0242
3D-Patch-Based Low-Rank Reconstruction (PROST) for Highly-Accelerated CMRA Acquisition1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare Limited, Frimley, United Kingdom
Synopsis
Free-breathing coronary MR angiography (CMRA) has shown great potential to visualize coronary stenosis. Three-dimensional (3D) CMRA, however, remains time consuming because a large amount of data is needed to accurately visualize all major coronary arteries. Scan acceleration using compressed sensing (CS) reconstruction has successfully been applied to coronary artery imaging. For high acceleration factors, however, CS-based techniques suffer from residual aliasing artifacts which compromise the diagnostic value of the reconstructed image. We propose a new 3D-patch-based reconstruction that exploits the complex 3D anatomy of the coronary arteries in an effective low-rank framework, which combined with 100% respiratory efficiency enables high-quality isotropic Cartesian CMRA images in ~3 mins.
PURPOSE
Free-breathing coronary MR angiography (CMRA) has shown significant potential to noninvasively visualize coronary stenosis, which is of vital importance for the diagnosis of coronary artery disease. Three-dimensional (3D) whole-heart CMRA, however, remains time consuming as a large amount of data is needed to accurately visualize the major coronary arteries with adequate spatial resolution for quantification of luminal stenosis. Scan acceleration using reduced data sampling and compressed sensing (CS) reconstruction has successfully been applied to CMRA1. For high acceleration factors, however, CS-based techniques suffer from residual aliasing artifacts, which compromise the diagnostic value of the reconstructed image. Two-dimensional (2D) patch-based reconstructions2 have been proposed as an alternative strategy to recover image information by exploiting 2D spatial redundancies in the image. In this study, we propose a new 3D-patch-based reconstruction which exploits the complex 3D anatomy of the coronary arteries in a low-rank framework to further accelerate the scan. We combine this approach with 100% respiratory efficiency to enable high-quality 1.2mm3 isotropic Cartesian CMRA images in less than 3mins.METHODS
Acquisition: A prototype undersampled Cartesian variable density 3D spiral-like Cartesian sampling (VD-CASPR3) was implemented on a 1.5T scanner (Siemens, Aera). A 2D image-navigator precedes each VD-CASPR acquisition to enable beat-to-beat 2D translational respiratory motion estimation/correction without data rejection4. Five healthy volunteers (30±4 years) underwent free-breathing CMRA. Data were acquired in mid-diastole with an ECG-gated 3D bSSFP sequence, 18-channel body and 32-channel spine coils, fat-saturation and T2-preparation pulses (FOV=320x320x120mm3,TR/TE=3.35/1.47ms,FA=90°,bandwidth=890Hz/pixel,T2-preparation duration=40ms) with 1.2mm3 isotropic resolution and undersampling factors of 5 and 9. An additional free-breathing fully-sampled Cartesian acquisition was performed with identical imaging parameters for comparison purposes.
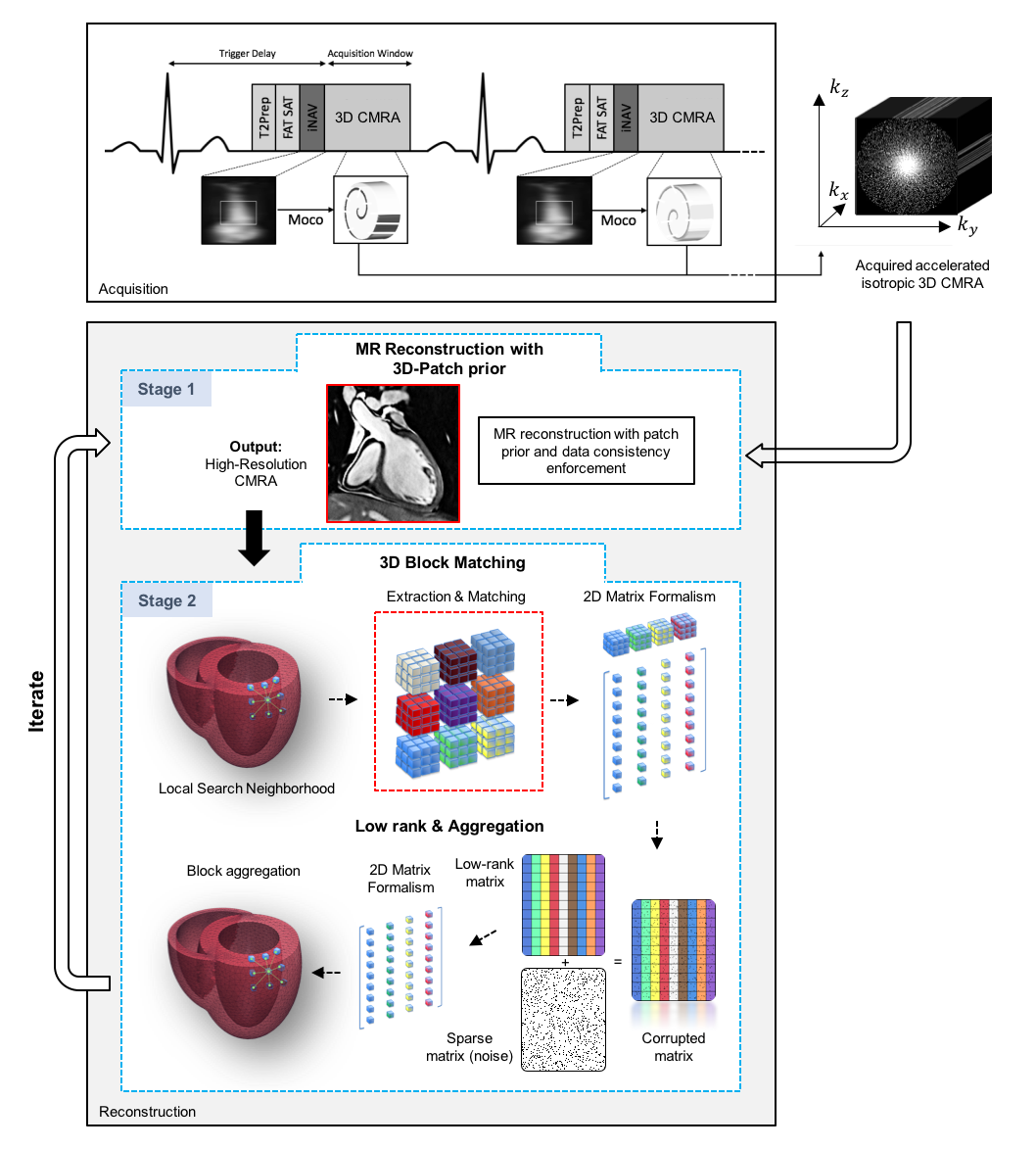
Reconstruction: The proposed 3D-Patch-based low-rank ReconstructiOn with Self-similariTy learning (3D-PROST) integrates anatomical structure information from 3D patch neighborhoods through sparse representation, exploiting the redundancy of 3D patches in the acquired data itself. The optimization problem iterates between a data consistency step, which reconstructs a high-resolution isotropic MR volume , and a low-complexity 3D patch-based denoising step, which provides a reconstructed volume as prior for the next step (Fig.1). The two sub-problems are solved iteratively in an effective Augmented Lagrangian (AL) scheme: $$\mathcal{L}\left (x,\alpha \right ):=\underset{x,\alpha}{\mathrm{argmin}}\,\frac{1}{2}\Vert Ex-\rho\Vert_2^2+\lambda\Vert\alpha\Vert_0+\frac{\mu}{2}\Vert x-D\alpha-b\Vert_2^2$$ where $$$E$$$ is the encoding operator (including coils, Fourier operator and sampling), $$$\rho$$$ denotes the undersampled data, $$$b$$$ denotes the AL multiplier, $$$D$$$ is the patch-grouping operator and $$$\alpha$$$ are the associated sparse coefficients. The $$$l_0$$$ norm counts the number of non-zeros element in $$$\alpha$$$, and $$$\lambda>0$$$ controls the strength of sparsity. The two problems are:
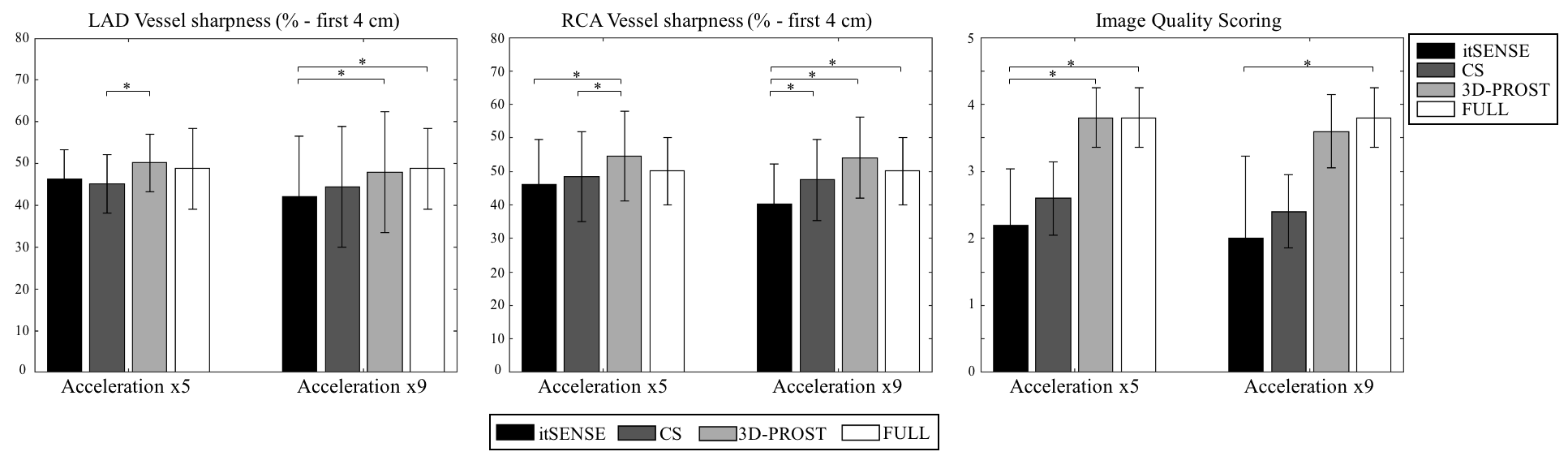
1) MR reconstruction (Fig.1-Stage 1) is performed using a conjugate gradient (CG) descent and uses the 3D denoised volume ($$$\omega=D\alpha$$$) obtained from Stage 2 as prior knowledge ($$$\omega_0=b_0 = 0$$$):$$\mathcal{L}_1\left (x\right):=\underset{x}{\mathrm{argmin}}\,\frac{1}{2} \Vert Ex-\rho\Vert_2^2+\frac{\mu}{2}\Vert x-\omega-b\Vert_2^2$$ 2) A 3D block-matching2,5 algorithm is used to exploit redundancies in the volume $$$x$$$. The L-most similar 3D blocks to a reference block are extracted, vectorised and concatenated into a 2D matrix. Sparsity of this low-rank matrix is enforced using complex SVD and by hard thresholding the singular values below a specific threshold $$$\lambda$$$. The denoised 3D blocks are then placed back to their original positions by averaging (Fig.1-Stage 2): $$\mathcal{L}_2\left(\alpha\right):=\underset{\alpha}{\mathrm{argmin}}\,\frac{\mu}{2}\Vert x-D\alpha-b\Vert_2^2+\lambda\Vert\alpha\Vert_0$$ Implementation and Analysis: The following parameters were empirically selected to provide the best reconstruction quality: patch_size=5x5x5voxels, window_search=14x14x14voxels, AL_iterations=4, CG_iterations=30,$$$\lambda=4$$$,$$$\mu=1$$$. The proposed approach was compared to conventional zero-filled (ZF), iterative-SENSE, and Wavelet-based CS6 reconstructions. Vessel sharpness of the right and left coronary arteries was measured using SoapBubble7, and image quality scoring was performed by two experts.
RESULTS
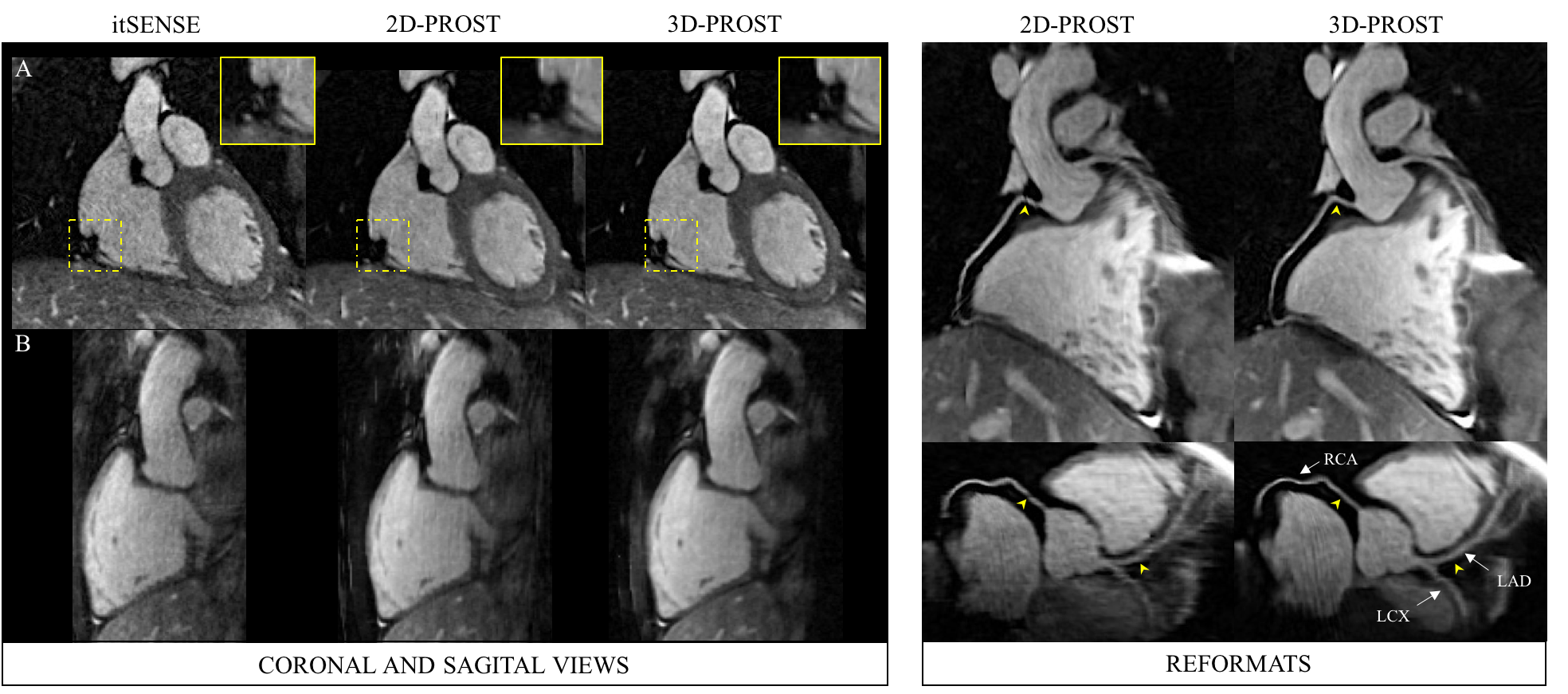
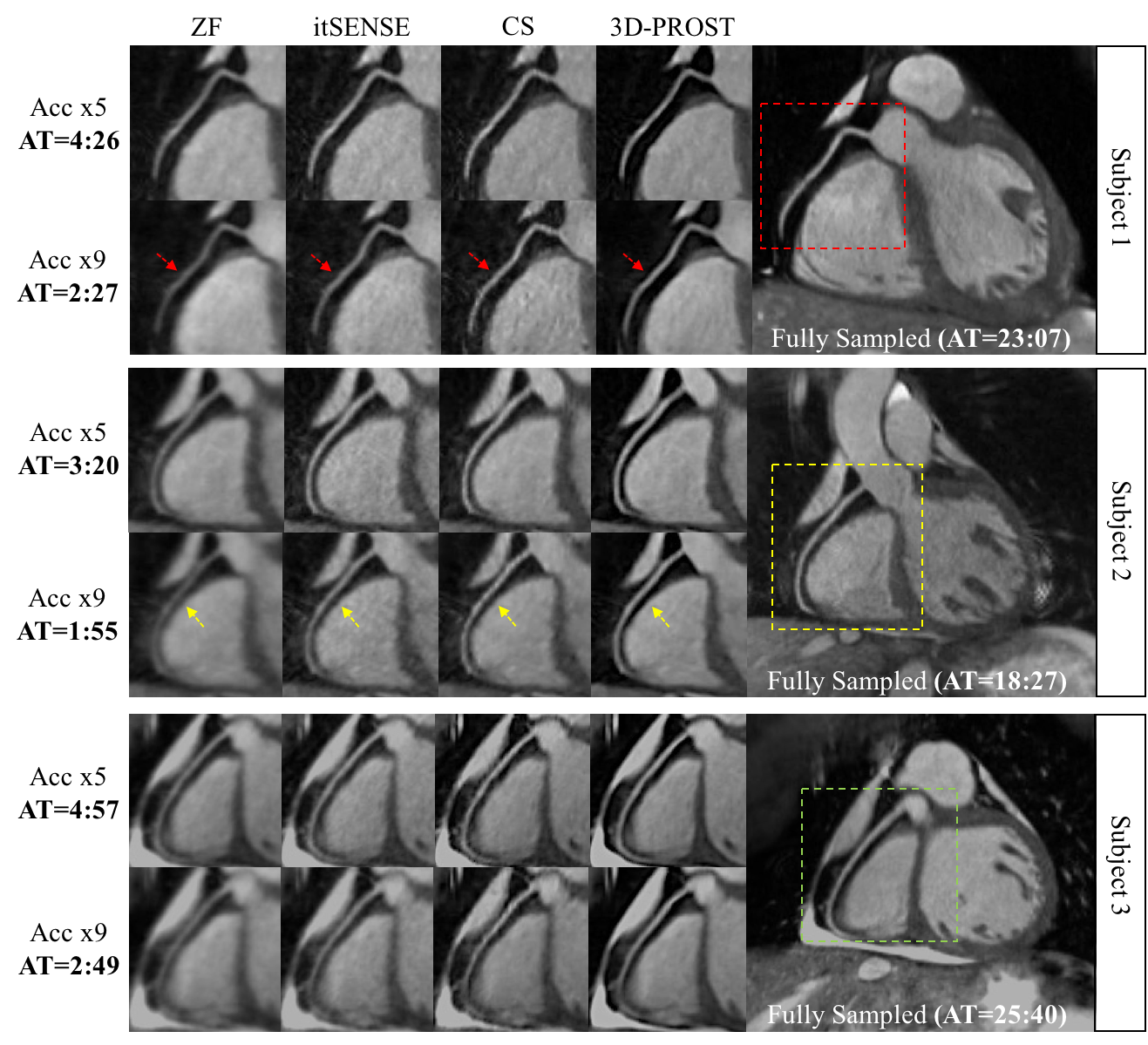
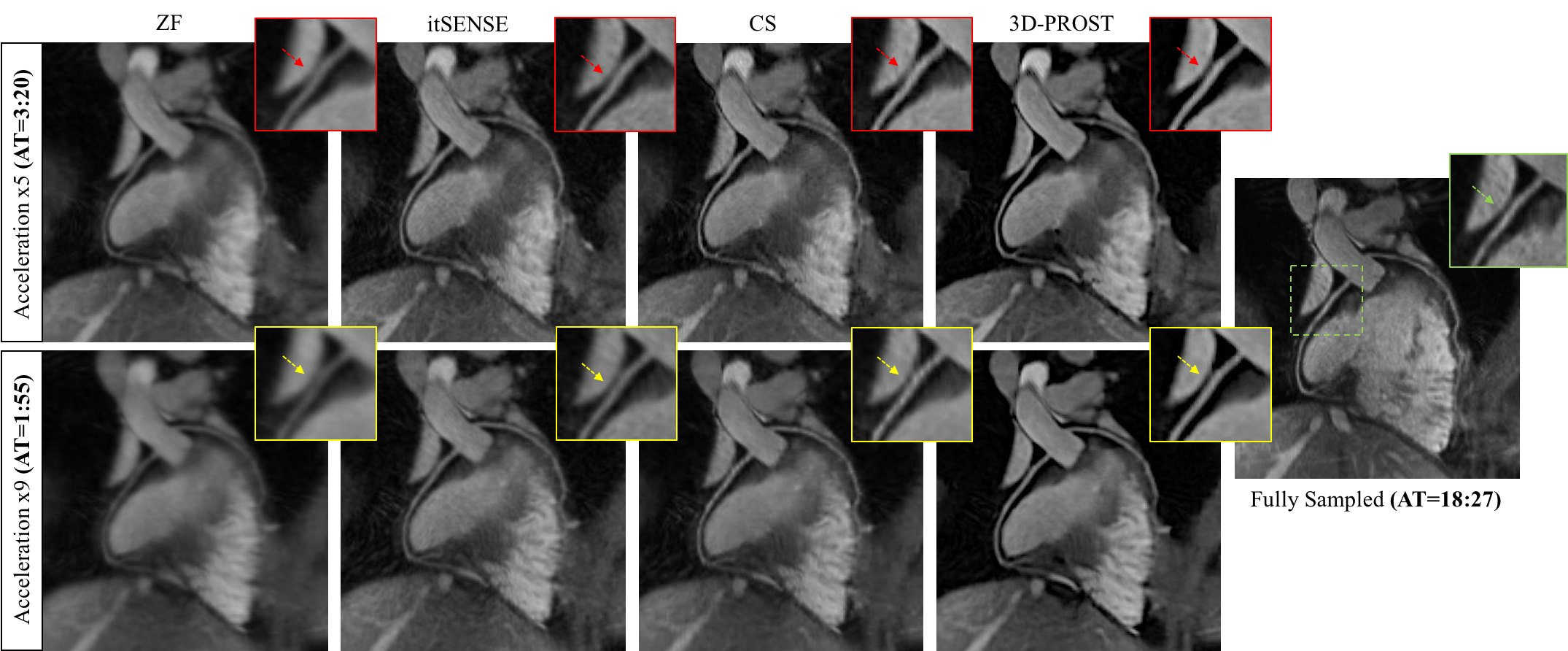
The average total acquisition time (m:s) was 25:46 for the fully sampled acquisition, 4:02 and 2:16 for accelerations of 5x and 9x, respectively. All scans were performed with 100% navigator effiency. The average total reconstruction time was ~2min (16cores/256Gb RAM). The impact of integrating 3D information in the patch-based reconstruction, in comparison to exploiting 2D redundancy, is shown in Fig.2. 3D-PROST provides better reconstruction results than its 2D variant, with high signal-to-noise ratio (SNR) and excellent contrast, reducing the apparent streaking artifacts which could be misinterpreted as stenosis in the reformatted images (Fig.2-right,arrows). 3D-PROST reconstruction provided higher image quality scores than ZF, iterative-SENSE and CS for both accelerations (Figs.3-4) with image quality and vessel sharpness comparable to the fully-sampled reference (Table 1).CONCLUSION
Free-breathing whole-heart 3D coronary images acquired in ~3 min with 1.2mm3 isotropic resolution were successfully obtained using 3D-PROST with 100% respiratory efficiency. 3D-PROST proved to be superior to iterative-SENSE, CS and 2D-patch based reconstructions, offering several potential advantages: i) high-SNR and high-resolution CMRA reconstruction by exploiting the inherent 3D redundancy of the coronary anatomy structure, ii) short scan times leading to both improved patient comfort and reduction of respiratory motion artifacts, iii) fast and efficient implementation leading to clinically feasible reconstruction times.Acknowledgements
This work was supported by an EPSRC programme and project Grant (EP/P001009/1 and EP/P007619/1) and FONDECYT N° 1161051.References
1. Akçakaya M, et al. Accelerated isotropic sub-millimeter whole-heart coronary MRI: compressed sensing versus parallel imaging. Magnetic resonance in medicine. 2014;71(2):815-822.
2. Akçakaya M, et al. Low-dimensional-structure self-learning and thresholding (LOST): Regularization beyond compressed sensing for MRI reconstruction. Magnetic resonance in medicine. 2011;66(3):756-767.
3. Prieto C, et al. Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. Journal of magnetic resonance imaging. 2015;41(3):738-746.
4. Henningsson M, et al. Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Magnetic resonance in medicine. 2012;67(2):437-445.
5. Dabov K, et al. Image denoising by sparse 3-D transform-domain collaborative filtering. IEEE Transactions on Image Processing. 2007;16(8):2080-2095.
6. Lustig M, et al. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magnetic resonance in medicine. 2007;58(6):1182-1195.
7. Etienne A, et al. “Soap-Bubble” visualization and quantitative analysis of 3D coronary magnetic resonance angiograms. Magnetic resonance in medicine. 2002;48(4):658-66.
Figures