0319
Methods to accelerate STAGE: Toward 8 min for Twelve 3D images on 1.5T1Neusoft Medical System, Shanghai, China, 2Shanghai Key Laboratory of Magnetic Resonance, East China Normal University, Shanghai, China, 3The MRI Institute for Biomedical Research, Detroit, MI, United States, 4Sino-Dutch Biomedical and Information Engineering School, Northeastern University, Shenyang, China, 5Department of Radiology, School of Medicine, Wayne State University, Detroit, MI, United States
Synopsis
A technique named Strategically Acquired Gradient Echo (STAGE) was recently published, which can acquire 10 images with sufficient resolution, good SNR, and co-registration in one 5-min scan on 3T. With an additional 4-min scan, MRAV and MRA can also be produced. However, to acquire a full set of 12 images on 1.5T takes over 20 minutes, which is still longer than clinical expectation. Novel acquisition and reconstruction schemes are developed in this work to further reduce acquisition time. Feasibility experiments demonstrate it is achievable to acquire 12 high quality clinically meaningful images with 0.67×1.33×2.7 mm3 in 8 minutes on 1.5T.
Introduction
Multi-contrast brain imaging is necessary for comprehensive diagnosis of cerebral disease. Conventional individual acquisition scheme suffers from long scan time. To address this issue, a technique called Strategically Acquired Gradient Echo (STAGE) 1, 2, 3 was recently published, which can acquire 10 types of images with sufficient resolution, good SNR, and co-registration in one 5-min scan on 3T. With an additional 4-min scan 3, MRAV and MRA can also be produced. Using the published protocol, the total acquisition time for the full set of 12 images would be 9 min and 17 min on 3T and 1.5T separately. The purpose of this work is to develop new acquisition and reconstruction schemes to further reduce the total acquisition time. Feasibility experiments demonstrate that it is achievable to acquire 12 high quality clinically meaningful images with 0.67×1.33×2.7 mm3 resolution in 8 minutes on 1.5T.Methods
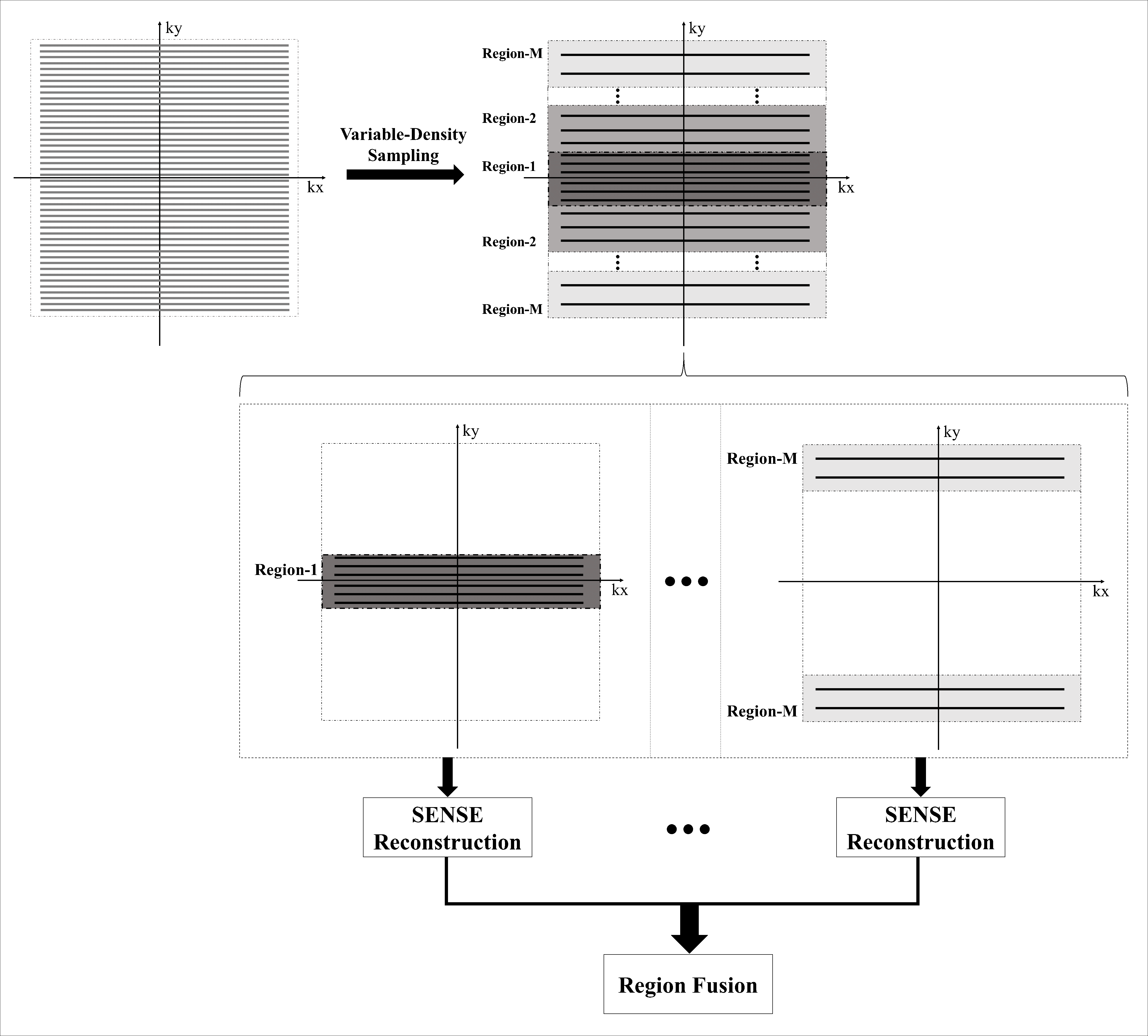
Sequence Design To save acquisition time, two strategies are used. First, the two separate acquisitions introduced in Ref [1] and Ref [3] are combined to be one consecutive acquisition. Second, to accelerate acquisition without degrading image quality much, a variable density (VD) sampling strategy, as shown in Fig. 1, is adopted. In this strategy, the k-space is divided into multiple regions, and the acceleration factors are increased from the inside region out. The sampling density in each region keeps constant.
Data Acquisition and Simulation Two healthy volunteers were scanned on a NMS S15P 1.5T system (Neusoft Medical System, Shenyang, China) with an 8-channel head coil (NMS, Shenyang, China). Eight sets of 3D axial images with fully acquired k-space were collected in 21 min. Partially acquired data sets were simulated by dividing the whole k-space into two regions with acceleration factor of 2 along L-R direction for the central region and 4 for the outer region. Partial Fourier factor 80% was used along L-R direction. The partial acquisition of net acceleration factor 2.78 simulated an 8-min acquisition.
Data Reconstruction A non-iterative VD SENSE 4 reconstruction algorithm was developed, as shown in Fig. 1. The algorithm proposed in Ref [5] was used for Partial Fourier reconstruction. The methods described in Ref [1, 2, 3] were applied for post-processing with slight modification to take advantage of 8-echo for higher SNR.
Results
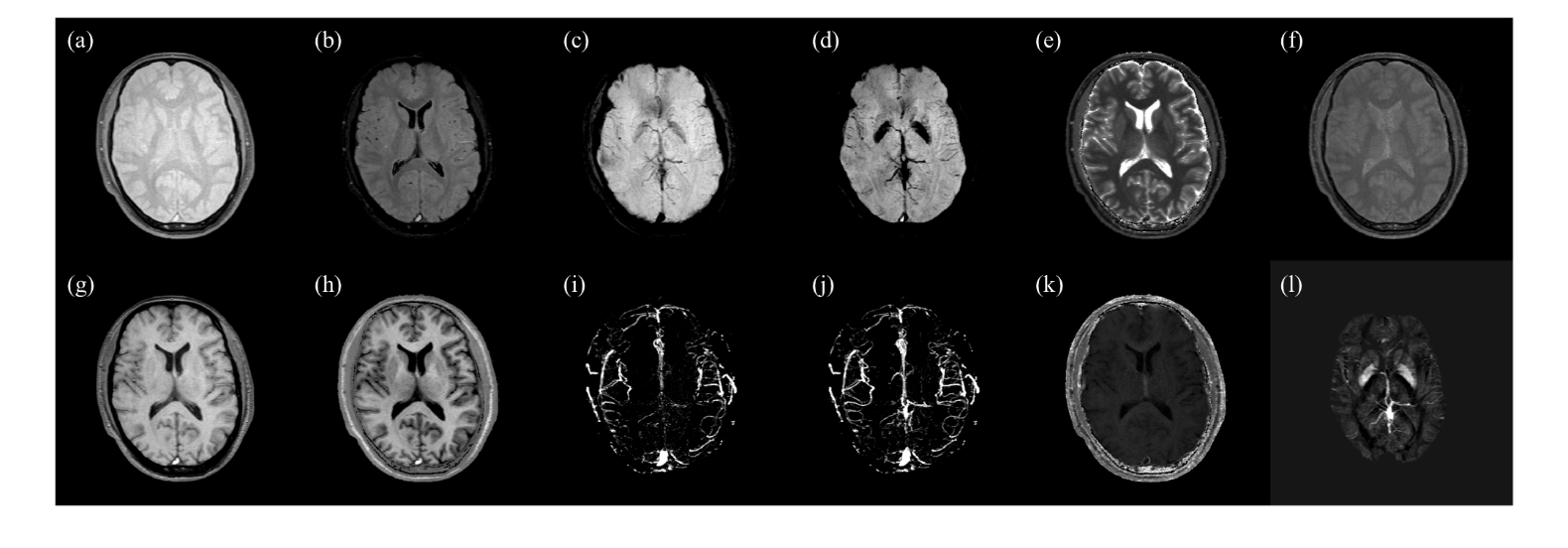
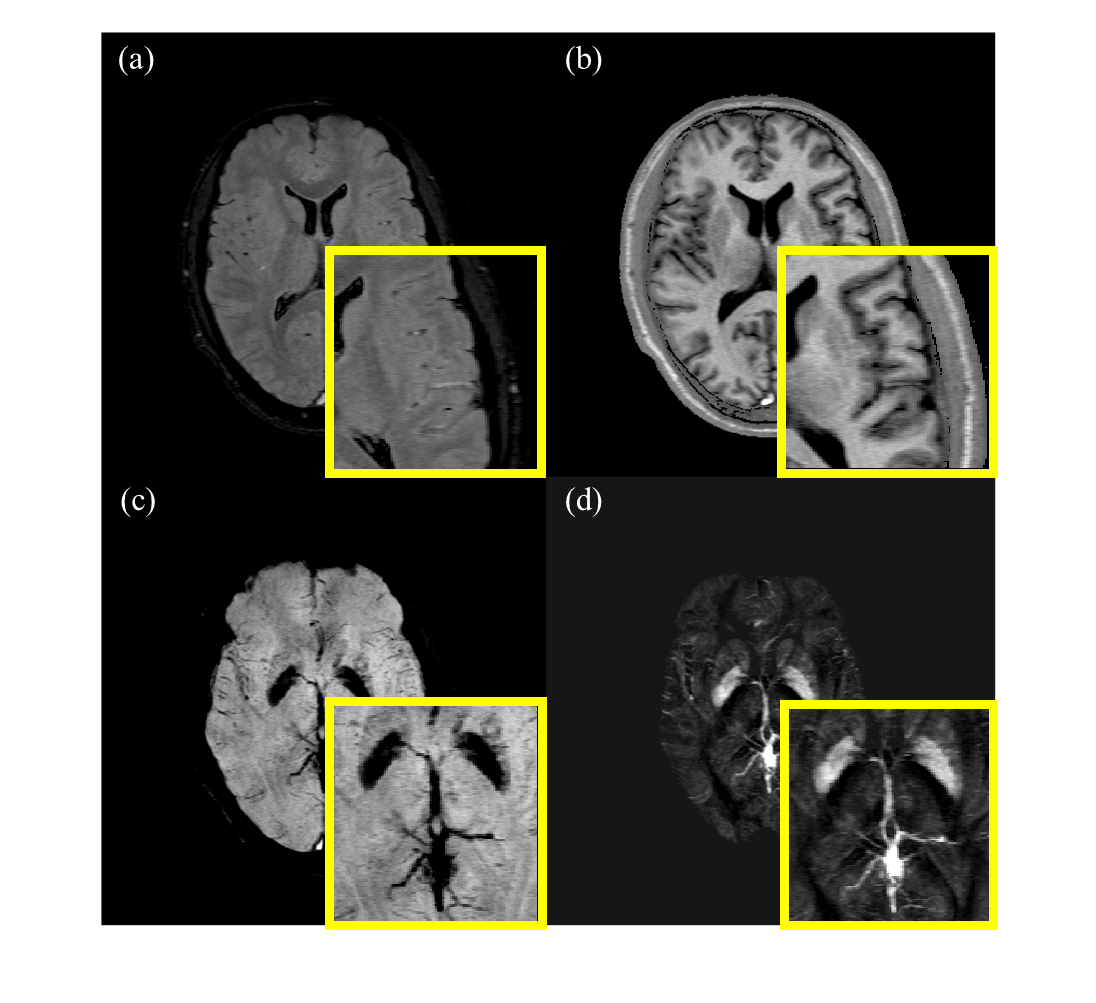
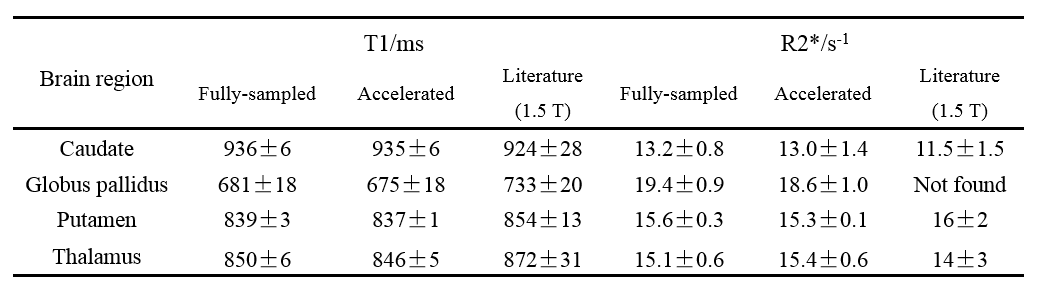
Based on the reconstruction from the partially acquired 8-echo data set, twelve 3D brain images with resolution 0.67×1.33×2.7 mm3 were derived, including T1w, PDw, simulated FLAIR (sFLAIR), enhanced T1w (eT1w), SWI, true-SWI (tSWI), MRAV, MRA, T1 map, PD map, R2* map and QSM. The results of one subject are shown in Fig. 2. For better visualization, Fig. 3 provides enlarged display for sFLAIR, eT1w, tSWI and QSM. Table 1 presents the comparisons of the calculated T1 and R2* values respectively from the fully-sampled and simulated partially acquired STAGE, and also with those in literature. The biases for different regions between the accelerated STAGE and the fully-sampled one are all within 5%.Discussion
As shown in Figs. 2 and 3, the images reconstructed with acceleration factor 2.78 have no visible artifacts due to k-space undersampling. From Fig. 3, it can be clearly seen that sFLAIR (Fig. 3a) and eT1w (Fig. 3b) images show excellent CNR, and the reconstructed tSWI (Fig. 3c) can well characterize the structures with high susceptibility, such as veins and globus pallidus. Furthermore, the generated QSM (Fig. 3d) also provides accurate basal ganglia and veins. Table 1 demonstrates the partially acquired STAGE can derive similar parametric values as the fully-sampled STAGE. There are two reasons that the proposed method resulted in high image quality even if the acceleration factor along one direction is as high as 2.78. First, with 8 echoes, there are more data for each calculated image, which is helpful for higher SNR. Second, the VD acquisition scheme using low acceleration factor at the central k-space protect the contrast and phase well, which is also important for the calculations of SWI, QSM, and quantitative mapping. Different from the conventional reconstruction methods for VD acquisition, the proposed non-iterative reconstruction strategy is computationally efficient, which can be easily applied to clinical practice.Conclusion
With the proposed acquisition and reconstruction method for acceleration, we demonstrated the feasibility to acquire twelve 3D brain images with high resolution, good SNR and co-registration in one single 8-min scan on a 1.5T.Acknowledgements
No acknowledgement found.References
[1] Chen Y, Liu S, Wang Y, et al. STrategically acquired gradient Echo (STAGE) imaging, part I: Creating enhanced T1 contrast and standardized susceptibility weighted imaging and quantitative susceptibility mapping. Magn Reson Imag, 2017, doi:10.1016/j.mri.2017.10.005.
[2] Wang Y, Chen Y, Wu D, et al. Strategically acquired gradient Echo (STAGE) imaging, part II: Correcting for RF inhomogeneities in estimating T1 and proton density. Magn Reson Imag, 2017, doi:10.1016/j.mri.2017.10.006.
[3] Chen Y, Liu S, Kang Y, et. al. An interleaved sequence for simultaneous MRA, SWI and QSM. ISMRM 2017; p1215.
[4] Pruessmann KP, Weiger M, Scheidegger MB, et al. SENSE: sensitivity encoding for fast MRI. Magn Reson Med, 1999; 42(5): 952-962.
[5] Huang F, Lin W, Li Y. Partial Fourier reconstruction through data fitting and convolution in k-space. Magn Reson Med, 2009; 62:1261-1269.
Figures