0005
Postoperative changes in volume flow rate in the thoracic aorta and the aortic arch branches in patients with aortic valve stenosis: a prospective serial 4D flow MRI studyHiroki Kamada1, Hideki Ota1, Masanori Nakamura2, Yohsuke Imai3, Wenyu Sun1, Yoshiaki Komori4, Ko Sakatsume5, Ichiro Yoshioka5, Yoshikatsu Saiki6, and Kei Takase1
1Department of Diagnostic Radiology, Tohoku University Hospital, Sendai, Japan, 2Department of Electrical and Mechanical Engineering, Nagoya Institute of technology, Nagoya, Japan, 3School of Engineering, Tohoku University, Sendai, Japan, 4Siemens Japan K.K., Tokyo, Japan, 5Division of Cardiovascular Surgery, Tohoku University Hospital, Sendai, Japan, 6Division of Cardiovascular Surgery, Tohoku University Graduate School of Medicine, Sendai, Japan
Synopsis
Postoperative hemodynamic changes in the aorta in patients with aortic valve stenosis (AS) remain unclear. Four-dimensional (4D) flow MRI was perfumed in 11 AS patients before and after aortic valve replacement (AVR). We evaluated volume flow rate and the main flow direction, setting 15 planes of the aorta and 3 planes of the arch branches. Volume flow rate significantly increased in the ascending aorta and the arch branches. The main flow direction came to match with the axial direction of the aorta. These results suggest that AVR results in more efficient blood transport to the upper body including the brain.
Introduction
Aortic valve stenosis (AS) is known to be associated with cerebral ischemia due to decreased blood flow from the aortic arch. However, postoperative changes in the aortic blood flow in patients with AS remain unclear. Transthoracic echocardiography is a common clinical tool for the assessment of AS, but it has a limited window to visualize the blood flow in the aortic arch and its branches supplying blood to the brain. Four-dimensional (4D) flow MRI has been developed to evaluate the blood flow through the heart and the large vessels 1,2. The purpose of this study is to investigate hemodynamic changes in the thoracic aorta and branches of the arch before and after aortic valve replacement (AVR) in AS patients using 4D flow MRI.Methods
In this institutional-review-board approved prospective study, we enrolled 11 AS patients (6 men, 5 women; mean age 76 years, range 70-84 years). Thoracic 4D flow MRI using a 3.0T scanner was performed in patients before and after AVR (mean interval, 27±5.5 days). 4D flow MRI was acquired using the following parameters: 3-dimensional phase-contrast MR imaging with 3-directional velocity encoding in transverse acquisition; ECG-gating; respiratory-gating; TR/TE, 42.6/2.54 ms; flip angle, 15 degrees; VENC, 160-360 cm/sec; spatial resolution, 2.5x1.8x2.5 mm3; time resolution 14-24 phase/beat. Fifteen planes in the aorta (ascending aorta, 4, arch, 5, descending aorta 6) and 3 planes in the aortic arch branches (1 per each branch) were set to evaluate 1) volume flow rate in each plane during a cardiac cycle and 2) the angle between the main flow direction in a specified plane and the axial direction of the aorta during the systole phase, as shown in Fig. 1.Results
A significant increase in volume flow rate after AVR was found in the ascending aorta (pre-AVR, 59.7±27.2 mL/cycle vs. post-AVR 76.3±19.5 mL/cycle, p=0.0024) and the aortic arch branches (pre-AVR, 23.4±8.6 mL/cycle vs. post-AVR 36.0±1.4 mL/cycle, p=0.002), whereas no significant change was observed in the descending aorta (pre-AVR, 59.9±14.5 mL/cycle vs. post-AVR, 59.1±12.8 mL/cycle, p=0.5), as shown in Fig. 2A. Postoperative ratios of volume flow rate were 1.45±0.54 in the ascending aorta, 1.57±0.28 in the branches and 1.00±0.15 in the descending aorta, respectively. Among the aortic arch branches, the ratios were 1.53±0.39 in the brachiocephalic, 1.38±0.55 in the left common carotid, and 1.81±0.83 in the left subclavian arteries, respectively. The flow angle significantly decreased in the ascending aorta (before 35.3±13.6 degree vs. after 23.9±9.3 degree, p<.0001) and the aortic arch (pre-AVR, 16.8±10.2 degree vs. post-AVR, 13.3±6.5 degree, p=0.006), as shown in Fig. 2B . However, no significant change in the angle was found in the descending aorta (pre-AVR 10.8±5.7 degree vs. post-AVR 11.2±5.5 degree, p=0.652).Discussion
The main flow direction became near the axis of the ascending and the aortic arch and the volume flow rate was significantly increased in the ascending aorta and the aortic arch branches after AVR. To study postoperative hemodynamic changes, we plotted the streamline and helicity in patients where the volume flow rate in the ascending aorta and the aortic arch branches were remarkably increased. The streamline plots show jet and swirling flow in the aortic root, and secondary flow in the ascending aorta and aortic arch before AVR, as shown in Fig. 3A. After AVR, jet flow disappeared and streamline plots distributed along with greater curvature of the ascending aorta and the aortic arch as shown in Fig. 3B. The isosurface plot of helicity density in systole is shown in Fig. 4. The helicity density is decreased in the arch aorta after AVR as shown in Fig. 4B. Here, helicity density is defined as scalar product between flow velocity and vorticity. Thus, the decrease in helicity density proximal to the aortic arch branches indicates decrease in secondary flow after AVR. The observations of streamline and helicity plots suggest that AVR results in the improvement of flow direction as well as decrease in secondary flow in the ascending and the aortic arch, which would contribute to increase in volume flow rate in the ascending aorta and the aortic arch branches.Conclusion
After AVR, blood flow in the ascending and the aortic arch as well as the aortic arch branches increased within 1 month, showing more blood supply to the upper body including the brain. In addition, the direction along the main flow from the ascending and the arch aorta came to match with the axial direction of the aorta after AVR, thereby achieving more efficient blood transport.Acknowledgements
No acknowledgement found.References
- Uribe S, Beerbaum P, Sorensen TS, et al. Four-dimensional (4D) flow of the whole heart and great vessels using real-time respiratory self-gating. Magn Reson Med. 2009;62:984–92.
- Nordmeyer S, Riesenkampff E, Messroghli D, et al. Four-dimensional velocity-encoded magnetic resonance imaging improves blood flow quantification in patients with complex accelerated flow. J Magn Reson Imaging. 2013;37:208–16.
Figures
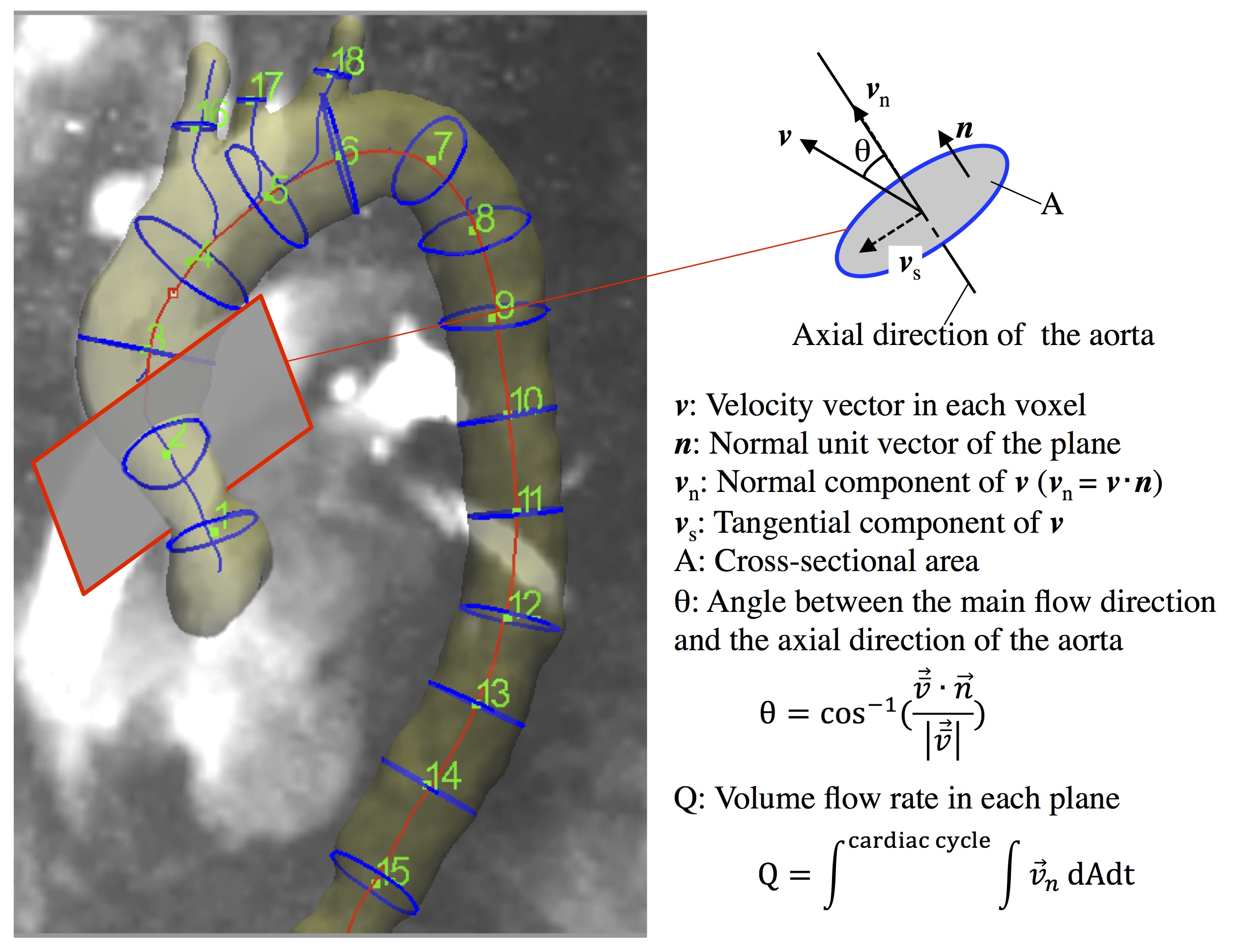
Figure 1: Assessment
of thoracic aortic blood flow by use of 4D flow MRI. 15 planes of aorta (4
ascending, 5 arch, and 6 descending aorta) and 3 planes of the aortic arch
branches (1 per each branch) were set. Axial direction of aorta was defined as
the normal direction of the plane.
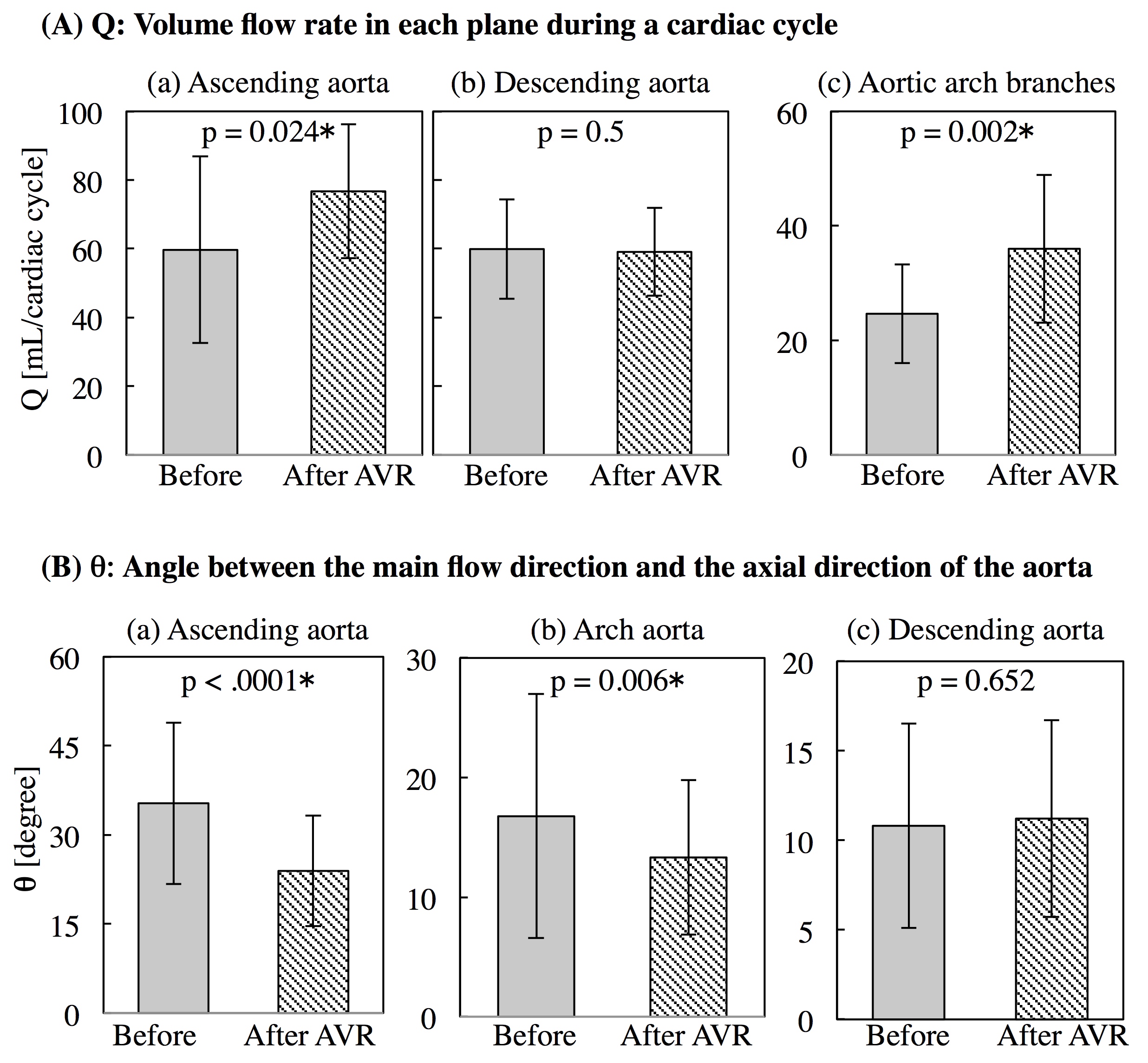
Figure 2: (A)
Volume flow rate (Q) in the ascending (a), the descending aorta (b), and the aortic
arch branches (c) with P-value for Wilcoxon Signed-Rank test. (B) The angle (θ) in the
ascending (a), the arch (b), and the descending aorta (c) with P-value for
Wilcoxon Signed-Rank test.
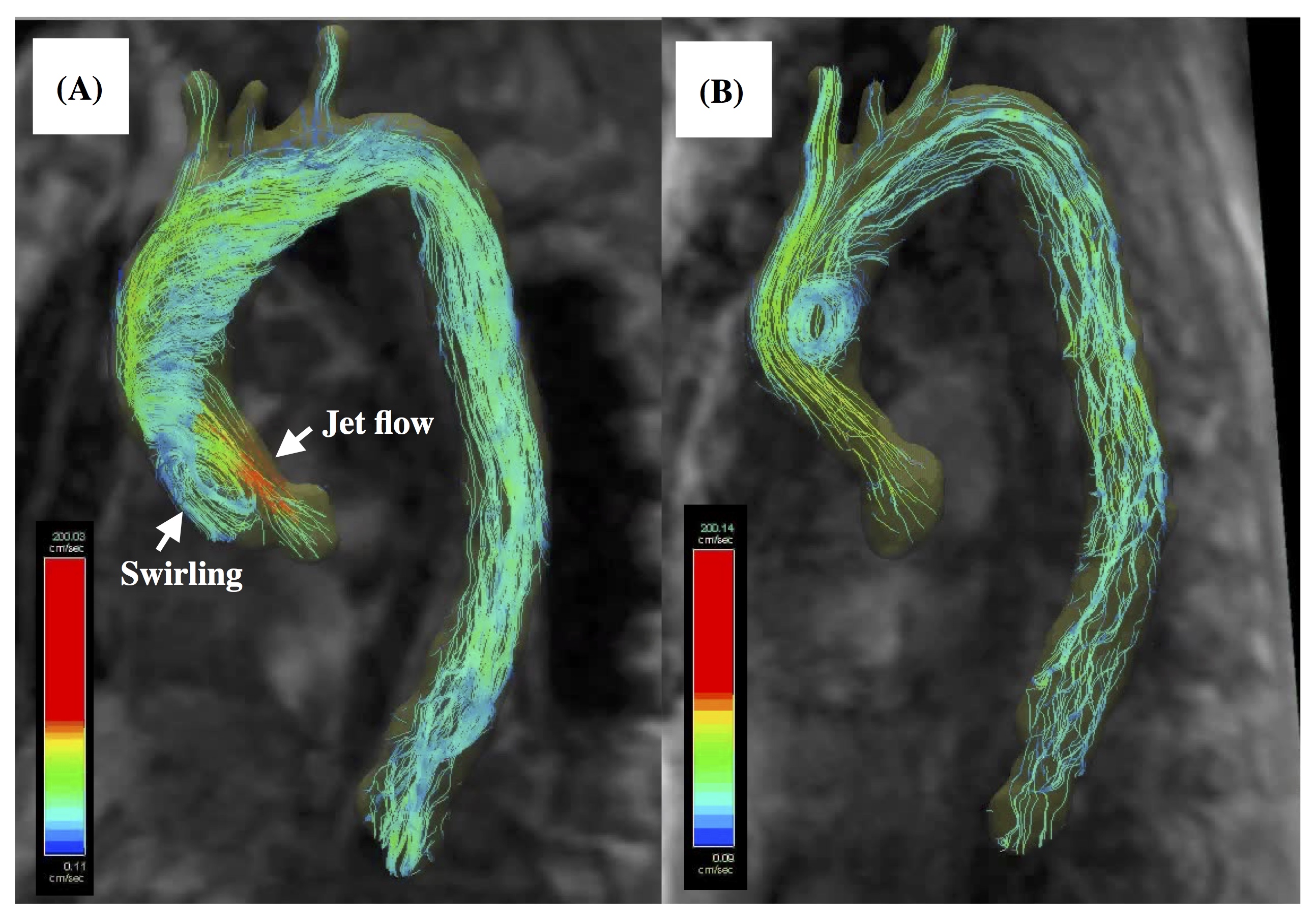
Figure
3: Streamline
of thoracic aorta during systole in this patient where the volume flow rates in
the ascending aorta and the aortic arch branches were remarkably increased after AVR. Jet flow
and swirling flow are observed in aortic root, and secondary flow forms in the
ascending aorta and aortic arch before AVR (A). After AVR, jet flow disappears
in the aortic root and the streamline become to distribute along with grater
curvature of the ascending aorta and arch (B).
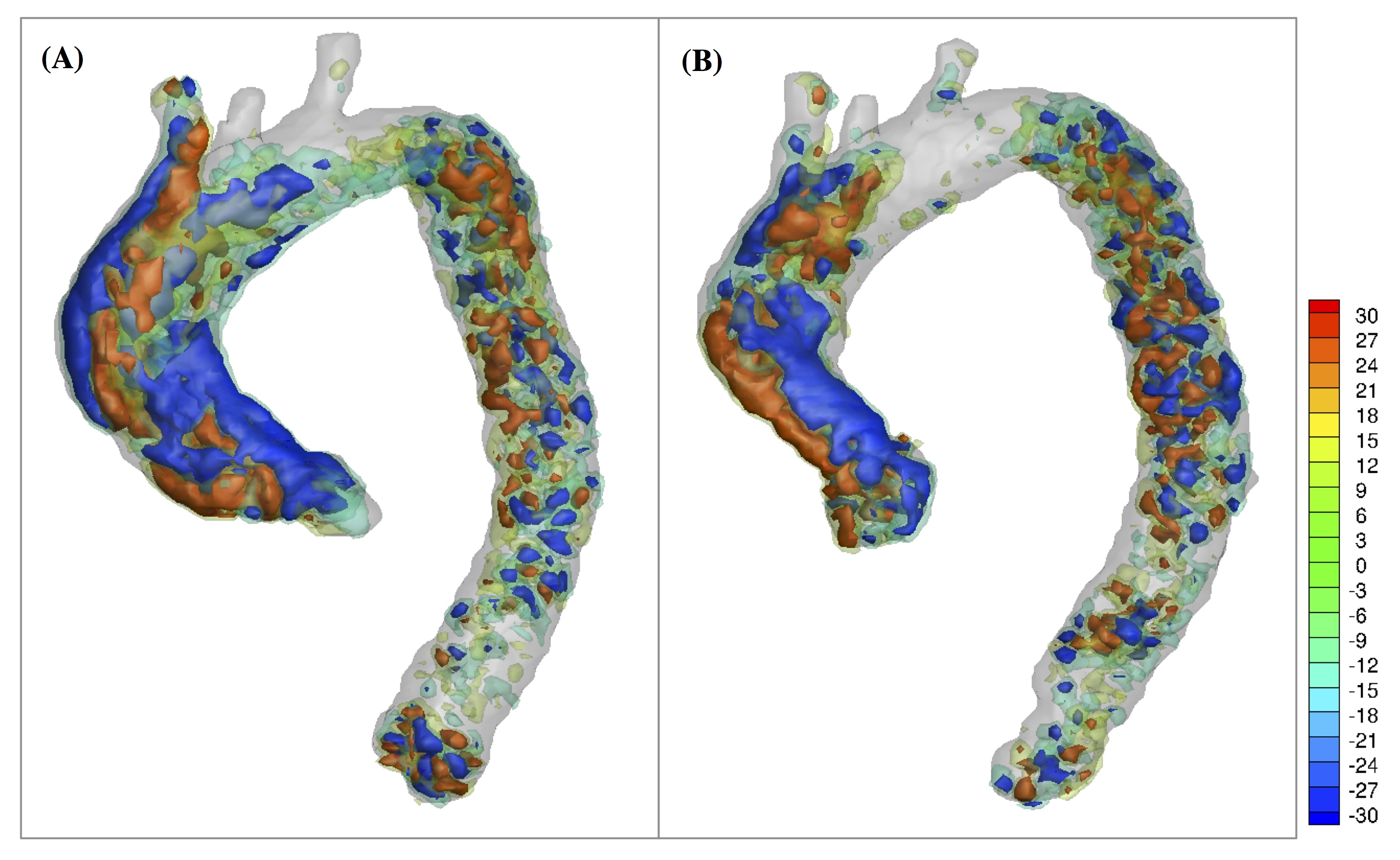
Figure
4: Isosurface plot of helicity density during systole
in this patient where the volume
flow rates in the ascending and the aortic arch branches increased remarkably after AVR. The
helicity density is high in the ascending aorta before and after AVR (A) and
(B), whereas it decreases at arch aorta after AVR (B).