Rectal CA Staging
Synopsis
This lecture will cover the basic information needed to properly perform and interpret baseline MRI for rectal cancer staging. It includes recommended techniques and parameters by the ESGAR 2012/2016 guidelines. It illustrates how to interpret T- and N- staging as well as proper assessment of the CRM and of EMVI. It discusses geographic differences in treatment around the world and also introduces staging of low rectal cancer involving the anal sphincter apparatus.
Target Audience
The information in "Rectal Ca Staging" will benefit all physicians, but particularly radiologists in training and in practice, whether academic or private, because the field and knowledge is one of active research and new knowledge almost on a monthly basis. In addition, technologists may benefit from this talk which illustrates and focuses on important technical parameters and why they matter, including what Guidelines have been/are being adopted in Europe and in the USA.Outcomes and Objectives
At the end of this lecture, the participant will be able to do the following:
- > Understand the requirements for performing a good quality, high resolution rectal MRI
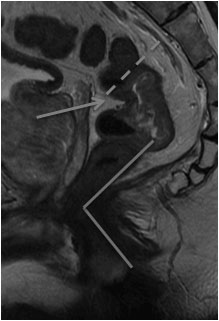
- > Locate and describe general characteristics of a rectal primary tumor
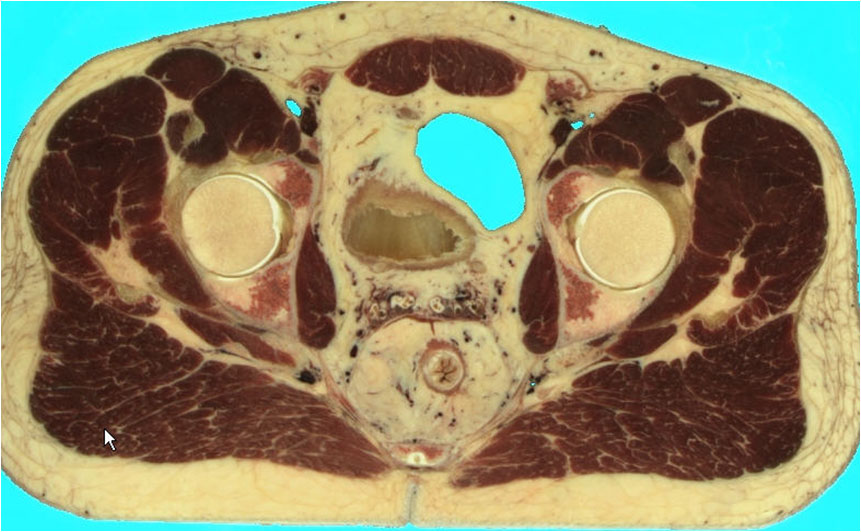
- > Measure, in a reproducible way, the tumor and its relationships with important surrounding anatomic landmarks that the surgeon and radiation and medical oncologoist need to know.
- > Perform clinical (radiologic) Tumor and Nodal (and Metastatic) staging [TNM], understanding the limitations of what they have found, and the implications of these limitations
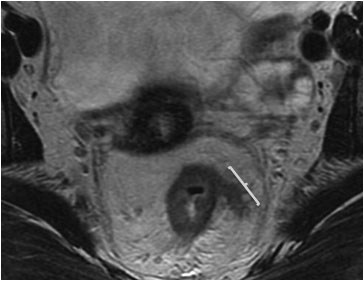
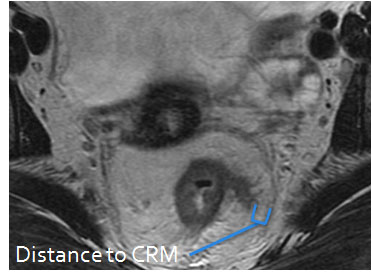
- > Assess the presence of involvement of the circumferential resection margin (CRM) by tumor and the presence of potential extramural vascular invasion
- > Understand the concepts of different treatment approaches around the world
- > Have a good understanding of the anal canal and anorectal junction anatomy and how to stage the very common and potentially QoL-altering low rectal cancers.
Acknowledgements
No acknowledgement found.References
> Beets-Tan RG, Lambregts DM, Maas M et al. Magnetic resonance imaging for the clinical management of rectal cancer patients: recommendations from the 2012 European Society of Gastrointestinal and Abdominal Radiology (ESGAR) consensus meeting. Eur Radiol. 2013 Sep;23(9):2522-31
> The MERCURY study group. Extramural Depth of Tumor Invasion at Thin-Section MR in Patients with Rectal Cancer: Results of the MERCURY Study. Radiology 2007; 243:132–139
> N. J. Smith, Y. Barbachano, A. R. Norman et al. Prognostic significance of magnetic resonance imaging-detected extramural vascular invasion in rectal cancer. British Journal of Surgery 2008; 95: 229–236
> Gina Brown, Catherine J. Richards, Michael W. Bourne, et al. Morphologic Predictors of Lymph Node Status in Rectal Cancer with Use of High-Spatial-Resolution MR Imaging with Histopathologic Comparison. Radiology 2003; 227:371–377
Figures