0021
First clinical pilot study using screen-printed flexible MRI receive coils for pediatric applications1Department of Radiology, Stanford University, Stanford, CA, United States, 2University of California Berkeley, Berkeley, CA, United States, 3Lucile Packard Children's Hospital Stanford, Stanford, CA, United States, 4GE Healthcare, Aurora, OH, United States, 5Department of Electrical Engineering, Stanford University, Stanford, CA, United States
Synopsis
Pediatric MRI is often performed suboptimally by the use of heavy, large, and relatively inflexible coil arrays that are designed and built for adult MR imaging. For the child, these arrays can be intimidating and uncomfortable, restricting breathing. For parents, they contribute to the stress of the exam. For pediatric caregivers for smaller children, the coils complicate placing medical support equipment. Here, we assess the use of screen printed flexible coil arrays for pediatric applications, focusing on clinical image quality and caregiver acceptance. We conclude that a flexible screen-printed MRI receive coil is likely to yield diagnostic image quality and be preferred to a traditional coil by patients, parents, and caregivers.
Purpose
To assess the clinical performance and acceptance of small-sized screen printed flexible coil arrays in pediatric MRI.Introduction
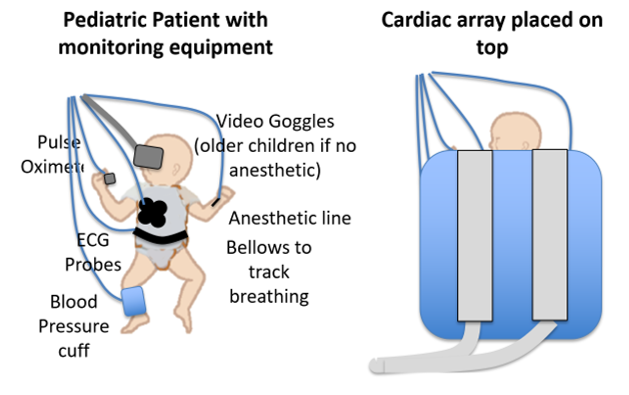
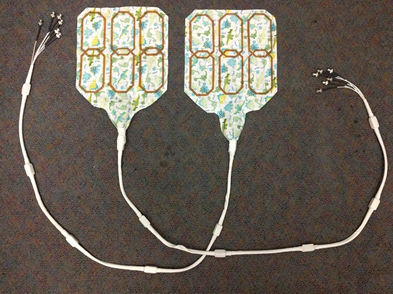
Pediatric MRI is often performed suboptimally by the use of heavy, large, and relatively inflexible coil arrays that are designed and built for adult MR imaging. For the child, these arrays can be intimidating and uncomfortable, restricting breathing. For parents, they contribute to the stress of the exam. For pediatric caregivers for smaller children, the coils complicate placing medical support equipment, such as mechanical ventilation tubes, pulse oximeters, anesthetic lines, respiratory bellows, blood pressure cuffs, ECG probes, and video goggles (Fig. 1). For sedated/anesthetized children, the respiratory compromise often requires more invasive respiratory support. Here, we assess the use of screen printed flexible coil arrays [1-3] (Fig. 2,3) for pediatric applications, focusing on clinical image quality and caregiver acceptance.Methods
With IRB approval and informed consent/assent, 20 patients were recruited. They were scanned with a 12-channel screen printed coil on a GE 3T MR750 scanner using standard clinical protocols. For each subject, MR technologists, nurses, anesthesiologists, and the children/parents involved in each exam were surveyed to assess the level of acceptance of printed coils.
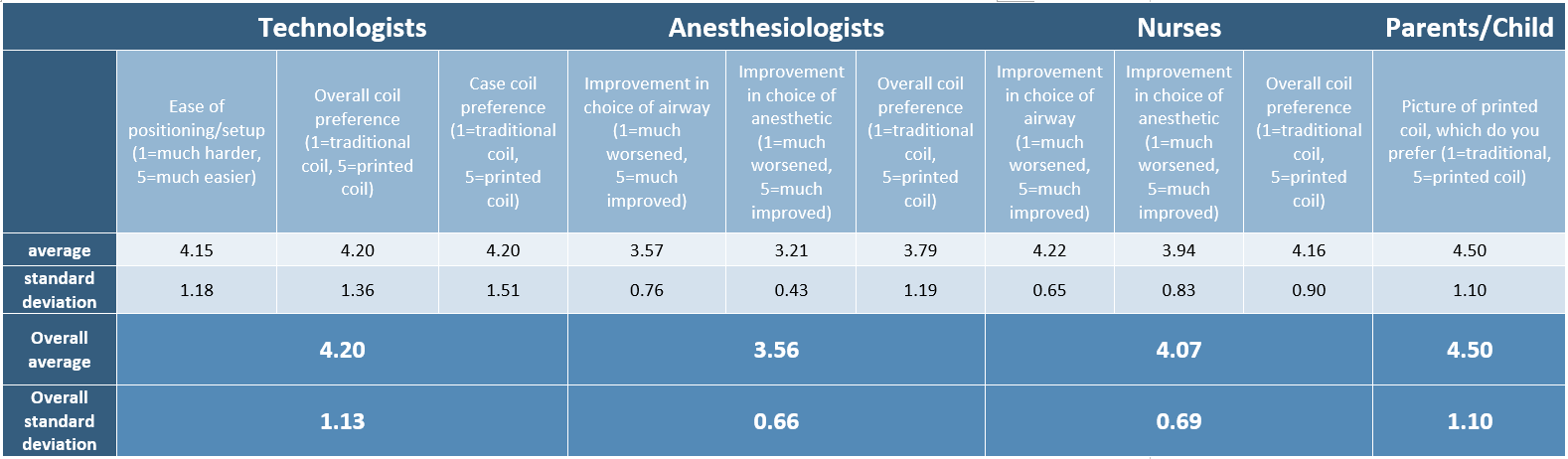
Technologists recorded the (1) ease of positioning, (2) coil preference for the specific exam, and (3) overall coil preference. Anesthesiologists were queried on (1) choice of airway, (2) choice of anesthetic, and (3) overall coil preference. Patients and/or their parents recorded their overall coil preference. Each preference was recorded on a rating on a scale from 1 (traditional coil) to 5 (printed coil). Additionally, open-ended feedback was recorded.
To compare imaging performance, signal-to-noise ratio (SNR) was evaluated in muscle tissue on an axial T2 image with parameters (TE=80, no acceleration, non-fat-saturated, FOV=24cm, voxel size=0.75mm x 0.75mm x 5mm, scan time ~90s depending on respiratory triggering). SNR for age-matched cases imaged with a product GE 32 channel cardiac array coil was similarly calculated, and normalized to the 0.75mm x 0.75mm x 5mm voxel size for this relative comparison wherever a varied FOV was necessary.
Results
Patient ages were 2 days to 12 years, weight 1.8 kg to 57 kg and imaged body parts were abdominal/pelvic (9 patients), MRCP (3 patients), cardiac (3 patients), chest (3 patients), and upper extremities exams (2 patients). 10 patients were scanned with ferumoxytol, 9 patients with gadobutrol, and one with no intravenous contrast agent. 14 patients received anesthesia.
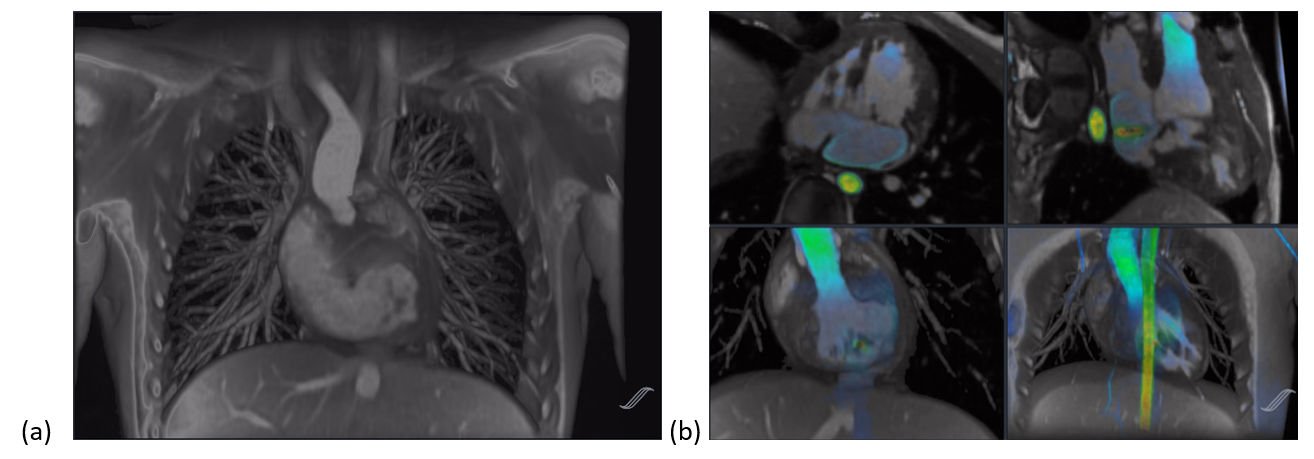
Representative results are shown in Fig. 4. In the patient/provider survey we obtained an overall score of 4.08 ± 0.62 (1=traditional coil, 5=screen-printed coil), favoring the screen-printed coil. Averaging the ratings for all the preferences, technologists, anesthesiologists, nurses, and parents/children gave ratings of 4.20 ± 1.13, 3.56 ± 0.66, 4.07 ± 0.69, 4.50 ± 1.10, respectively (more detailed responses shown in Fig. 5). Together, this yielded an overall score of 4.08 ± 0.62. Each case was judged to have good diagnostic quality by two experienced radiologists. The normalized SNR was measured to 53.8 ± 49.3 for the screen-printed coil, as compared to 43.8 ± 13.6 for the product coil. A more complete analysis comparing screen-printed and product coils is available in the original design work [1,2].
Discussion
Areas noted for improvement included potential padding of the cord to prevent discomfort in chest imaging and stiffening support that was required to activate respiratory monitoring in a few isolated cases. The latter could be easily remedied by integrating an air pad into the coil.Conclusion
A flexible screen-printed MRI receive coil is likely to yield diagnostic image quality and be preferred to a traditional coil by patients, parents, and caregivers.Acknowledgements
The authors gratefully acknowledge support through NIH K99 EB24341 and NIH R01 EB019241.References
[1] Corea JR, Flynn AM, Lechene B, Scott G, Reed GD, Shin PJ, Lustig M, Arias AC. Screen-printed flexible MRI receive coils. Nat Commun. 2016;7:10839. [2] Corea JR, Lechene PB, Lustig M, Arias AC. Materials and methods for higher performance screen-printed flexible MRI receive coils. Magn Reson Med. 2017;78(2):775-783. [3] Corea J, Lechene BP, Grafendorfer T, Robb, F, Arias AC, Lustig M. Printed receive coil arrays with high SNR. Proc Int Symp Magn Res Med. 2016;24:2146.Figures