Introduction To Cerebrovascular Reserve & Its Measurements
Jill De Vis
Synopsis
Cerebrovascular reserve is a marker of the brain's ability to compensate for a decreased perfusion pressure which would otherwise lead to a decreased cerebral blood flow with consequently ischemic events. In this lecture we will describe the concept of cerebrovascular reserve, we will briefly go through the different MRI methods to evaluate the cerebrovascular reserve and we will describe the challenges available to assess the cerebrovascular reserve.
Background and purpose
Cerebrovascular reactivity or cerebrovascular reserve capacity (CVR) refers to the capacity of the brain’s vasculature to increase cerebral perfusion by vasodilatation (Figure 1) [1]. This increase may be necessary when the perfusion pressure towards the brain is decreased, e.g. in case of steno-occlusive cerebrovascular disease [2]. Thereby, a measurement of cerebrovascular reactivity provides insight into how close the brain is to exhaustion of this reserve capacity, and thus, to a possible shortage of brain perfusion leading to ischemic events. Positron Emission Tomography (PET) and single-photon emission computed tomography (SPECT) have always been the brain imaging standard for the assessment of cerebrovascular reactivity. However, both require a radioactive tracer and ionizing radiation which makes them less suited for clinical use. A non-invasive approach has been transcranial Doppler ultrasonography (TCD). However, TCD measurements are limited to the brain-feeding vessels and thus provide no regional assessment of CVR. The invasiveness of PET/SPECT, and the limitations of TCD have led to a search for non-invasive alternatives. Currently, phase-contrast (PC) MRI, blood oxygen level-dependent (BOLD) MRI and arterial spin labeling (ASL) MRI are the non-invasive MRI-based imaging techniques which are used to obtain a measure of either global CVR (in the case of PC MRI) or regional CVR (in the case of BOLD and ASL MRI). Similar to PET/SPECT and TCD, these more novel techniques have to be paired with a vasodilatory challenge to enable an evaluation of the CVR.Methods
The cerebrovascular reserve is evaluated by comparing the brains blood flow at baseline status to the brains blood flow when a vasodilatory stimulus is administered to the subject. In order to assess the cerebrovascular reserve capacity one needs two things: (1) a technique which can assess the brains blood flow, and (2) a stimulus which causes dilatation of the brains blood vessels. There are three MRI techniques which allow non-invasive assessment of the brain’s blood flow; PC MRI, ASL MRI and BOLD MRI. PC MRI assesses the blood flow towards the brain at the level of the brain’s feeding arteries (thus, the brains blood flow equals the blood flow through both internal carotid arteries and through both vertebral arteries). For this, for each vessel, two flow-sensitive datasets are acquired with opposite flow-encoding gradients. Thereby, the flowing protons, or spins, in the blood will obtain a net phase shift in between the acquisition of both datasets while stationary spins (e.g. tissue) do not gain a net phase shift. The magnitude of the phase shift is proportional to the velocity of the spins, and multiplication of this velocity with the vessel’s cross-sectional surface area gives the actual flow (in ml/min) through that vessel. ASL MRI magnetizes (either inverts or saturates) the arterial hydrogen protons in the neck region by applying radiofrequency pulses. The labeled (i.e. inverted or saturated) hydrogen protons within the brain’s feeding arteries will move upwards to the brain’s microvascular bed by means of flow. Therefore, imaging at the brain’s tissue level is only performed after a certain time delay to ensure the arrival and exchange of the labeled hydrogen protons at the microvascular bed and with the hydrogen protons in the brain tissue. Labeled and control images are alternated acquired after which they are subtracted from each other to provide us with an image which solely reflects the brains blood flow or perfusion. Heavily T2*-weighted sequences are used for BOLD MR imaging. The BOLD’s principle is based on differences in magnetic properties between oxygenated and deoxygenated hemoglobin. Deoxygenated hemoglobin is paramagnetic (whereas oxygenated hemoglobin is diamagnetic) which causes a local dephasing of protons which reduces the signal from the tissues in the immediate vicinity. Increased cerebral blood flow leads to an increase in oxygenated hemoglobin thereby increasing the signal. However, it is important to realize that the BOLD signal does not only depend on the brains blood flow, but is also influenced by cerebral blood volume (CBV) and the brains oxygen consumption. Thereby, BOLD MRI is an imaging sequence which does not solely reflects the brain’s blood flow. Different stimuli can be used to dilate the brains blood vessels [4]. A first approach is to modulate a subject’s PaCO­2 which causes vasodilatation through the production of nitric oxide. A subject’s PaCO2 can be modulated by administrating hypercapnia gas mixtures [5] or the subject can simply be asked to hold his or her breath. A second approach is the administration of intravenous or oral acetazolamide, a carbonic anhydrase inhibitor [6]. Acetazolamide causes carbonic acidosis which induces a considerable increase in cerebral blood flow. A third approach is to let the subject perform a functional task which increases the cerebral blood flow to the region which is activated. The typical design of a cerebrovascular reactivity study is to measure the cerebral blood flow both at baseline status as when the vasodilating stimulus is given to the subject. The relative difference in cerebral blood flow then determines the cerebrovascular reserve capacity. BOLD MR imaging is a bit different in the sense that it measures relative signal changes and thereby both the baseline status as the stimulus-status have to be within the same imaging sequence. This makes that BOLD MR imaging can only be performed while alternating between baseline breathing and hypercapnia breathing, or while alternating between rest-status and an activity task. In contrast, PC MRI and ASL MRI reactivity studies can also be performed using acetazolamide as a stimulus. For this, it is important to realize that the baseline scan needs to be performed prior to the scan at vasodilated status as it takes a while before the effect of acetazolamide wears off.Discussion
The decision regarding which MR imaging technique to choose when one wants to evaluate the cerebral blood flow in a reactivity study is a trade-off where on needs to consider if global or regional CVR values are preferred and if one wants to obtain a CVR value which purely reflects the cerebral blood flow. On top of this, the imaging time and the signal-to-noise ratio may also influence the decision. The vasodilatory challenge or stimulus can be chosen based on the imaging sequence which is used, the available equipment and the time allocated for the experiment. For instance, in a clinical setting with limited scan time, inexperienced or little experienced technicians, and no time for complicated set-ups, one might opt for a less sensitive breath-hold approach. In a research setting, a more complicated set-up with exact knowledge of gas input and resulting EtCO2 and ETO2 could be more desirable. Acetazolamide is currently not approved by the food and drug administration (FDA) for use in this setting (off-label use) which may restrict its use in clinical practice.Acknowledgements
No acknowledgement found.References
[1] Derdeyn CP, Grubb RL Jr, Powers WJ: Cerebral hemodynamic impairment: methods of measurement and association with stroke risk. Neurology 1999;53:251–259. [2] Sam K, Small E, Poublanc J, Han JS, Mandell DM, Fisher JA, et al: Reduced contralateral cerebrovascular reserve in patients with unilateral steno-occlusive disease. Cerebrovasc Dis 2014;38:94–100.Figures
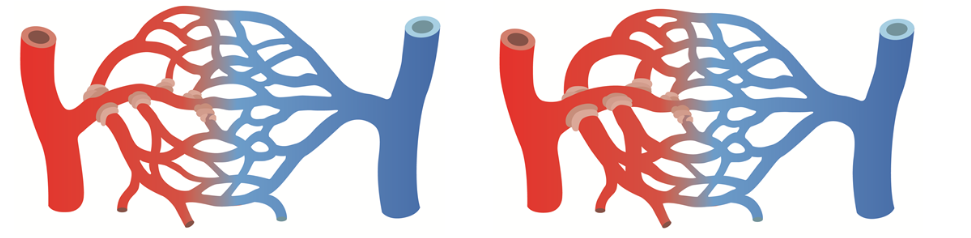
This figure illustrates the concept of cerebrovascular
reserve whereby the figure on the left shows the baseline situation and the
figure on the right shows the microvascular bed in dilated status. The cerebrovascular
reserve is the relative increase in flow which can be obtained through
vasodilatation.