0241
Presence of non-hypervacular hypointense nodule on hepatobiliary phase of gadoxetic acid enhanced MR: Risk of tumor recurrence after curative treatment for small single nodular HCC and guidance for selection of treatment option1Radiology, Seoul National University Hospital, Seoul, Republic of Korea
Synopsis
Presence of non-hypervascular hypointense nodule on hepatobiliary phase of gadoxetic acid enhanced liver MR can stratify the risk of tumor recurrence after curative treatment for small single nodular HCC equal to or less than 3cm.
Purpose: To evaluate whether presence of non-hypervascular hypointense nodue (NHHN) on hepatobiliary phase of gadoxetic acid enhanced liver MR could predict tumor recurrence after curative treatment for small single nodular HCC using either surgical resection or radiofrequency ablation (RFA) and could guide the selection of treatment option
Materials and Methods: A total of 396 patients with single nodular HCC ≤ 3 cm treated by either surgical resection (n=157) or RFA (n=239) were included in this study. All patients underwent gadoxetic acid enhanced liver MR before treatment for HCC. After treatment, overall and recurrence-free survival (RFS) was estimated using Kaplan-Meier method. The presence of NHHN on hepatobiliary phase was assessed, and its prognostic implication was evaluated by using Cox-proportional hazard regression model.
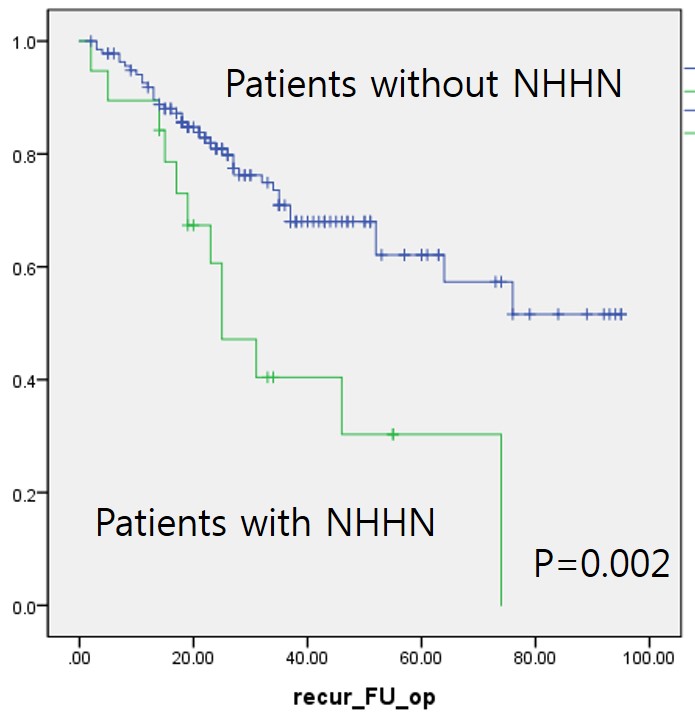
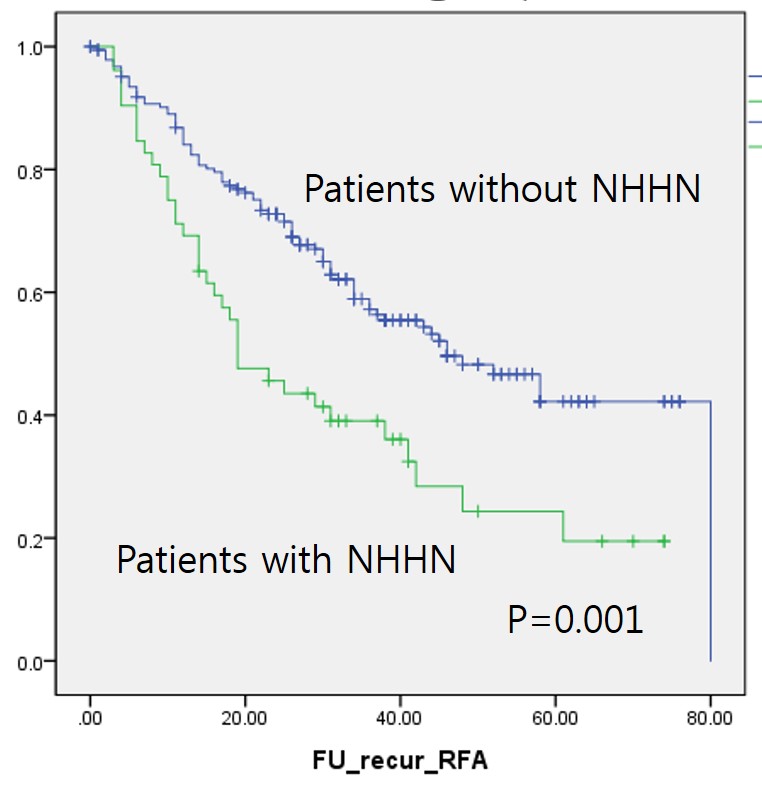
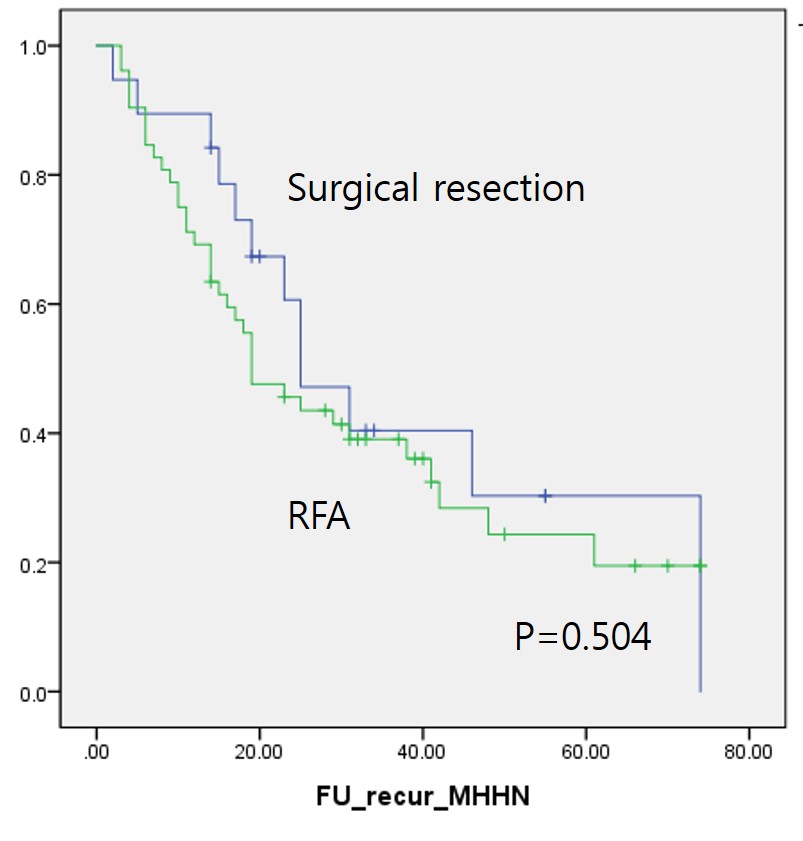
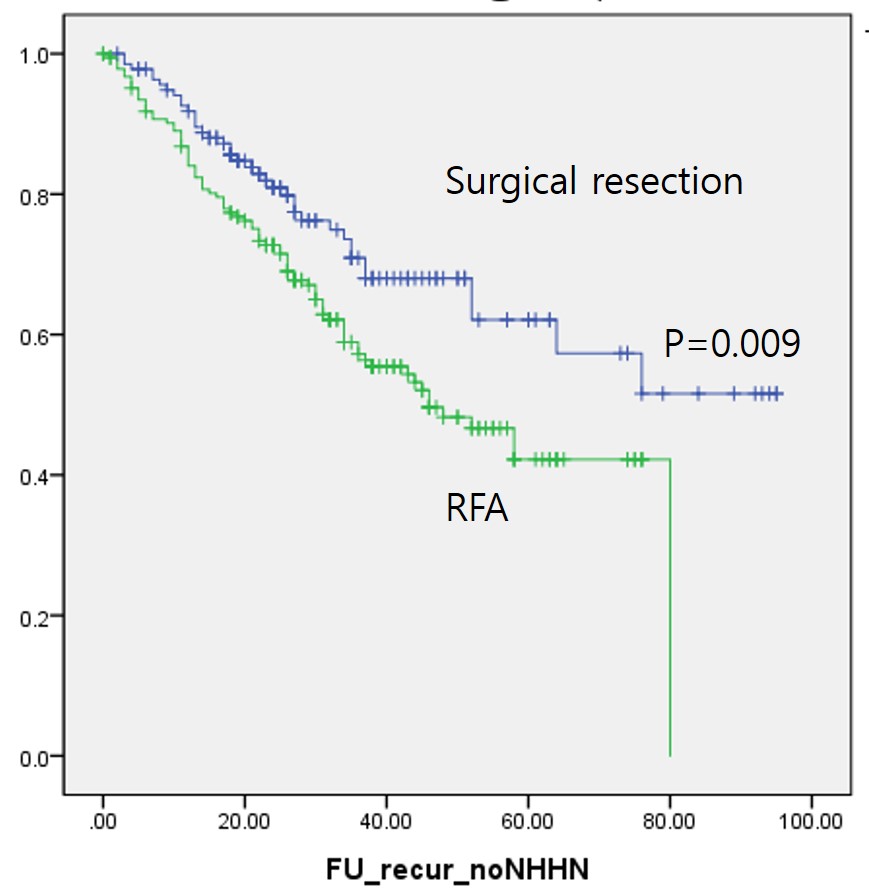
Results: The 5-year estimated overall survival was not significantly different between surgical resection and RFA (P=0.461). The estimated 5-year RFS was 57.7% in surgical resection group and 38.5% in RFA group, respectively: this difference was statistically significant (P=0.002). Presence of NHHN was significant predictive factor for RFS in both surgical resection group (62.1% 5-year RFS in 138 patients without NHHN vs. 30.3% in 19 patients with NHHN; P=0.002, Hazard ratio [HR]=2.74) and RFA group (42.2% 5-year RFS in 187 patients without NHHN vs. 24.3% in 52 patients with NHHN; P=0.001, HR=1.97). In 71 patients with NHHN, there was no significant difference in RFS between surgical resection and RFA (30.3% 5-year RFS in surgical resection vs. 24.3% in RFA, P=0.504). However, when NHHN was absent, 5-year RFS was 62.1% in 138 patients treated by surgical resection whereas 42.2% in 187 patients treated by RFA: this difference was statistically significant (P=0.009, HR=1.67).
Conclusion: Presence of NHHN was significant predictive factor for tumor recurrence after both surgical resection and RFA for single nodular HCC ≤ 3 cm, and surgical resection could be a preferred treatment option for patients without NHHN as surgical resection would provide significantly better RFS than RFA for these patients.
Acknowledgements
No acknowledgement found.References
No reference found.Figures