0073
Dynamic Gd-EOB-DTPA enhanced MR imaging of the liver: Value of High Temporal-resolution Images with Parallel imaging and Compressed Sensing1Radiology, Seirei Hamamatsu General Hospital, Hamamatsu, Japan, 2Global MR Applications and Workflow, GE Healthcare, Hino, Japan, 3Global MR Applications and Workflow, GE Healthcare, Madison, WI, United States, 4Global MR Applications and Workflow, GE Healthcare, Rochester, MN, United States
Synopsis
With ARC and CS, breath-hold dynamic Gd-EOB-DTPA enhanced MR imaging for the liver can be successfully performed with acceptable image quality and lesion recognitions on a clinical 3T magnet. High temporal resolution images with CS-LAVA for dynamic contrast MR study may give us benefits in comparison of Turbo-LAVA with lower temporal resolutions.
Introduction
Combination of parallel imaging (ARC) and compressed sensing (CS) can enhance speed of fast imaging. So far, with ARC and CS, temporal resolution for one phase covering the liver can be about five seconds in 3D T1WI of LAVA. Gd-EOB-DTPA is a liver specific contrast media, which is often used for evaluations of the liver. Dynamic contrast enhanced MR imaging should provide perfusion of hepatic tumor and much fast imaging will also provide selective vascular visualization1. The purpose was to asses values of fast MR imaging for dynamic Gd-EOB-DTPA enhanced MR imaging using turbo LAVA with ARC and CS in comparison with that using turbo LAVA with ARC only for the evaluation of the liver.Materials and Methods
The study was approved by the institutional review board and informed consent was obtained from the patients. Patients population: Thirty patients (19 men, 11 women, mean 65 years old) were selected, who underwent dynamic Gd-contrast (Gd-EOB-DTPA) enhanced MR imaging of the liver using turbo LAVA using spec IR for fat saturation with ARC and CS (CS-LAVA) at 3T (Discovery 750, GEHC), and who had undergone prior dynamic contrast study with double arterial phases using turbo LAVA-Flex (Turbo-LAVA) at 3T within one year. Pathologies were as follows; CS LAVA group: HCC 4 cases, AP/AV shunts 7, post radiofrequency ablation (RFA) 8, Hemangioma 2, turbo LAVA group: HCC 8 cases, AP/AV shunts 6, post radiofrequency ablation (RFA) 10, Hemangioma with shunts 2. MR imaging: The current dynamic contrast imaging was obtained using Turbo-LAVA with ARC and CS (one phase; 4-5seconds Gd-EOB-DTPA 0.1mL/kg, injection rate 1mL/sec) was performed using smart prep technique for triggering initial imaging. Consecutive five phases within a breath-hold were obtained. Portal, equilibrium and hepatobiliary phase was obtained, respectively. The prior dynamic contrast enhanced MR study using Turbo-LAVA Flex with ARC (one phase; 11seconds, Gd-EOB-DTPA 0.1mL/kg, injection rate 1mL/sec) had been performed with the same conditions except acquisitions of consecutive two phases in a breath-hold were obtained as in the arterial phases followed by portal, equilibrium and hepatobiliary (HB) phases, respectively. Evaluations: Image quality and recognitions of hepatic arteries, portal veins and hepatic veins were evaluated using a five-point scale (1 undiagnostic-5 excellent) in the current and former study, respectively. Selective recognition of enhanced vasculature and pancreas was evaluated, respectively. “A” indicates that in the hepatic artery was only enhanced. Both the hepatic artery and branches of the portal artery were enhanced in the liver, but signal to noise (SNR) was higher in the hepatic artery “A>P”, or the branches of the portal vein (A<P), or equally enhanced (A=P). “V=” indicates the hepatic vein and the hepatic parenchyma were equally enhanced. “V+” indicates that the hepatic vein was enhanced stronger than the hepatic parenchyma. “Panc” indicated that the peak enhancement of the pancreatic parenchyma was observed. Lesions as hypervascular lesions including HCC, and vascular shunts were also evaluated. Enhanced hepatic lesions were regarded as HCC when the corresponding lesions were recognized as low signal intensity lesions on a HB phase. Vascular shunts were recognized as hypervascular areas, which were not recognized on HV phase. Confident of lesion recognitions was evaluated using a five point scale (5 definitely exist-1 definitely no lesions). Scores for five and four were regarded as positive lesions.Results
All
images in dynamic contrast phases were diagnostic in CS LAVA and Turbo LAVA
groups, respectively (Fig 1). Time for image reconstruction was about 5 minutes
for each phase. Artery only and arterial dominant enhancement was recognized in
the first and second phase of CS-ALVA group (Table, Figures 2, 3). HCC,
and AP shunts were successfully diagnosed in the CS-LAVA with higher
confidence than in Turbo-LAVA because in the 1st phase, lesions or
shunts and arteries were solely recognized as enhanced regions (Fig 3, 4, Table). For
the detection of HCC, among 26 HCCs of CS-LAVA group, 23 lesions were detected as
a true positive (Score 4:5=7cases:16cases)(88.5%) and among 17 HCCs of Turbo-LAVA
group, 14 lesions were detected as a true positive lesion (Score4:5=6cases:8cases)
(82.3%).Discussion
Dynamic contrast MR imaging could be successfully obtained with acceptable image quality and lesion recognitions with CS and ARC. High temporal resolution (4-5 seconds for one phase); images reconstructed from independent data sets (without view share); optimal timing for start of 1st phase with monitoring contrast-arrival.
Conclusion
With ARC and CS, breath-hold dynamic Gd-EOB-DTPA enhanced MR imaging for the liver can be successfully performed on a clinical 3T magnet. High temporal resolution images with CS-LAVA for dynamic contrast MR study may give us benefits in comparison of Turbo-LAVA with lower temporal resolutions.Acknowledgements
No acknowledgement found.References
No reference found.Figures
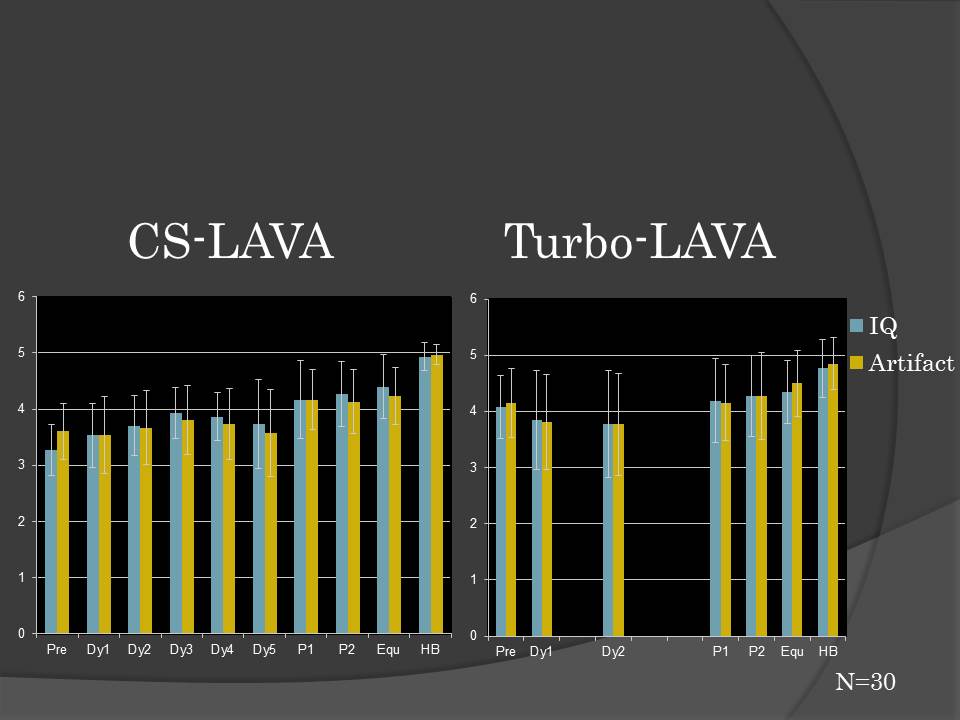
Fig. 1 Scores for Image quality & Artifact
Image quality of precontrst and 1st phase images with CS-LAVA was relatively low. Image quality of 2nd and later phase images were better. Image quality of all phases with Turbo-LAVA was stable.
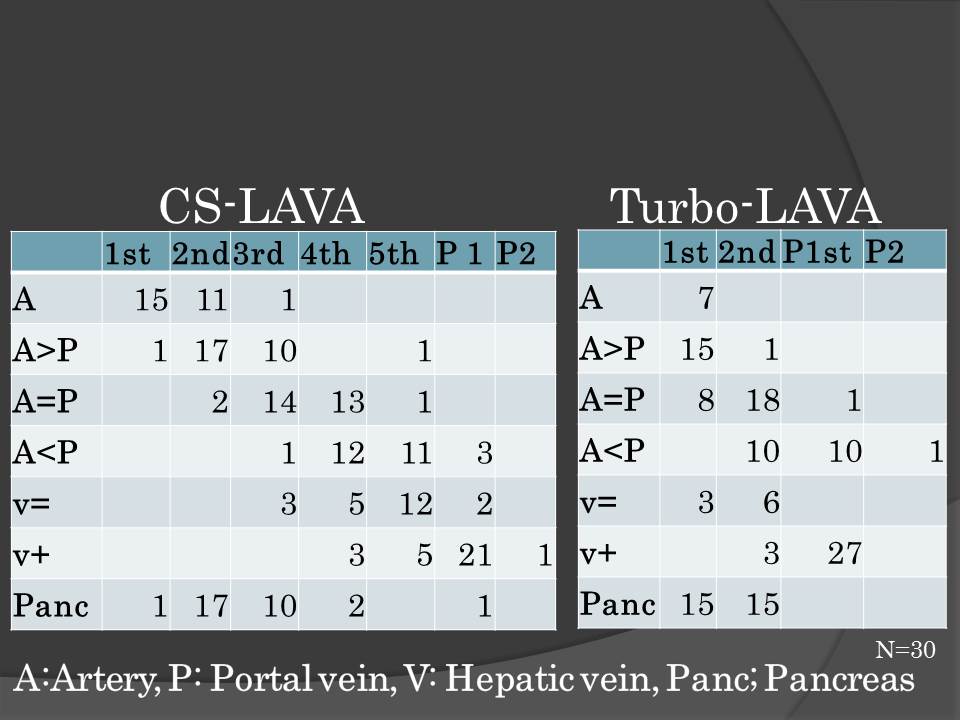
Table Selective enhancement of the hepatic vasculatures and pancreas.
With CS-LAVA in 27 patients, arteries were solely visualized in the early phases although with Turbo LAVA in only 8 patients, arteries were solely viualized.
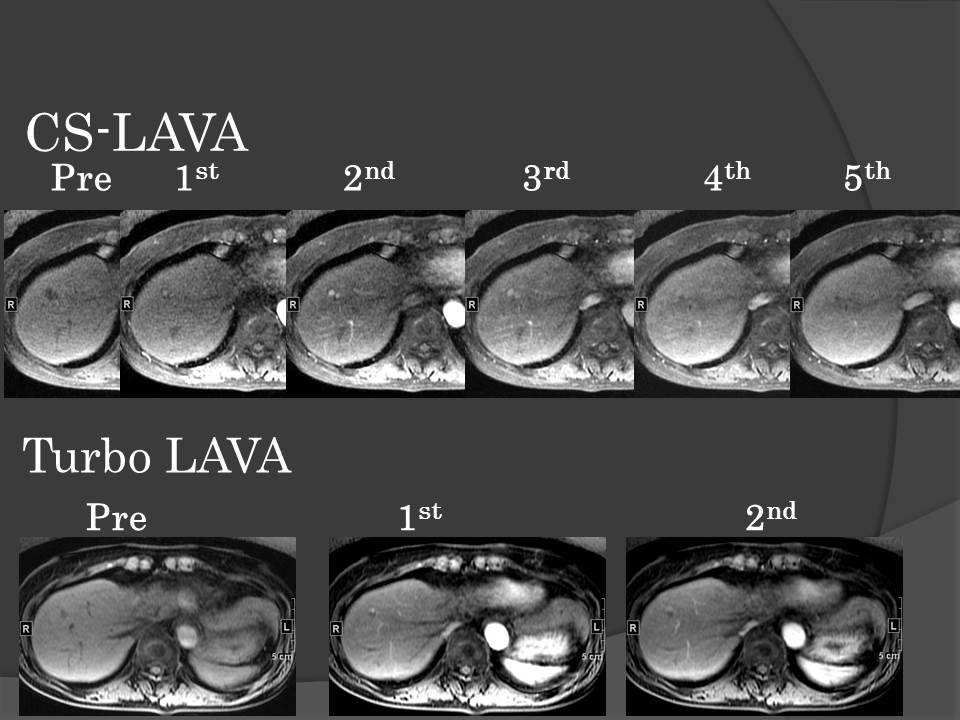
Fig. 3 Liver cirrhosis and HCC
In the right lobe of the liver, a recurrent hypervasuclar lesion after TACE is noted in CS-LAVA with high confidence because of no overlap of the hepatic vasulatures and lesions. In Turbo-LAVA, a hypervascular tumor in the right lobe is noted as HCC, but on 1st phase images, both lesion and hepatic vasculatures were enhanced. This lesion was treated with TACE.
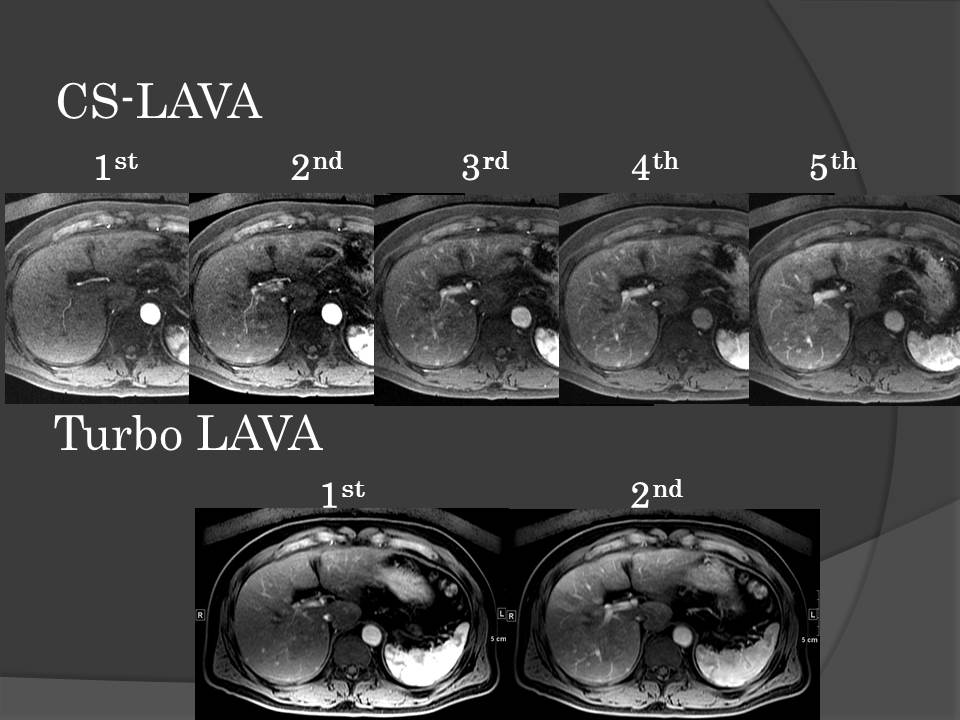
Fig. 4 Liver cirrhosis and arterial portal shunts
Hypervasuclar lesions are noted in the liver on both CS-LAVA and Turbo-LAVA images. Confidence for the detection of shunts is much higher on CS-LAVA than Turbo-LAVA because CS-LAVA demonstrated solely shunts and hepatic arteries without overlap of other vasculatures.