0129
Ferumoxytol-enhanced MRI: Early Results in Solid Organ Masses.Puja Shahrouki1,2, Woo Kyoung Jeong1,3, Steven S. Raman1, Ely R. Felker1, David S. Lu1, and J. Paul Finn1,2
1Department of Radiological Sciences, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States, 2Diagnostic Cardiovascular Imaging Laboratory, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States, 3Department of Radiology and Imaging Sciences, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea
Synopsis
Whereas experience is growing rapidly with the use of ferumoxytol as an alternative to gadolinium based contrast agents (GBCA) for cardiovascular imaging, little has been reported about its potential for imaging of solid organs. The pharmacokinetics and relaxometry of ferumoxytol are very different to all of the available GBCA, and data are lacking about its behavior in extracranial solid organ lesions. We report early results of FE-MR imaging in a variety of solid organ mass lesions with focus on enhancement characteristics and clinical impact.
Introduction
To date, the role of ferumoxytol-enhanced MR (FE-MR) in detection and characterization of solid organ mass lesions is still unexplored. This is increasingly relevant since the off-label use of ferumoxytol is increasing as an alternative contrast agent in patients with renal impairment or other contraindications to gadolinium based contrast agents. The evaluation of incidental mass lesions on FE-MR is challenging especially with limited published experience elucidating the behavior of common lesions with FE-MR. In this study we show the early results of FE-MR imaging in a variety of solid organ mass lesions with focus on its technique, enhancement characteristics and clinical impact.Methods
In this IRB-approved and HIPAA-compliant study, adult patients with retrospectively identified solid organ non CNS, body mass lesions on FE-MR were analyzed. The primary imaging indications for FE-MR were either vascular (n=22), infectious (n=1) or oncologic (n=18). The imaging sequences included pre- and post T2 weighted Half-Fourier Acquisition Single-shot Turbo spin Echo (HASTE), pre- and post T1 weighted fat-suppressed 3D gradient echo, and high resolution MRA. Comparative imaging and biopsies were available for review. Retrospective chart review was carried out to determine the need for additional imaging and if biopsies or autopsies supported imaging findings.Results
The study cohort comprised 41 adult patients who underwent FE-MR (age range 19 to 89 years, 56 % male), with 42 solid organ lesions (Table 1). The signal enhancement characteristics of the lesions were studied during the steady state distribution of ferumoyxtol (n=41), and in addition studied for dynamic enhancement characteristics in a subset (n=22). Two representative cases are illustrated in Figure 1 and 2, which include steady-state and dynamic HASTE imaging. Benign lesions in the abdominal organs including cysts in the liver, kidney, spleen and pancreas, and hepatic and splenic hemangiomas, were diagnosed with high confidence. Of the 18 patients undergoing FE-MR for oncological indications, single lesions in three patients (1 renal, 1 liver and 1 splenic) were confidently excluded as malignant without the need for additional imaging and none of these have been found to be malignant on follow up. In total, masses in 18 patients were suspected of being malignant, where 13 masses were either known from before or had high suspicion prior to FE-MR imaging, and 5 were incidental. In these 18 lesions with FE-MR imaging features of malignancy, eight patients had biopsies or autopsies of the primary lesion site or primary malignant site if assumed to be metastatic, and biopsy or autopsy supported a malignant diagnosis in all patients.Conclusion
Early results of FE-MR in solid organs show that ferumoxytol is a useful tool in characterizing both benign and malignant mass lesions. By analyzing the enhancement characteristics on T1-weighted and T2-weighted images, it was possible to differentiate between benign and malignant lesions in a high proportion of cases. Our findings suggest that ferumoxytol may add diagnostic value for diagnosis of solid organ mass lesions in patients where GBCA are contraindicated.Acknowledgements
No acknowledgement found.References
1. Toth GB, Varallyay CG, Horvath A, et al. Current and potential imaging applications of ferumoxytol for magnetic resonance imaging. Kidney Int. 2017.Figures

Figure 1.
37 year old male with renal failure and
undiagnosed angiosarcoma of the left arm.
Reconstructed 3D volume rendered steady-state MR
(a), thin MIP projection (b) and post-contrast HASTE (c) show an extensive, heterogeneously enhancing solid mass lesion
(green arrows) in the left upper arm with pathological fracture of the left
humerus. Positive enhancement on
T1-weighted images is reflected by negative enhancement on T2-weighted images;
a unique property of ferumoxytol.
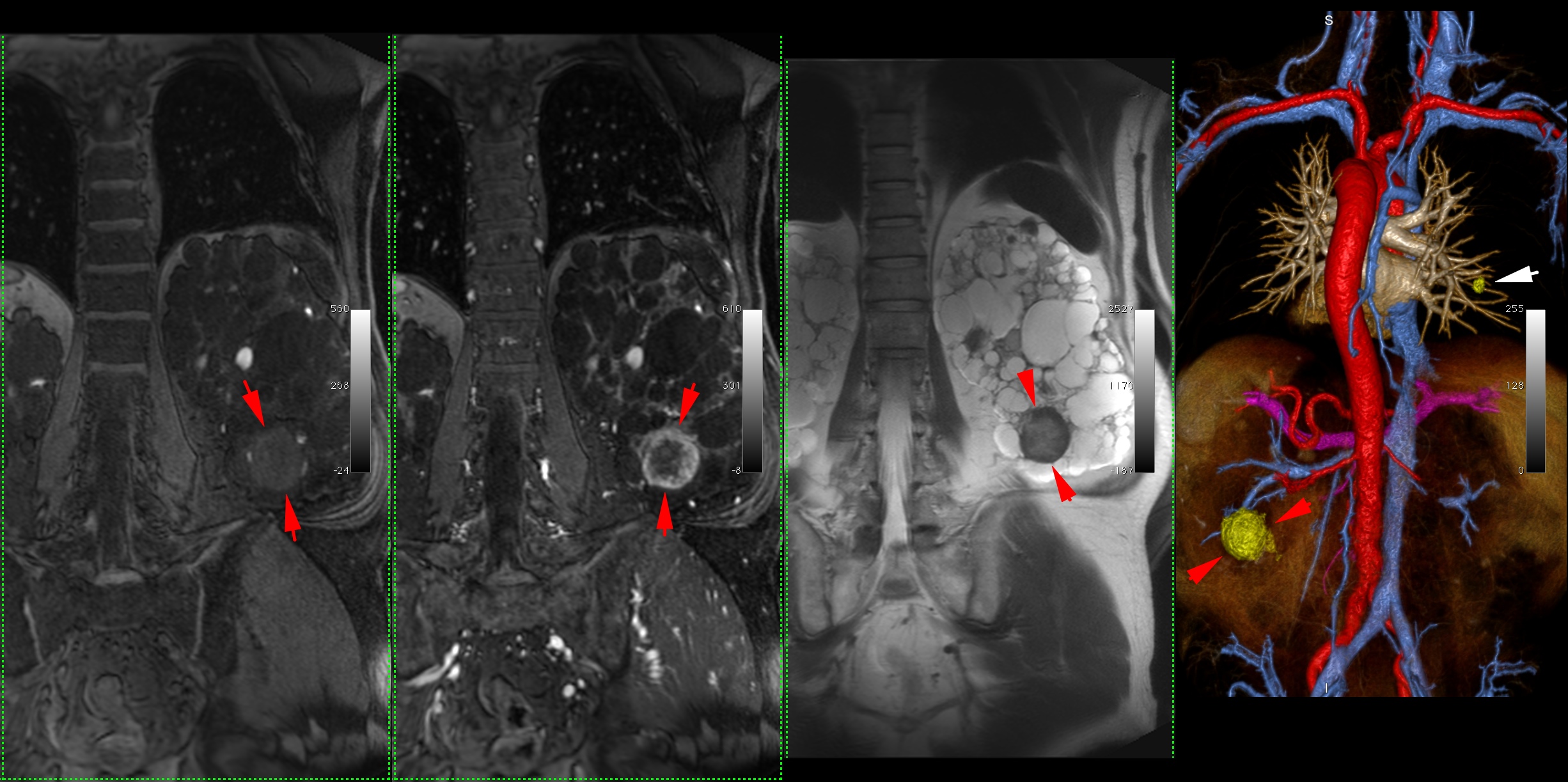
Figure 2. 71-year-old male with polycystic kidney disease
and a suspicious renal mass. T1 pre-contrast VIBE
(a), T1 post-contrast VIBE (b), T2 post-contrast HASTE (c), and reconstructed 3D MRA (d) show a peripherally enhancing (red arrows) hypervascular, solid mass in the inferior pole
of the left kidney due to renal cell carcinoma. The white arrow points to an incidental stable lung lesion.

Table 1. Identification of solid organ mass lesions.