0076
Gadoxetate-enhanced abbreviated MRI is reliable and effective for HCC surveillance in high-risk patients.1Liver Imaging Group, University of California San Diego, San Diego, CA, United States, 2Radiology, University of California San Diego, San Diego, CA, United States, 3Gastroenterology and Hepatology, Virginia Mason Medical Center, Seattle, WA, United States, 4Hepatology, University of California San Diego, San Diego, CA, United States
Synopsis
Gadoxetate enhanced abbreviated MRI (AMRI) is a simple, rapid acquisition protocol aimed at reducing the cost and increasing the throughput of MRI-based HCC surveillance. Here we analyze 330 consecutive patients with cirrhosis or chronic HBV who underwent at least one screening AMRI. The rate of HCC detected at cross sectional analysis (3.3%) was in line with published incidence of HCC, while the technical failure rate was low (5.8%) despite high prevalence of cirrhosis and ascites. Longitudinal analysis demonstrated high sensitivity, specificity, and negative predictive value in HCC detection, using a composite reference standard.
Introduction
Imaging-based hepatocellular carcinoma (HCC) surveillance is known to improve survival in high -risk patients1. Despite higher sensitivity over other modalities2,3, MRI-based HCC surveillance is limited by concerns of cost and acquisition time. Previous work has demonstrated that a simplified gadoxetate-enhanced abbreviated MRI (AMRI) protocol including T1w hepatobiliary phase (HBP), T2w SSFSE, and diffusion weighted (DWI) imaging can detect HCC with high sensitivity and specificity when retrospectively simulated from complete scans4, but its performance in the clinical setting has been untested. In 2014 our institution began offering AMRI-based surveillance (total scanner time ≤ 15 minutes) for HCC in high-risk patients in which sonographic screening was compromised by obesity, hepatic steatosis, or severe parenchymal heterogeneity. Here we present cross-sectional and longitudinal analysis of the first three years utilizing this protocol on our clinical service.Methods
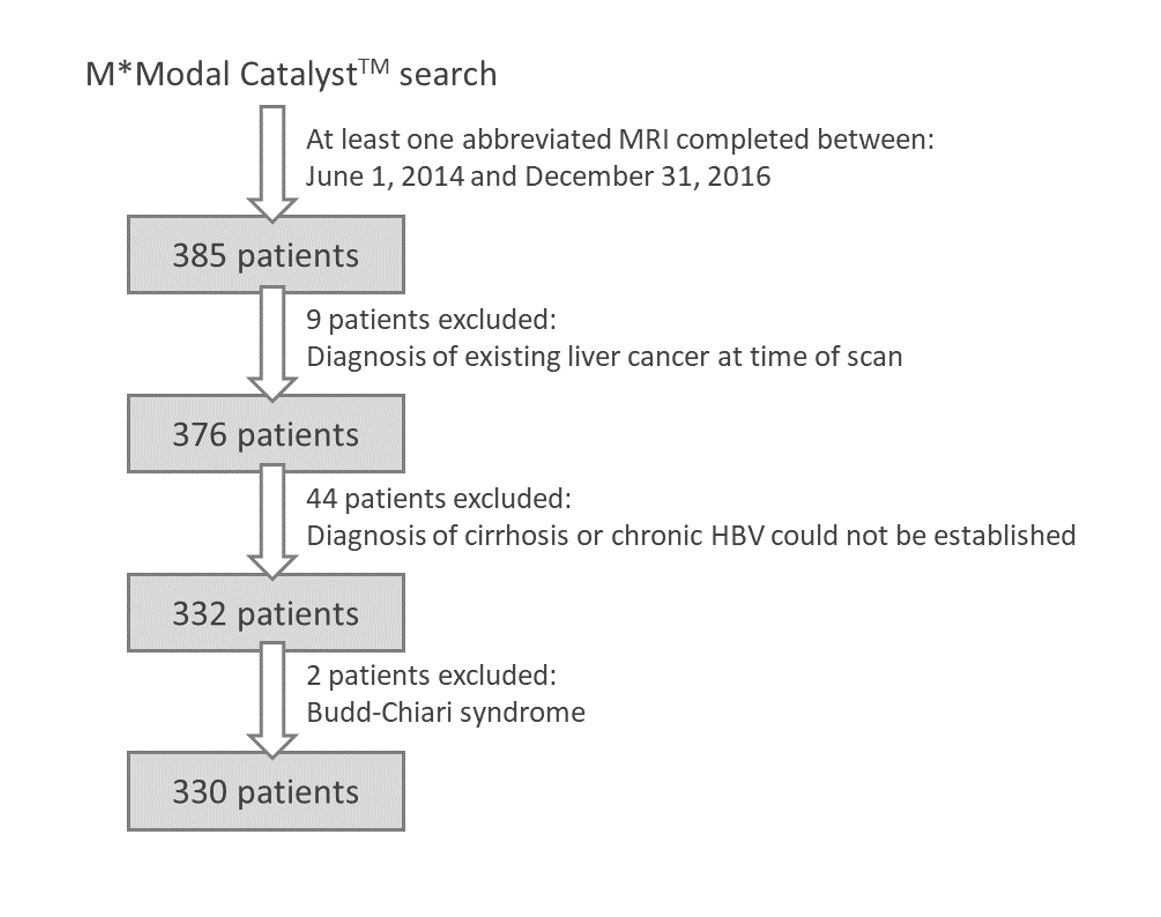
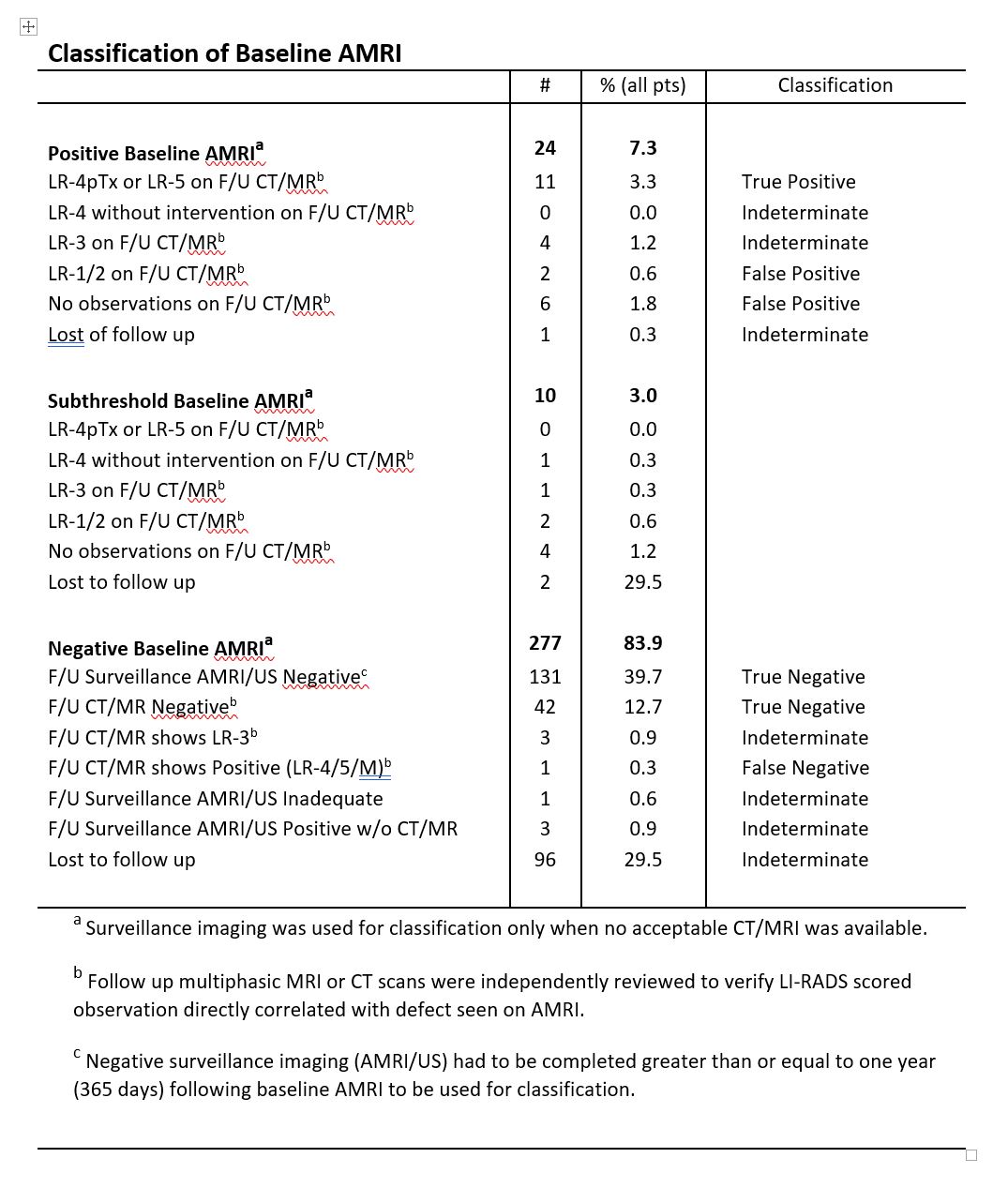
This is a single-center retrospective study with cross-sectional and longitudinal components. The study was HIPAA-compliant and approved by the institutional review board with an informed consent waiver. Consecutive patients meeting eligibility criteria were enrolled. Using a cloud-based search engine, we identified all patients aged 18 or greater with either cirrhosis or chronic HBV who underwent at least one AMRI for HCC screening from June 1, 2014 through December 31, 2016. For this cohort, all follow-up imaging through July 31, 2017 was reviewed. Contemporaneous laboratory data and any subsequent pathology results were extracted from the electronic medical record. Scans were acquired on 1.5T or 3T clinical scanners, read for clinical care by faculty abdominal radiologists, and reported using standard templates. Positive AMRIs triggered call-back multiphasic CT or MRI to characterize the AMRI-detected lesions; call-back exams were interpreted and reported using LI-RADS. A composite reference standard was applied based on all available follow-up exams and other diagnostic tests to classify patients as HCC-positive or -negative.Results
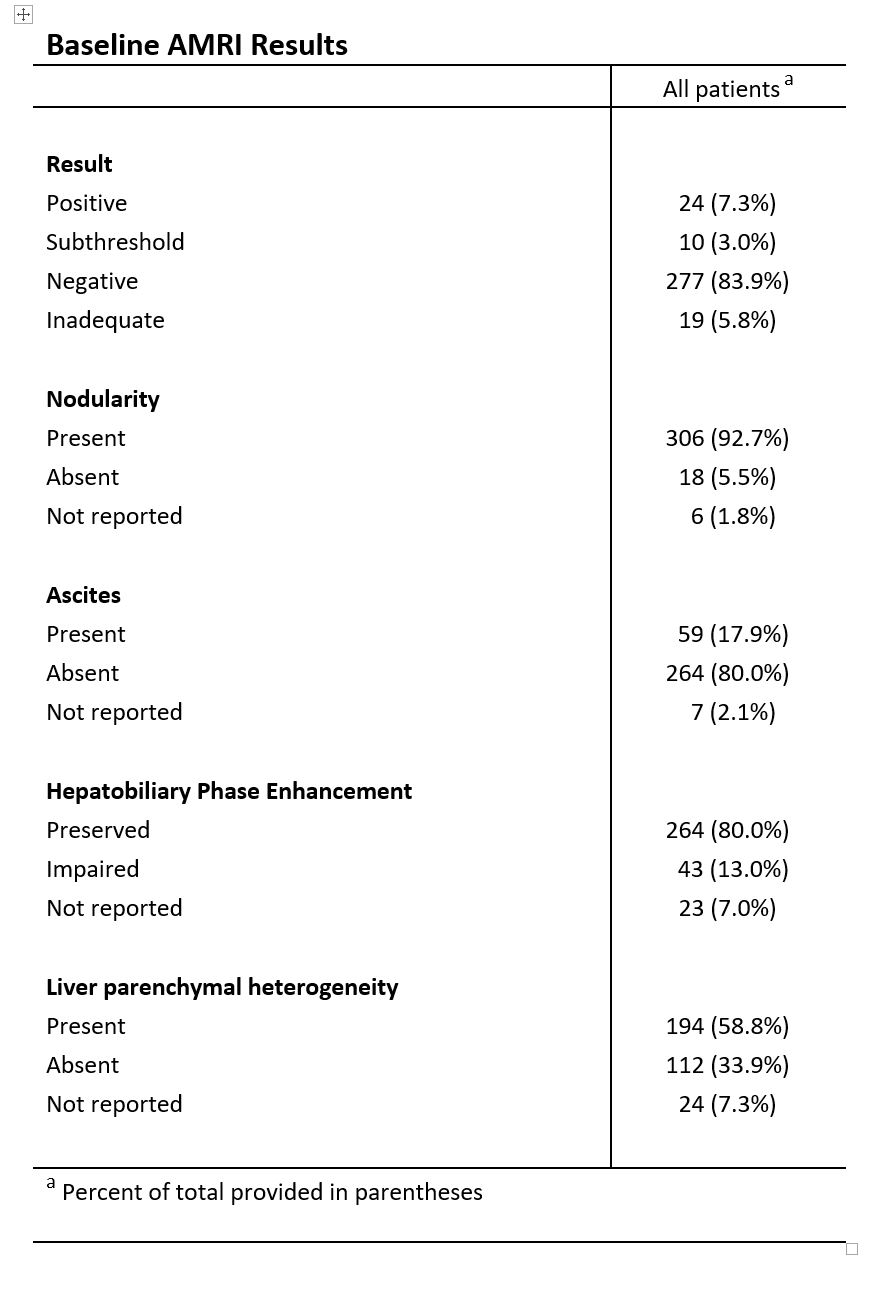
330 patients (93% with cirrhosis, 17% with ascites, 45% female, mean age 59 years) were included. Of 330 baseline AMRI, 24 (7.3%) were positive, including 11 true positives (defined as LI-RADS-5 or LI-RADS-4 treated as presumptive HCC after multidisciplinary discussion without biopsy) based on call-back multiphasic CT/MRI. Sensitivity was 0.92, specificity 0.96, positive predictive value (PPV) 0.58, and negative predictive value (NPV) 0.99. Conversely, 19 (5.8%) baseline AMRI were deemed inadequate, 15 due to heterogeneous or suboptimal liver enhancement, 3 due to motion artifact, 2 due to artifacts from large-volume ascites, and 1 unspecified (2 patients had multiple reasons given). Almost half (163/330) of patients underwent at least two AMRI. The average interval between scans ranging from 5.3 – 9.0 months. The percent positive dropped with each round of screening, reaching 2.3% (1/44) by the 4th AMRI.Discussion
AMRI is a rapid acquisition protocol (total scanner time ≤ 15 minutes) aimed at reducing the cost and increasing the throughput of MRI-based HCC surveillance. At our institution it is performed preferentially in cirrhotic patients with compromised sonographic screening. Positive baseline AMRI led to an HCC diagnosis in 3.3% of 330 consecutive high-risk patients, consistent with published HCC incidence in this population5. Longitudinal analysis demonstrated high sensitivity, specificity, and NPV. The frequency of inadequate exams was low (5.8%) despite the high prevalence of cirrhosis and ascites. The average surveillance interval for the 163 patient who underwent multiple AMRI was around 6 months, in line with current surveillance recommendations. The rate of positive studies declined with each round of imaging, possibly reflecting fewer false positives as experience accrued or differences in screening interval.Conclusion
Gadoxetate enhanced abbreviated MRI (AMRI) is a simple, rapid acquisition protocol aimed at reducing the cost and increasing the throughput of MRI-based HCC surveillance. Here we analyze 330 consecutive patients with cirrhosis or chronic HBV who underwent at least one screening AMRI. The rate of HCC detected at cross sectional analysis (3.3%) was in line with published incidence of HCC, while the technical failure rate was low (5.8%) despite high prevalence of cirrhosis and ascites. Longitudinal analysis demonstrated high sensitivity, specificity, and negative predictive value in HCC detection, using a composite reference standard.Acknowledgements
No acknowledgement found.References
1 Zhang, B. H., Yang, B. H. & Tang, Z. Y. Randomized controlled trial of screening for hepatocellular carcinoma. J Cancer Res Clin Oncol 130, 417-422, (2004).
2 Yu, N. C. et al. CT and MRI improve detection of hepatocellular carcinoma, compared with ultrasound alone, in patients with cirrhosis. Clin Gastroenterol Hepatol 9, 161-167, (2011).
3 Lee, Y. J. et al. Hepatocellular carcinoma: diagnostic performance of multidetector CT and MR imaging-a systematic review and meta-analysis. Radiology 275, 97-109, (2015).
4 Marks, R. M. et al. Diagnostic per-patient accuracy of an abbreviated hepatobiliary phase gadoxetic acid-enhanced MRI for hepatocellular carcinoma surveillance. AJR Am J Roentgenol 204, 527-535, (2015).
5 Fattovich, G., Stroffolini, T., Zagni, I. & Donato, F. Hepatocellular carcinoma in cirrhosis: incidence and risk factors. Gastroenterology 127, S35-50 (2004).
Figures