0247
Reconstruction of Arrhythmic Cardiac Cycles in Patients with Atrial Fibrillation1New York University School of Medicine, New York, NY, United States, 2Siemens Healthineers, Erlangen, Germany
Synopsis
Arrhythmia is often a significant challenge to acquiring diagnostic quality cardiac MRI. While discarding atypical cardiac cycles can exclude short-lived arrhythmic events, such as premature ventricular contractions (PVCs), this fails for atrial fibrillation (Afib), where subjects have an irregular cardiac cycle pattern. Harnessing the potential of the XD-GRASP MRI technique to reconstruct continuously acquired data with cardiac and respiratory phase as extra dimensions, we propose to additionally classify cardiac cycles for Afib patients according to their preload state, and simultaneously reconstruct the different types of arrhythmic cycles in a five-dimensional image space.
Introduction
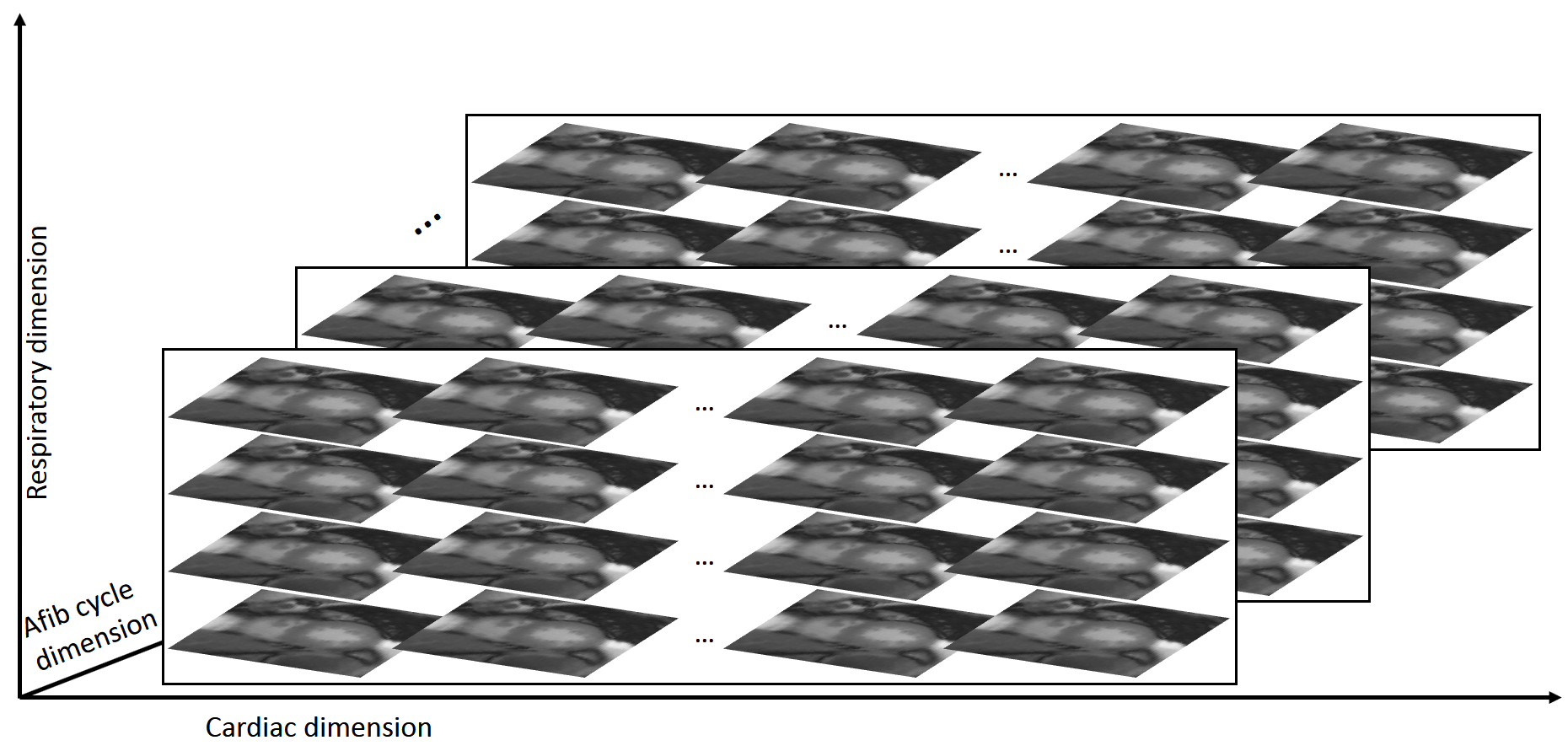
Arrhythmia can adversely affect cardiac MRI, often leading to non-diagnostic image quality. New MRI techniques allow the joint reconstruction of cardiac cycles during multiple different relative breathing phases. Self-gating (detecting cardiac cycles without electrocardiogram) allows automatic detection and classification of common arrhythmias from continuously acquired data,1 opening the way to arrhythmia-robust imaging. While discarding atypical heart cycles can benefit patients with short-lived arrhythmic events (PVCs), it fails for subjects with atrial fibrillation (Afib) (reportedly more than 1% of the population other than 60),2 who have a completely irregular cardiac cycle pattern. Instead of discarding atypical cardiac cycles, we propose to reconstruct different types of cardiac cycles as a new dimension, based on their preload state using the XD-GRASP3 technique. XD-GRASP was originally developed to reconstruct cardiac and respiratory phases. Here we add the cardiac cycle type dimension, resulting in a five-dimensional image object composed of two-dimensional image frames of different relative cardiac phase, relative breathing phase and cardiac cycle type (Fig.1).Methods
Patients underwent free-breathing continuous acquisition, using a steady-state free precession sequence, with golden-angle radial sampling scheme, for a single-slice mid-ventricular short axis cine. Imaging was performed on a 1.5T scanner (Aera, Siemens, Erlangen, Germany), TR/TE=2.8/1.4ms, FOV=320×320mm2, 128 readout points per spoke, spatial resolution 2×2mm2, slice thickness 8mm, acquisition time 2min.
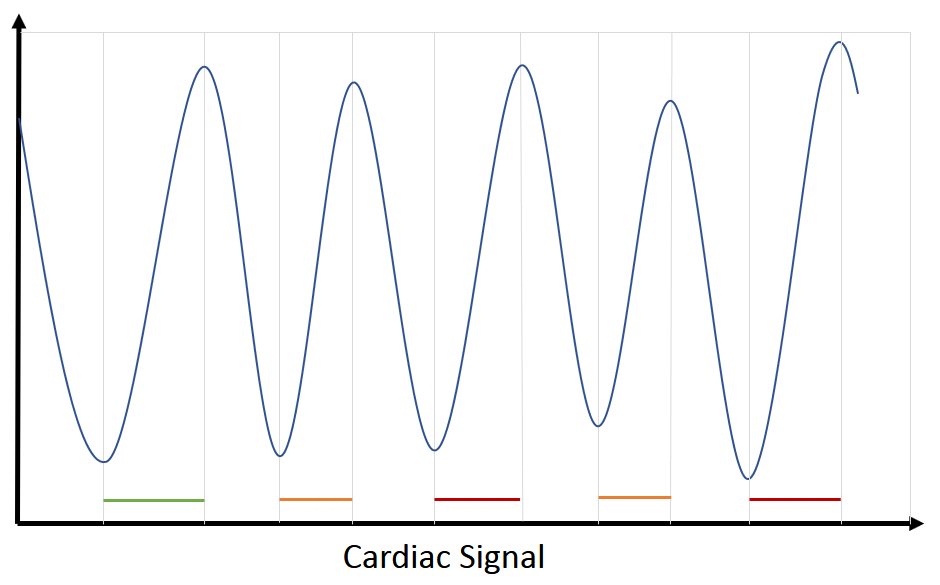
Breathing and cardiac motion-related signals were separately extracted from the image data, after a "real-time" KWIC reconstruction.4 Cardiac signal was derived from an automatically detected region around the heart. The breathing motion signal was extracted from an automatically determined image block with strongest periodic signal in the breathing range (0.2-0.4Hz). Data was grouped into 5 respiratory phases using probabilistic k-means, which minimizes the intra-class variance.
Classifying cardiac cycles by length of RR interval is common but suboptimal, as it may group together cycles with different cardiac state. It was shown that, in Afib, cardiac function can be predicted by previous cycle dynamics.5 Since the P wave is absent, the amount of preload of the LV is mainly determined by the length of diastole during the previous cardiac cycle (LD). The preload is, in turn, correlated with the next cycle’s ejection fraction. Based on this observation, we use LD-dependent preload as a measure of self-similarity for cardiac cycles in Afib, which ensures a similar blood pool size for corresponding cardiac cycles. Cardiac cycles were thus classified by their preload state, computed as LD (Fig.2.). The number of distinct classes was heuristically determined from the LD distribution (3 to 6). To facilitate joint multidimensional reconstruction, reconstructed cardiac cycles were equally resampled into 15 cardiac phases.
After rebinning data in the three extra dimensions (cardiac phase, arrhythmic cycle type, and respiratory phase), each reconstructed image frame has a variable degree of undersampling (30 to 80 spokes per frame). Joint reconstruction was performed using XD-GRASP by iterative optimization.3 The optimal “sparsifiable” multidimensional image $$$d$$$ for all acquired data $$$y$$$ was found by:$$d=argmin\parallel E(d)-y\parallel_2+\lambda_1\phi_d\parallel T_1(d)\parallel_1+\lambda_2\phi_d\parallel T_2(d) \parallel_1w_2+\lambda_3\phi_d\parallel T_3(d)\parallel_1$$where $$$E$$$ is the sampling function (including coil sensitivities), $$$T_{1,2,3}$$$ are total variation functions computed separately over the cardiac, respiratory, and cardiac cycle type dimensions, as sparsity transforms, and $$$\lambda_{1,2,3}$$$ are regularizing parameters. The probabilistic result of k-means classification was used to implement weighted view sharing along the respiratory dimension $$$w_2$$$, for the highly undersampled respiratory states. To account for the variable undersampling, the additional $$$\phi_d=1/n_s$$$ weighting term is inversely proportional to the number of spokes $$$n_s$$$ in each frame.
Results and Discussion
The continuously acquired data from 3 patients was reconstructed with the described method, resulting in a 5D image object consisting of 2D frames along cardiac phase, respiratory phase and cycle preload dimensions. The variability of different reconstructed arrhythmic cycles can be inspected for all cardiac phases across their corresponding frames, as shown in Fig.3. for a given end-expiration position. Cardiac cycles are sorted by their initial preload state, correlated with the initial amount of blood in the LV at end-diastole. We observed that larger preload corresponds to a more vigorous contraction during systole. By separately reconstructing different arrhythmic cycles with varying preload, despite reconstructing more separate cycles with higher undersampling, the image sharpness is qualitatively improved compared to previous 4D XD-GRASP reconstruction (only cardiac and respiratory dimensions), as shown in Fig.4.Conclusion
We have shown that reconstruction of different types of cardiac cycles in patients with Afib is possible using 5D XD-GRASP, with improved image quality. The ability to reconstruct cardiac cycles grouped by the length of the previous filling phase (determined from an image-derived cardiac signal) is a promising approach to better understand functional variability during arrhythmia.Acknowledgements
No acknowledgement found.References
1. Piekarski E, Chitiboi T, Ramb R, Feng L, Axel L. Use of self-gated radial cardiovascular magnetic resonance to detect and classify arrhythmias (atrial fibrillation and premature ventricular contraction). JCMR 2016; 18(1):83.
2.Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke 1991;22:983-988
3. Feng L, Axel L, Chandarana H, Block KT, Sodickson DK, Otazo R. XD‐GRASP: Golden‐angle radial MRI with reconstruction of extra motion‐state dimensions using compressed sensing. MRM 2016; 75(2):775-88.
4. Song HK, Dougherty L. k‐Space weighted image contrast (KWIC) for contrast manipulation in projection reconstruction MRI. MRM 2000;44(6):825-32.
5. Rawles JM. A mathematical model of left ventricular function in atrial fibrillation. International journal of bio-medical computing. 1988 Oct 1;23(1-2):57-68.
Figures