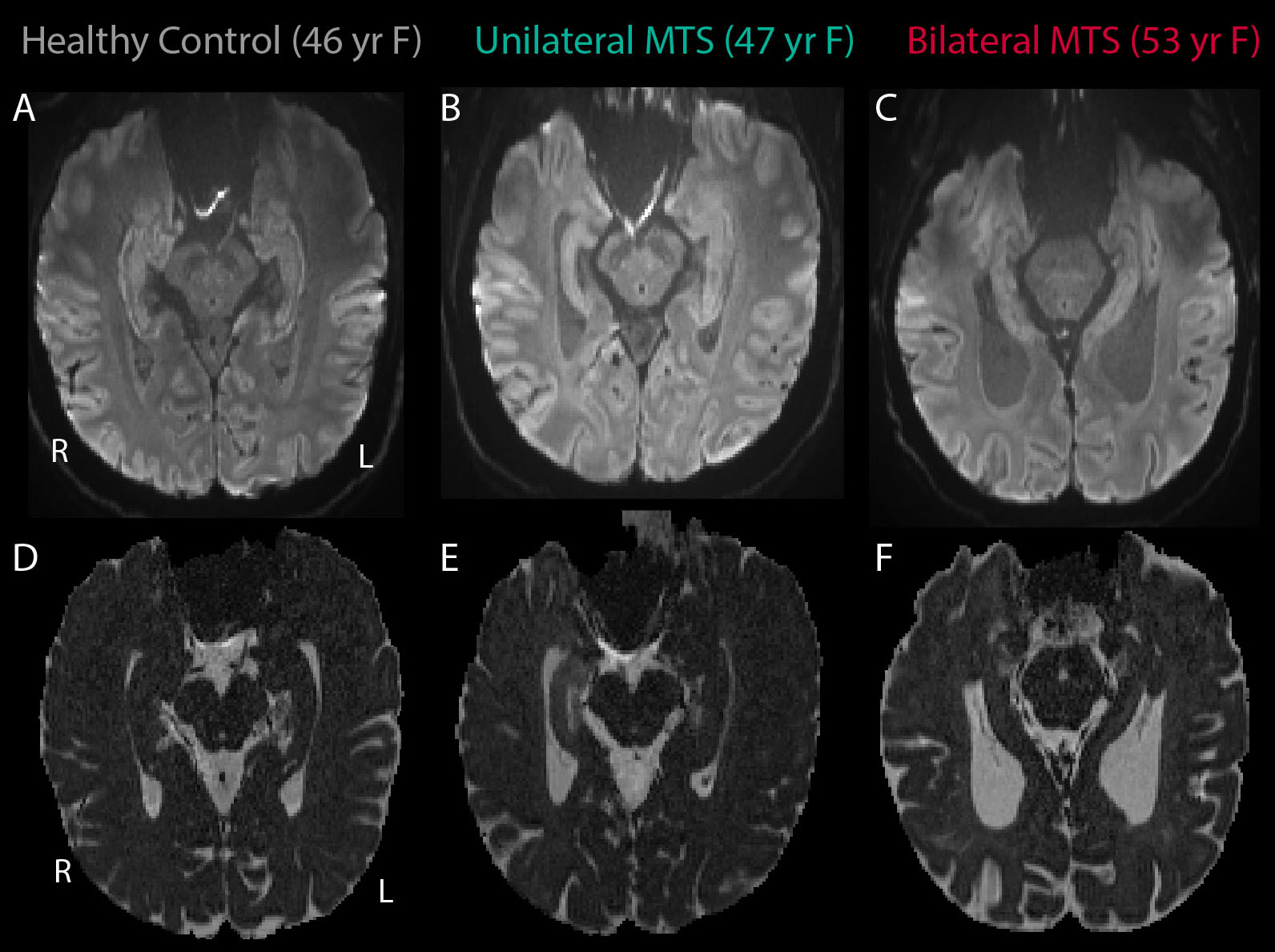
Hippocampal volume and MD were all within 2 SD of the control means for subjects with non-lesional TLE and non-MTS pathology (Figure 1). Conversely, all bilateral MTS patients and 3/8 unilateral MTS patients fell > 2 SD from the control mean for reduced volume and elevated MD on the ipsilateral side (or bilaterally for bilateral patients). In the remaining five unilateral MTS patients, two had ipsilateral volumes (but not MD values) > 2 SD from the control mean, one had MD values (but not volumes) > 2 SD from the control mean, and two were within 2 SD of the control mean for both volume and MD. For the unilateral MTS group, while volume was slightly reduced in the contralateral hippocampus, MD values were normal for all subjects. Mean diffusion weighted images show expected internal architecture (e.g. SLM, digitations) in an example healthy control (Figure 2A) that are not evident in the sclerotic hippocampus of a unilateral MTS patient (Figure 2B) or bilaterally in a bilateral MTS patient (Figure 2C). Elevation of MD is visually evident in the unilateral patient within the remaining sclerotic hippocampus (Figure 2E). Blinded qualitative evaluation of mean DWIs classified 23/26 subjects in the control, non-lesional TLE, or non-MTS pathology group as having “normal” hippocampi, 3/3 bilateral MTS as having bilateral MTS, and 5/8 unilateral MTS as unilateral MTS (with correct lateralization). 2/3 of the remaining unilateral MTS patients were classified as “normal” and 1/3 as bilateral MTS. Of note, the two unilateral MTS subjects classified as “normal” were the same patients who fell within the normal range for both volume and MD bilaterally.Discussion
High resolution (1x1x1 mm3) diffusion tensor imaging of the human hippocampus acquired in a clinically feasible scan time of ~5 minutes yields impressive visualization of internal architecture, allowing for both qualitative evaluation and quantification of MD and volume without the need for co-registration. Greater magnitude deviations in MD relative to volume, and incomplete subject overlap of MD/volume changes in the sclerotic hippocampus along with normal MD but reduced volume of the contralateral hippocampus in unilateral MTS patients suggests that these metrics reflect unique pathophysiological mechanisms. Moreover, classification of MTS pathology based on mean DWIs alone confirms the impressive detail and information that can be gleaned qualitatively from this acquisition, which may have applications to numerous disorders affecting the hippocampus.Acknowledgements
This study was funded by the Canadian Institutes of Health Research (CIHR).References
1. Modo M, Hitchens TK, Liu JR, Richardson RM. Detection of aberrant hippocampal mossy fiber connections: Ex vivo mesoscale diffusion MRI and microtractography with histological validation in a patient with uncontrolled temporal lobe epilepsy. Hum Brain Mapp. 2016;37(2):780-795.
2. Coras R, Milesi G, Zucca I, et al. 7T MRI features in control human hippocampus and hippocampal sclerosis: an ex vivo study with histologic correlations. Epilepsia. 2014;55(12):2003-2016.
3. Colon-Perez LM, King M, Parekh M, et al. High-field magnetic resonance imaging of the human temporal lobe. Neuroimage-Clinical. 2015;9:58-68.
4. Nazem-Zadeh MR, Schwalb JM, Elisevich KV, et al. Lateralization of temporal lobe epilepsy using a novel uncertainty analysis of MR diffusion in hippocampus, cingulum, and fornix, and hippocampal volume and FLAIR intensity. J Neurol Sci. 2014;342(1-2):152-161.
Figures