0072
View-Sharing Artifact Reduction with Retrospective Compressed Sensing Reconstruction in the Context of Contrast-Enhanced Liver MRI for Hepatocellular Carcinoma (HCC) Screening1Radiology, Stanford University, Stanford, CA, United States, 2Electrical Engineering and Radiology, Stanford University, Stanford, CA, United States, 3Radiology, Veteran Affairs Palo Alto Health Care System, Palo Alto, CA, United States
Synopsis
View-sharing (VS) increases spatiotemporal resolution in dynamic contrast-enhanced (DCE) MRI by temporally sharing high frequency k-space data across contrast phases. However, this temporal sharing results in respiratory motion occurring in any single phase to propagate artifacts across all phases. Compressed sensing (CS) can eliminate need for VS by recovering missing k-space data from pseudorandom under-sampling, reducing temporal blurring while maintaining spatial resolution. We tested CS versus VS in the setting of DCE MRI for HCC. CS reduced respiratory artifacts, produced images with a more synthetic appearance, and did not result in a difference in lesion detection.
Introduction
Hepatocellular carcinoma (HCC) screening is a common indication for contrast-enhanced liver MRI. However, MRI in the abdomen is often degraded by respiratory motion artifacts arising from incomplete suspension of respiration. These artifacts create difficulties in interpretation and can undermine the sensitivity of MRI, which is otherwise the best detection method for HCC.1
Diagnostic criteria for HCC are defined by Organ Procurement and Transplantation Network/United Network for Organ Sharing (OPTN/UNOS) and used extensively in radiologic reporting at transplant centers.2 As outlined by OPTN/UNOS, the crux of HCC diagnosis by MRI is high-quality DCE T1-weighted imaging including acquisition of the hepatic arterial phase.
To best image the optimal hepatic arterial phase, multiple early phases of contrast enhancement are acquired after contrast injection. However, maximizing temporal resolution is a competing goal with spatial resolution. View-sharing (VS) improves temporal resolution through rapid and frequent acquisition of central k-space data and an interleaved acquisition of segmented outer k-space data.3 Outer k-space data is then shared between temporal phases allowing preservation of spatial resolution at a cost of temporal blurring. This temporal sharing also propagates any motion occurring in a single contrast phase across all other VS phases. If the VS acquisition is arranged so the segmented outer k-space data is pseudo-randomly sampled, the acquired k-space data can alternatively be reconstructed using locally low rank compressed sensing (CS) methods exploiting inherent spatiotemporal sparsity of DCE images without resorting to VS. This CS reconstruction provides a shorter “temporal footprint” for the same acquired data, while leaving the VS reconstruction essentially unchanged.4,5
We hypothesized that a CS reconstruction of reduced VS data would be superior to VS in image quality, anatomic delineation, and overall detection of HCC. We have previously reported a similar such comparison6, and now extend those results using a further optimized CS reconstruction and a larger number of patients.
Methods
This was an IRB-approved, HIPAA-compliant retrospective study of DCE comparing VS to CS in patients who received MRI for HCC screening. Compared to our prior study, the CS reconstruction was further optimized by reducing the regularization parameter to improve synthetic appearance.
Two radiologists (SC and AR, 3 and 1 years of experience interpreting body MR, respectively) independently assessed VS and CS images for image quality (1-4; inferior-superior) and anatomic delineation (1-5; inferior-superior). Of the final cohort, a select group of patients with known HCC were subselected and in a separate assessment, OPTN criteria were used for lesions suspected to represent HCC. Diagnostic confidence in lesion detection was also assessed (1-5; low-high). Subsequently, side-by-side blinded evaluations were performed (-3 to 3; 0 implying equivalence).
Intraclass correlation coefficients were used to evaluate inter-reader agreement. Wilcoxon rank tests were performed for paired, nonparametric analyses with Bonferroni-Holm correction for multiple comparisons. McNemar’s test assessed for differences in frequency of lesion detection.
Results
The final cohort of 50 patients had an average age of 62 ± 10 years, with 29 males.
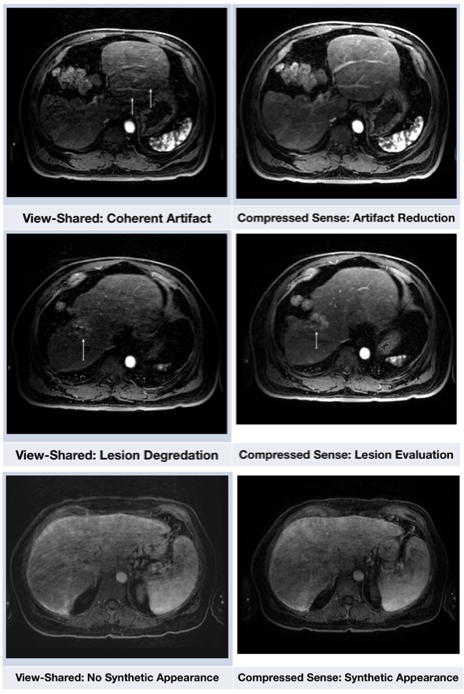
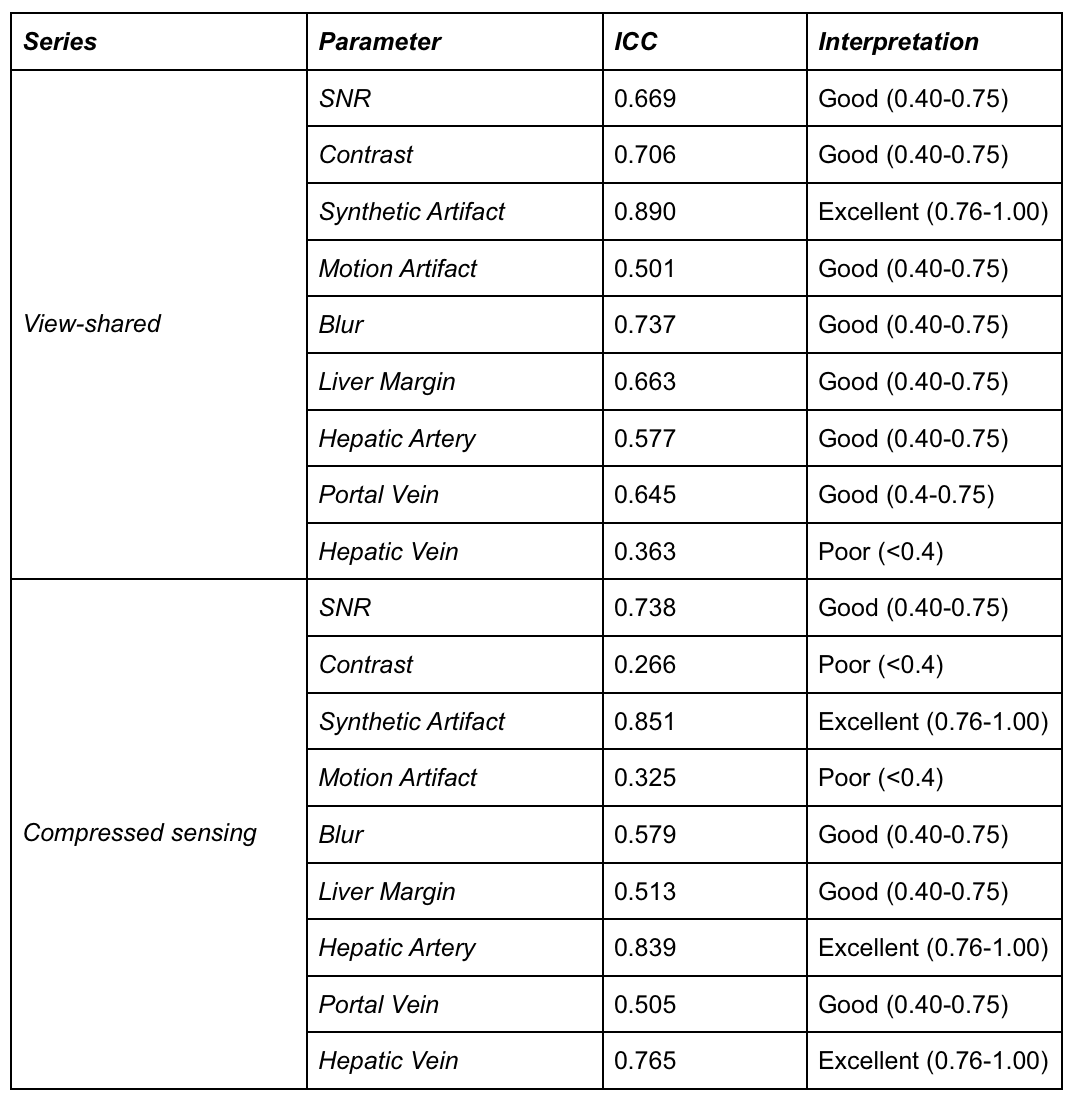
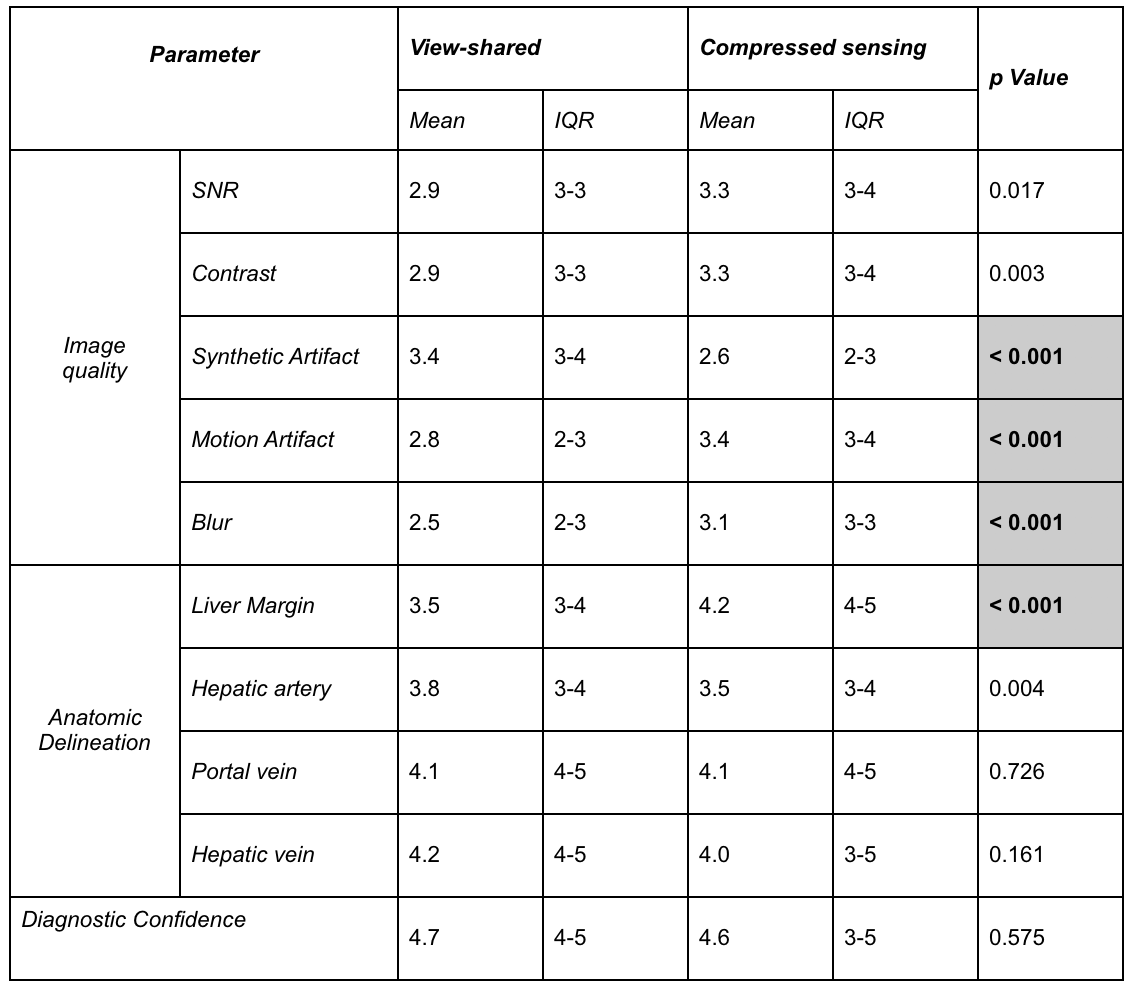
Inter-reader agreement was more substantial for general image quality than anatomic delineation (Table 1). CS demonstrated significantly less motion artifact and blurring than VS (Table 2; Figure 1). A synthetic appearance on CS was judged to be present, an expected finding using an iterative reconstruction. (Figure 2).
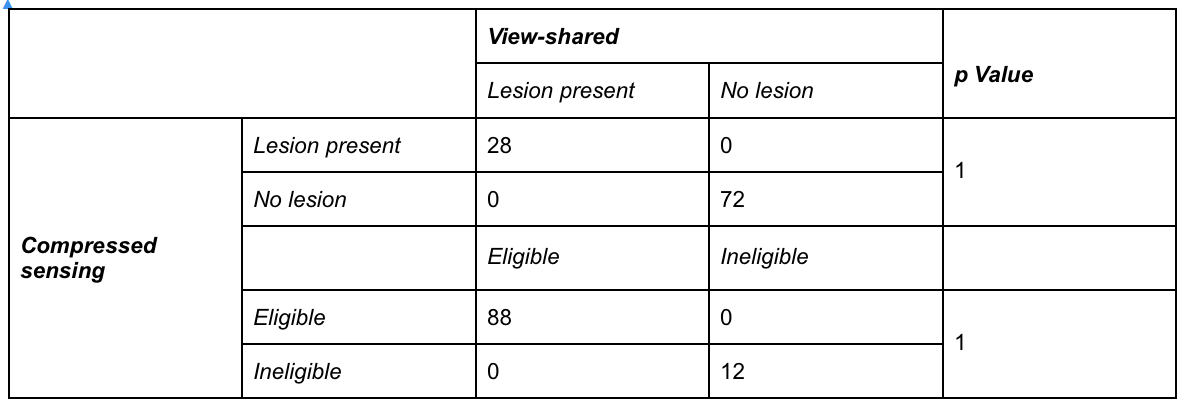
With respect to perceived diagnostic confidence in interpretation, no significant difference was noted between VS and CS. More importantly, frequency of lesion detection didn't differ by technique; every case of HCC on VS was detected on CS. This implies comparability of CS to VS for the most vital aspect of the exam: detection of HCC (Table 3). Similarly, no change in eligibility for transplantation would have occurred using CS (Table 3).
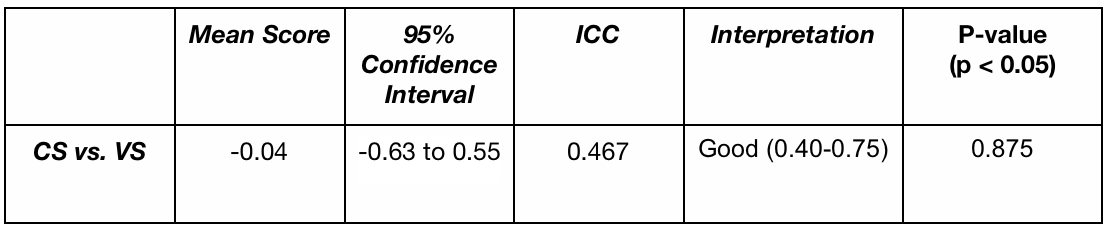
Side-by-side evaluations revealed a slight preference for CS over VS (Table 4), however this was not statistically significant (p < 0.05).
Discussion
CS significantly reduced motion artifacts, and readers aesthetically preferred CS over VS. One often cited imperfection of iterative reconstructions is a resultant synthetic (“cartoon-like”) appearance. However, this is not unanimously viewed as undesirable, especially among newly-trained radiologists who have greater exposure to iterative reconstructions in the context of computed and emission tomography. We demonstrated decreased motion artifact and blurring for CS compared to VS, and similar reliability in detection of HCC. No change in eligibility or prioritization for transplantation would have occurred through use of CS in our patients.
Conclusion
Applying a CS reconstruction to data acquired for a VS reconstruction can add robustness to motion artifacts in a clinical DCE protocol. Application of this technique beyond HCC can firmly establish its clinical benefit.Acknowledgements
This work was in part supported by NIH grant P41 EB015891 and R01 EB009055. The authors would also like to thank the support of GE Healthcare.References
1. Pitton MB, Kloeckner R, Herber S, Otto G, Kreitner KF, Dueber C. MRI versus 64-row MDCT for diagnosis of hepatocellular carcinoma. World J Gastroenterol. 2009;15:6044-6051.
2. Rosenkrantz AB, Campbell N, Wehrli N, Triolo MJ, Kim S. New OPTN/UNOS classification system for nodules in cirrhotic livers detected with MR imaging: effect on hepatocellular carcinoma detection and transplantation allocation. Radiology. 2015; 274:426-433.
3. Saranathan M, Rettmann DW, Hargreaves BA, Clarke SE, Vasanawala SS. Differential subsampling with Cartesian ordering (DISCO): a high spatio-temporal resolution Dixon imaging sequence for multiphasic contrast enhanced abdominal imaging. J Magn Reson Imaging. 2012; 35:1484-1492.
4. Liang ZP. Spatiotemporal imaging with partially separable functions. IEEE International Symposium on Biomedical Imaging: From Nano to Macro. 4th IEEE; 2007.
5. Levine E, Daniel B, Vasanawala SS, Hargreaves B, Saranathan M. 3D Cartesian MRI with compressed sensing and variable view sharing using complementary Poisson-disc sampling. Magn Reson Med. 21 April 2016.
6. Hepatocellular carcinoma (HCC) screening with contrast-enhanced liver MRI: View-sharing artifact reduction with retrospective compressed sensing reconstruction (ISMRM Abstract Submission 2017)
Figures