0306
Time-encoded golden angle radial ASL1C.J. Gorter Center for high field MRI, Department of Radiology, Leiden University Medical Center, Leiden, Netherlands, 2Philips, Best, Netherlands
Synopsis
The golden angle readout provides a flexible approach to acquire multiple reconstructions, each with a different trade-off between spatial and temporal resolution from the same dataset. In combination with a Hadamard labeling scheme, the golden angle readout can be optimized for reconstructions at multiple spatial resolutions, allowing for multi-slice acquisition. By changing to single-slice acquisition, high temporal resolution angiography and high quality perfusion images can be reconstructed from a single dataset.
Introduction
Radial sampling of k-space based on the golden angle, allows for retrospectively choosing the temporal resolution, since k-space is uniformly sampled for any arbitrary temporal window1. Moreover, by changing the number of spokes included in the reconstruction, the effective spatial resolution can be controlled. The golden angle radial readout provides therefore an extremely flexible approach to obtain multiple reconstructions with each different trade-offs between spatial and temporal resolution from the same data.
In combination with arterial spin labeling, a golden angle readout was proposed to obtain dynamic angiographic and perfusion images from the same dataset2,3. For this implementation, the golden angle readout was the only source of temporal information thereby necessitating to readout information over a 2 seconds period, which led to signal attenuation over time due to the large amount of excitation pulses that saturated the ASL-label2. Moreover, to sample with a high enough temporal resolution the approach was more suited for a single slice(or limited number of slices) acquisition.
By combining the golden angle readout with a time-encoding(Hadamard) labeling scheme as the primary source of temporal information, the golden angle readout can be optimized for reconstructions at multiple spatial resolutions, and it can enable acquisition of more slices to enable whole brain coverage.
The goal of the current study was to employ a time-encoded labeling scheme as the primary source of temporal information, so that the golden angle readout could act primarily as a multiple spatial resolution tool. Furthermore, by changing the acquisition to a single slice, high temporal resolution angiography and high-quality perfusion images can be acquired from a single acquisition.
Methods
Six healthy volunteers (age 21-40 y.o.,4f/2m) were scanned using a 32-channel head coil on a 3T scanner (Achieva, Philips, Netherlands). All volunteers provided informed consent and the study was approved by the local IRB.
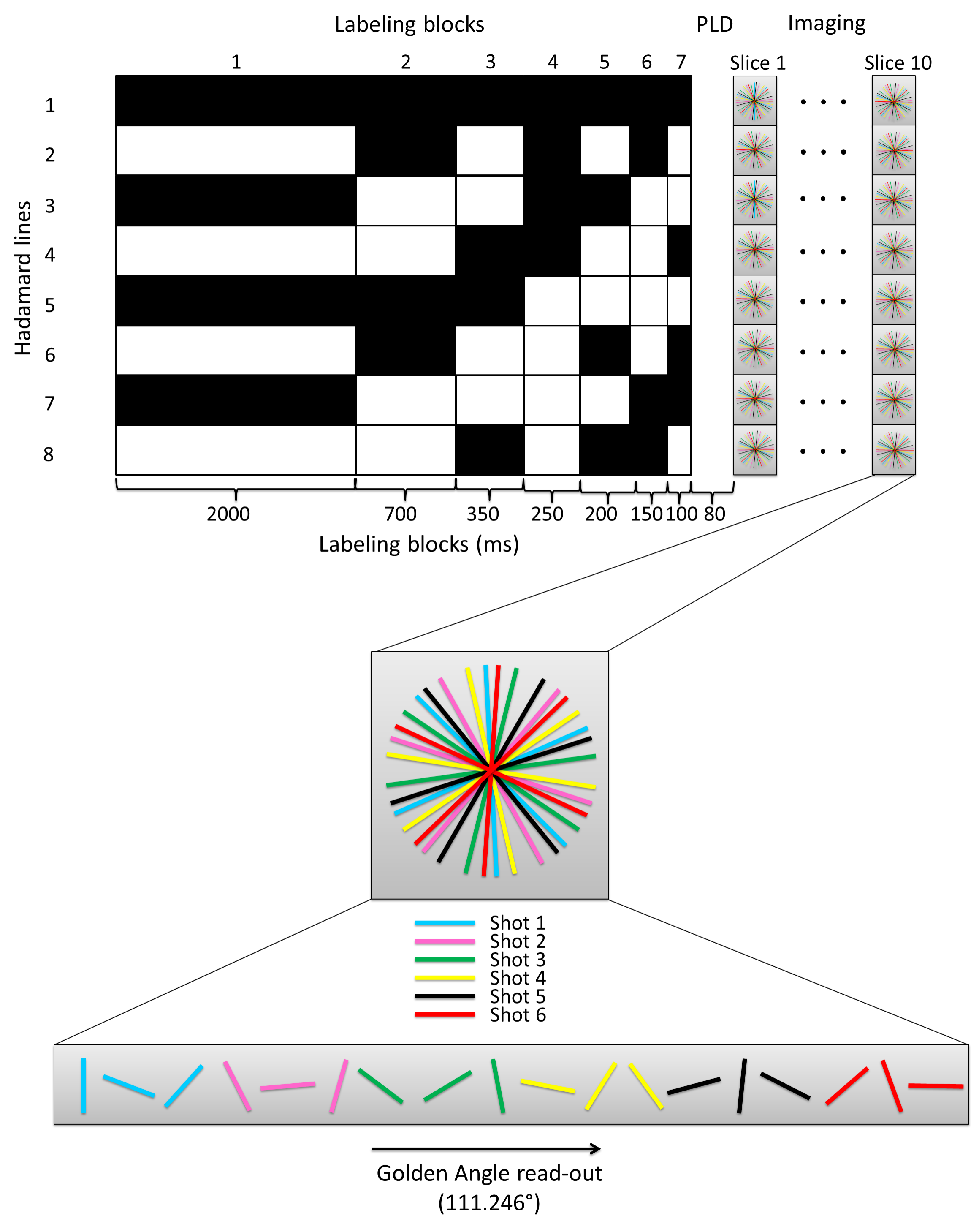
A Hadamard-8 matrix was used as the primary source for the temporal resolution. The total label duration of 3750ms was followed by a multi-shot acquisition, by which k-space was filled according to the golden angle, in multiple shots for each slice (Figure 1). For every shot, which contains a particular section (i.e. 16 spokes) of the total amount of spokes, the complete Hadamard matrix was acquired. Two FOCI pulses at 1950 and 3300ms were used for background suppression and the total scan duration was 9:39min to obtain whole brain coverage (TR/TE 4.4/1.95ms, 10 slices, matrix 256, 16 shots, shot duration 71.4ms, flip angle 20°).
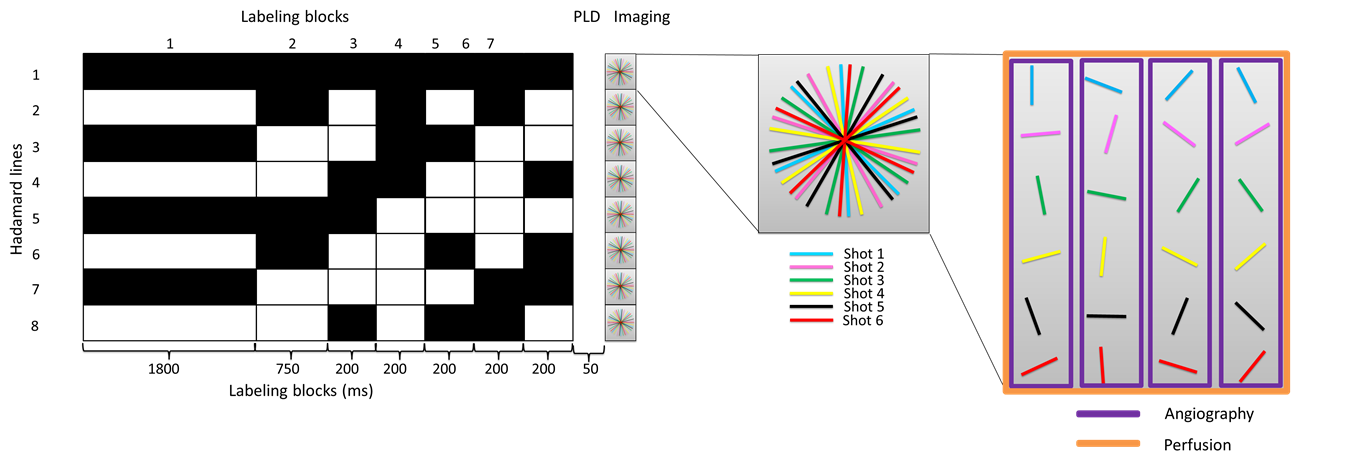
To obtain high temporal resolution angiography in combination with high quality perfusion images from a single dataset, the golden angle was used as a temporal resolution tool, while limiting the readout to a single slice(Figure 2). The total label duration was 3550ms, two FOCI pulses at 1850 and 3130ms were used for background suppression and the total scan duration was 8:06min. (TR/TE=3.6/1.55ms, matrix 224, 16 shots, flip angle 13°). Angiographic images were reconstructed at a temporal resolution of 50ms and an effective matrix of 224x224, whereas the perfusion images were reconstructed at 200ms and 70x70matrix, i.e. using only the densely sampled center of k-space.
Results
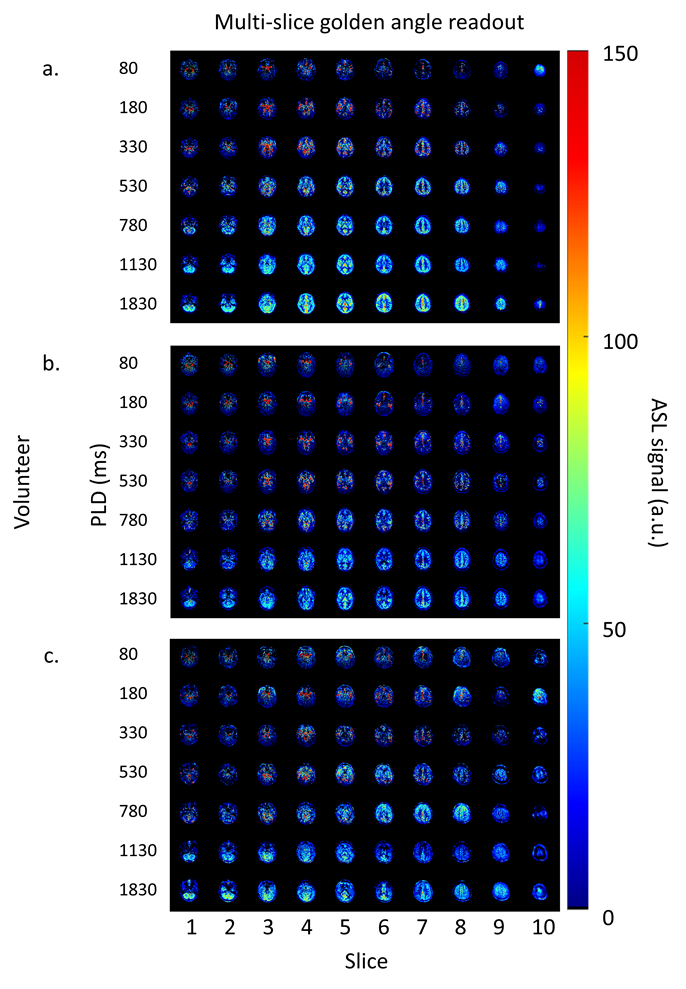
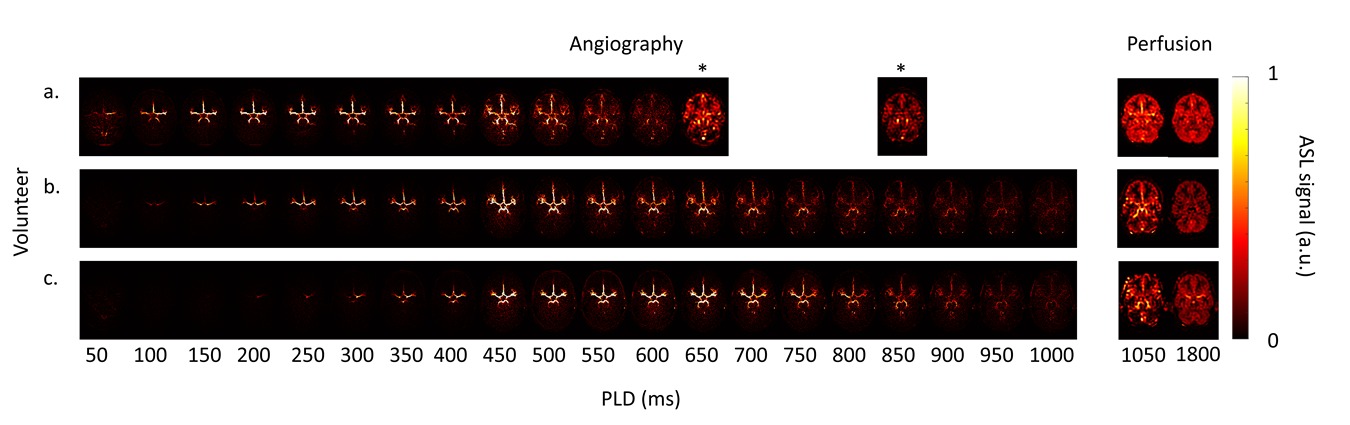
The multi-slice golden angle data of three volunteers are shown in figure 3. The temporal resolution of these acquisitions was determined by the Hadamard labeling scheme, which resulted in the following PLDs: 80, 180, 330, 530, 780, 1130 and 1830ms. The inflow of the labeled blood into the arteries, as well as the perfusion in the tissue is imaged with full brain coverage. Figure 4 shows the angiographic data at a temporal resolution of 50ms for three volunteers. At later time points, the perfusion data is reconstructed with a temporal window of 200ms, which was retrospectively chosen, using only the center of k-space. Note, blood flow in volunteer A was faster compared to the other volunteers, therefore, it was decided retrospectively to start the perfusion reconstruction (with a temporal reconstruction window of 200ms) at an earlier time-point.Discussion and Conclusion
By combining the golden angle readout with a Hadamard labeling scheme, multi-slice acquisition was easier enabled since this combination of techniques allowed for the golden angle to be focused on acquiring multiple spatial resolutions. To increase the number of slices to achieve truly whole brain coverage, simultaneously multi-slice acquisition should be introduced, which could also limit the total readout duration and thus minimize relaxation effects in the later acquired slices. By switching to single-slice acquisition, high temporal resolution angiography and high quality perfusion images were reconstructed. More importantly, the temporal window of the images could retrospectively be chosen and adjusted to the specific hemodynamics of the volunteer.Acknowledgements
No acknowledgement found.References
1. Winkelmann S, Schaeffter T, Koehler T, Eggers H, and Doessel O. An optimal radial profile order based on the golden ratio for time-resolved MRI. IEEE Transactions on medical imaging 2007;26.
2. Okell TW. Combined angiography and perfusion using radial imaging and arterial spin labelling. In proceedings 24th scientific meeting, ISMRM, Singapore, 2016. P1001.
3. Okell TW. 4D combined angiography and perfusion using radial imaging and arterial spin labelling. In proceedings 25th scientific meeting, ISMRM, Hawaï, 2017. P0675.
Figures