0085
QSM identifies pro-inflammatory iron-positive MS lesions1Radiology, Weill Cornell Medical College, New York, NY, United States, 2Neurology, Yale University, New Haven, CT, United States
Synopsis
Multiple sclerosis is an autoimmune disorder whose demyelinated plaques may be connected with elevated iron. We combined quantitative susceptibility mapping (QSM) with histopathological techniques to quantify iron, macrophages/microglia, and pro/anti-inflammatory markers to demonstrate that regions of high susceptibility on QSM correspond to pro-inflammatory iron-positive macrophages/microglia. QSM is therefore a valuable clinical tool to identify smoldering lesions not visible using conventional MRI techniques.
Introduction
MS is a chronic inflammatory disease of the central nervous system characterized by formation of demyelinating lesions. Acutely demyelinated lesions have a compromised blood brain barrier and can therefore be visualized with contrast-enhanced T1-weighted imaging (1). In chronic lesions in which the BBB has resealed, ongoing chronic inflammation can no longer be monitored. Given the evidence for iron accumulation in macrophages/microglia at the rim of chronic active lesions (2), the use of QSM is an attractive alternative for monitoring inflammatory activity behind a closed BBB. We used QSM and immunohistochemistry to demonstrate that QSM identifies chronic active lesions with pro-inflammatory iron-laden macrophages/microglia.
Methods
Brain slabs from patients with MS were obtained from the Rocky Mountain MS Center (RMMSC, Colorado, USA) and scanned on a 3T clinical MRI scanner (GE Healthcare, Wisconsin, USA) using an 8-channel coil. A T2FLAIR sequence (0.8 x 0.8 x 0.6 mm3, TE = 160 ms, TR = 9.6 s, bandwidth = ± 62.5 kHz) and 3D-gradient echo (GRE) sequence (0.6 x 0.6 x 0.6 mm3, TE1 = 4.3 ms, ΔTE = 4.8 ms, # TE = 11, TR = 74.2 ms, bandwidth = ± 62.5 kHz, 3 orientations) were used for QSM multiple orientation reconstruction (COSMOS) (Liu et al., MRM 2009). After scanning, lesions were paraffin embedded, sectioned into 5µm thick sections, and subjected to Perls’ stain (iron) and antibody labeling against: myelin basic protein (MBP; myelin), CD68 (macrophages and microglia), iNOS (M1), Ferritin (M1), MerTK (M2), and CD206 (M2). Slides were scanned with a digital scanner (Mirax). For each lesion, ROIs were delineated in the NAWM, lesion center, and lesion rim. Positive cells were counted manually and normalized to determine linear density.
Results
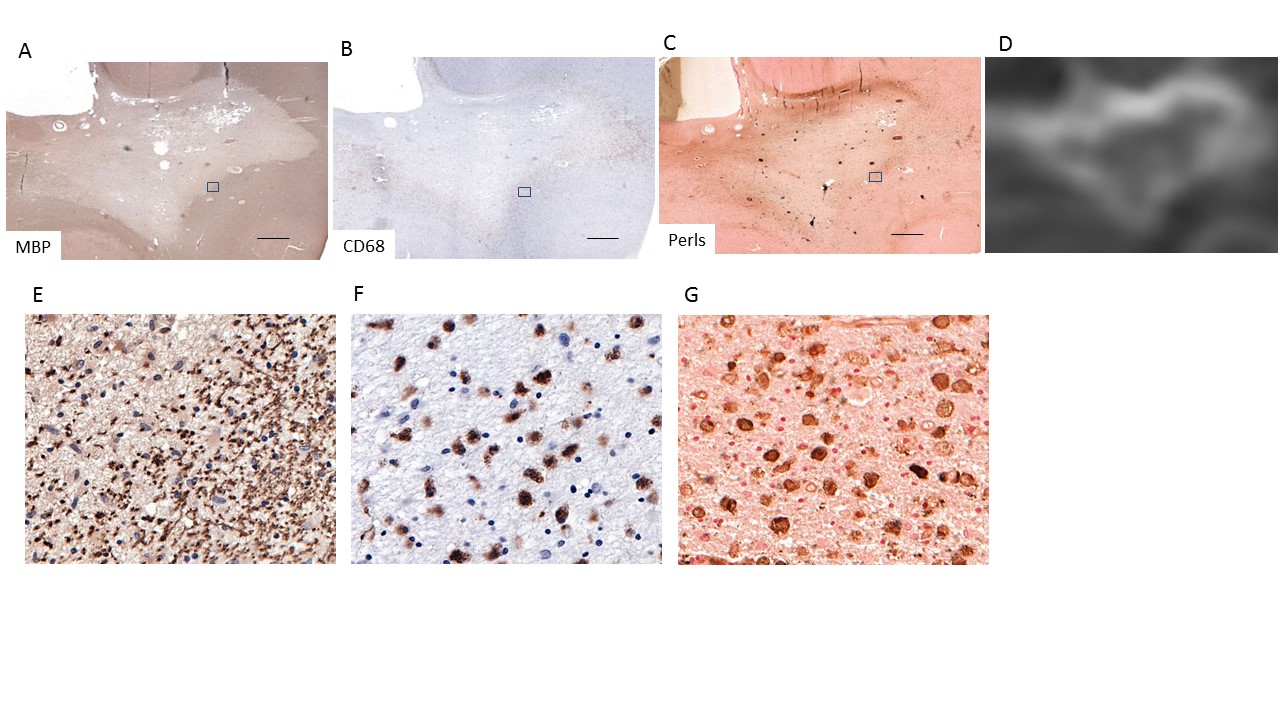
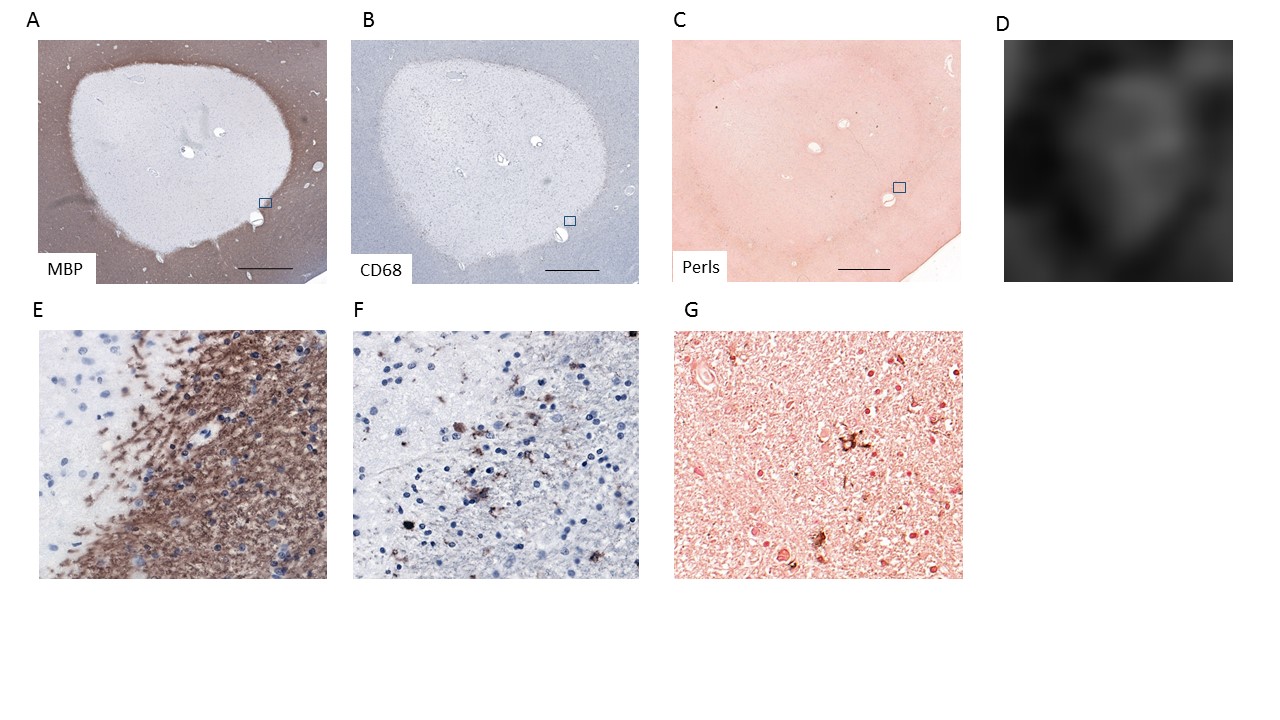
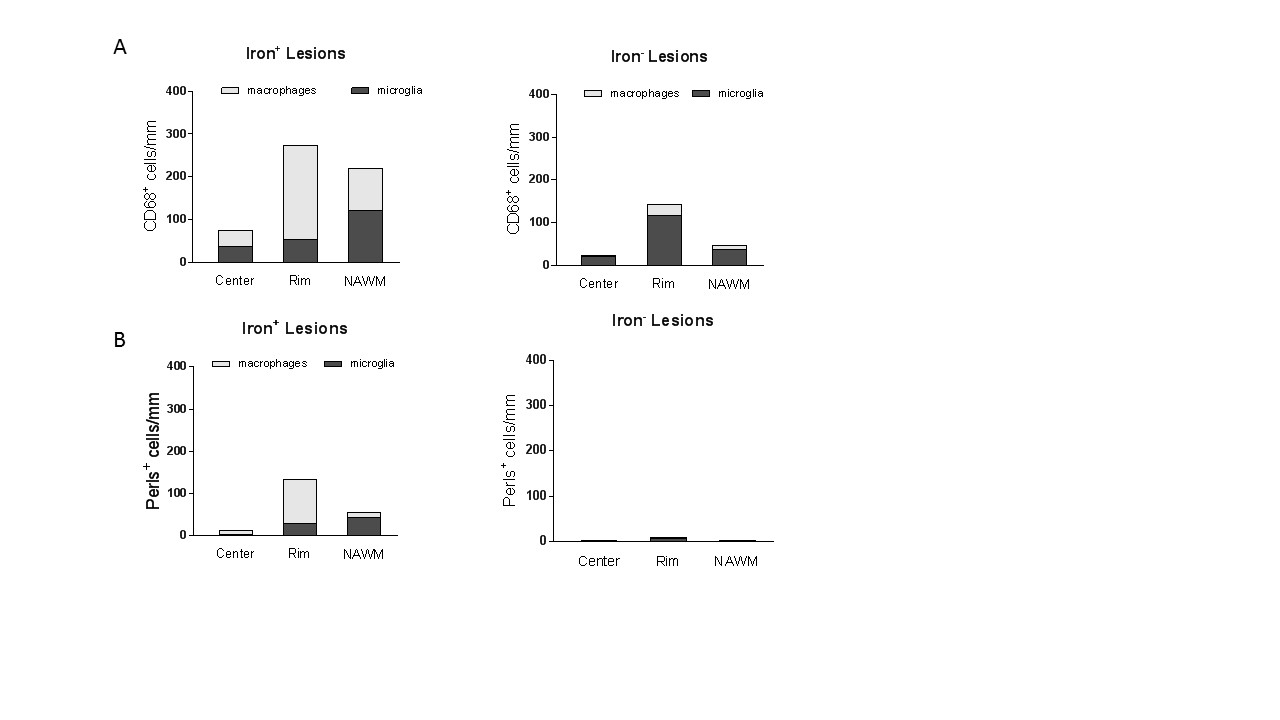
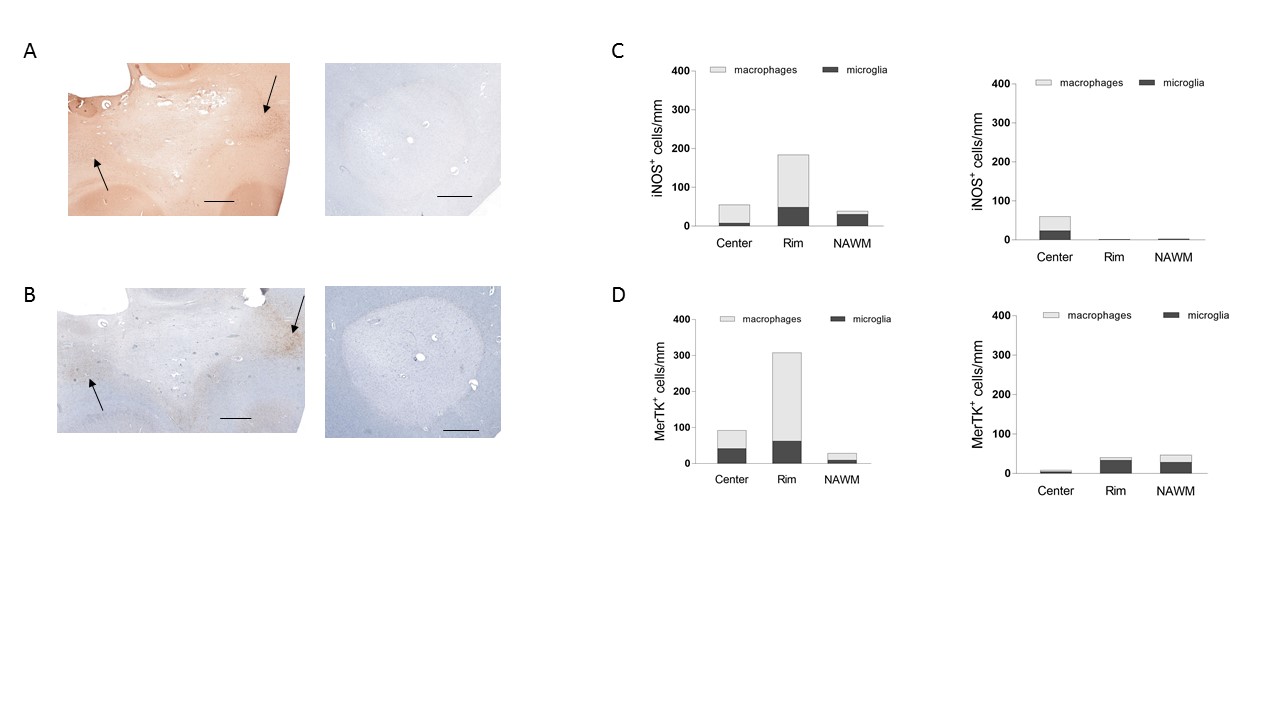
QSM identified lesions with high susceptibility rims; these areas contained iron-laden pro-inflammatory macrophages and microglia, as identified by staining techniques (Figure 1). Conversely, chronic active lesions that did not display high susceptibility rims on QSM were iron negative and contained significantly fewer activated macrophages and microglia in the lesion rim and surrounding white matter (Figures 2 & 3). While iron+ CD68+ cells expressed M1 markers such as iNOS and Ferritin and phagocytic markers such as MerTK (Figure 4), macrophages/microglia within iron- lesions expressed negligible levels of pro-inflammatory M1 markers and anti-inflammatory M2 markers (Figure 4).Discussion
Previous work has shown that MS lesion rims with macrophages/microglia contain iron, express CD86, and correspond to high susceptibility (3). By combining QSM with phenotypic markers and manual quantification, we demonstrate that lesions with high susceptibility rims correspond to regions of substantial pro-inflammatory inflammation that is likely to be of clinical relevance.Conclusion
Our results indicate that QSM can be used to detect chronic smoldering lesions behind an intact BBB. Identifying and tracking these lesions is of critical importance in the clinic, as the therapeutic goal in treating MS is to reduce the inflammatory response.Acknowledgements
This work is funded by grants from the NIH to D. Pitt and Y. Wang.References
1. Eskreis-Winkler S, Zhang Y, Zhang J, et al. The clinical utility of QSM: disease diagnosis, medical management, and surgical planning. NMR Biomed 2017;30(4).
2. Mehta V, Pei W, Yang G, et al. Iron is a sensitive biomarker for inflammation in multiple sclerosis lesions. PLoS One 2013;8(3):e57573.
3. Dal-Bianco A, Grabner G, Kronnerwetter C, et al. Slow expansion of multiple sclerosis iron rim lesions: pathology and 7 T magnetic resonance imaging. Acta Neuropathol 2017;133(1):25-42.
Figures