5588
Effect of liver transplantation on muscle metabolism and the abdomen adipose tissue volume in diabetic and non-diabetic patients1MR-unit, Institute for Clinical and Experimental Medicine, Prague, Czech Republic, 2Hepatogastroenterology Department, Institute for Clinical and Experimental Medicine, Prague, Czech Republic, 3Centre of Experimental Medicine, Institute for Clinical and Experimental Medicine, Prague, Czech Republic
Synopsis
Liver transplantation (TxL) is a treatment that rapidly improves the clinical status of patients. However, side effects due to long-term immunosuppressive therapy may negatively influence the function of certain organs and metabolism. 31P MRS and MRI are suitable methods for the clinical examination of muscles and abdomen fat volume in transplanted patients. Our pilot results show that TxL leads to an improvement of resting muscle metabolism in especially in diabetic patients and an increase of volume visceral fat in a short term (six months) after transplantation.
Introduction
Liver transplantation (TxL) is a treatment that rapidly improves the clinical status of patients. However, side effects due to long-term immunosuppressive therapy may negatively influence the function of certain organs and metabolism. The aim of this study was to monitor the effect of TxL on muscle metabolism and the volume of abdomen adipose tissue with respect to diabetes mellitus (DM).Subject and Methods
We examined 90 patients (BMI=27.8±5.1 kg/m2, mean age=56±10 years) with liver dysfunction who had been TxL candidates. 26 subjects underwent transplantation and an MR examination six months after TxL. The post TxL immunosuppressive treatment involved tacrolimus and mycophenolate mofetil (19 patients) and/or corticosteroids (prednisolone or methylprednisolone, 14 patients). DM was confirmed in 13 patients (BMI=29.4±4.7 kg/m2, mean age=59±10 years) both before and after TxL, 10 patients (BMI=24.0±3.2 kg/m2, mean age=59.5±8.5 years) were without DM and in 3 patients (BMI=26.1±4.5 kg/m2, mean age=59.4±4.5) DM de novo developed after TxL. All subjects were informed about the study protocol and signed an informed consent approved by the local ethical committee.
31P MRS
Rest and dynamic 31P MR spectroscopy of calf muscle and MR imaging of the abdominal area were performed at the 3T MR system equipped with a home-made ergometer [1] and dual 1H/31P surface coil. Subjects were examined in a supine position with the coil fixed under the gastrocnemius muscle. 31P MR spectra at rest were acquired by the sequence FID with the following parameters: acquisition delay TE*=0.4 ms, repetition time TR=15 s, 16 acquisitions, vector size of 1024, flip angle FA=90°. The dynamic examination (FID sequence: TE*=0.4 ms, TR=2 s, 2 acquisitions, vector size of 1024, number of measurements=420, FA=42°) consisted of a 6-min plantar flexion (each 2 s, 7.3 kg weights) followed by 6-min recovery [1]. Adenosine triphosphate (ATP), phosphocreatine (PCr), phosphodiesters (PDE) and inorganic phosphate (Pi) and their ratios were evaluated from 31P MR spectra using AMARES (jMRUI software). The drop of PCr (ΔPCr), PCr recovery rate constant (τPCr), mitochondrial capacity (Qmax) and end-exercise pH (pHend) were calculated.
1H MRI of Abdomen
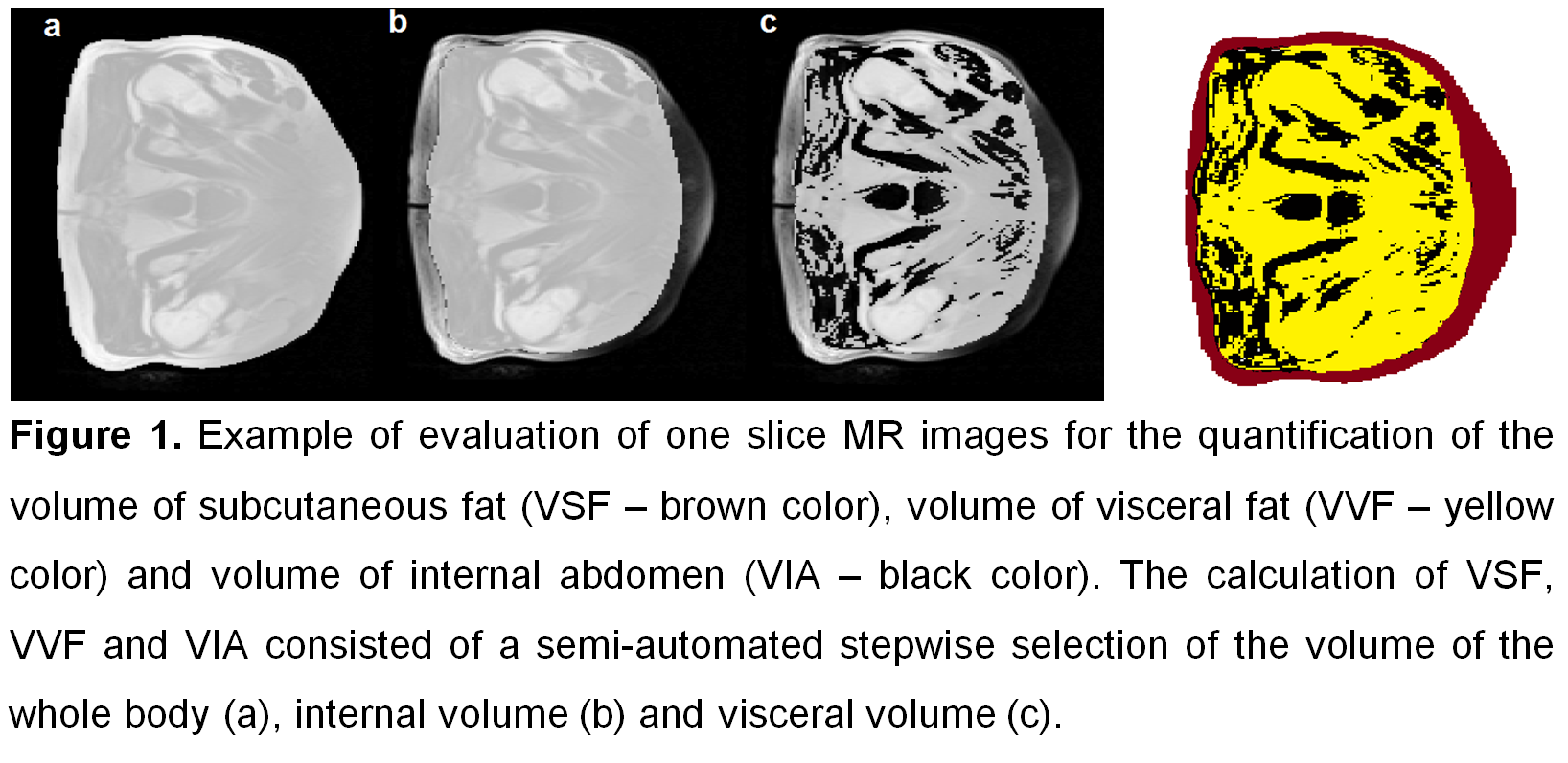
Subjects were examined in a supine position. MR imaging for segmentation routine was performed, body coil and turbo spin echo sequence was used (TR=450 ms, TE=10 ms, 27 slices centered over the umbilicus, slice thickness = 10 mm, matrix = 180*256, six concatenations in a 16-second breath hold). Three different volumes were evaluated (volume of subcutaneous fat (VSF), volume of visceral fat (VVF) and volume of internal abdomen without VVF (VIA – abdominal organs, bones, ascites…), see Figure 1. MR images were evaluated in a program developed in MATLAB.
Statistical evaluation
Results before and six months after TxL were compared by a paired t-test with respect to diabetes mellitus. The probability level of P<0.05 was considered as a statistically significant difference.
Results
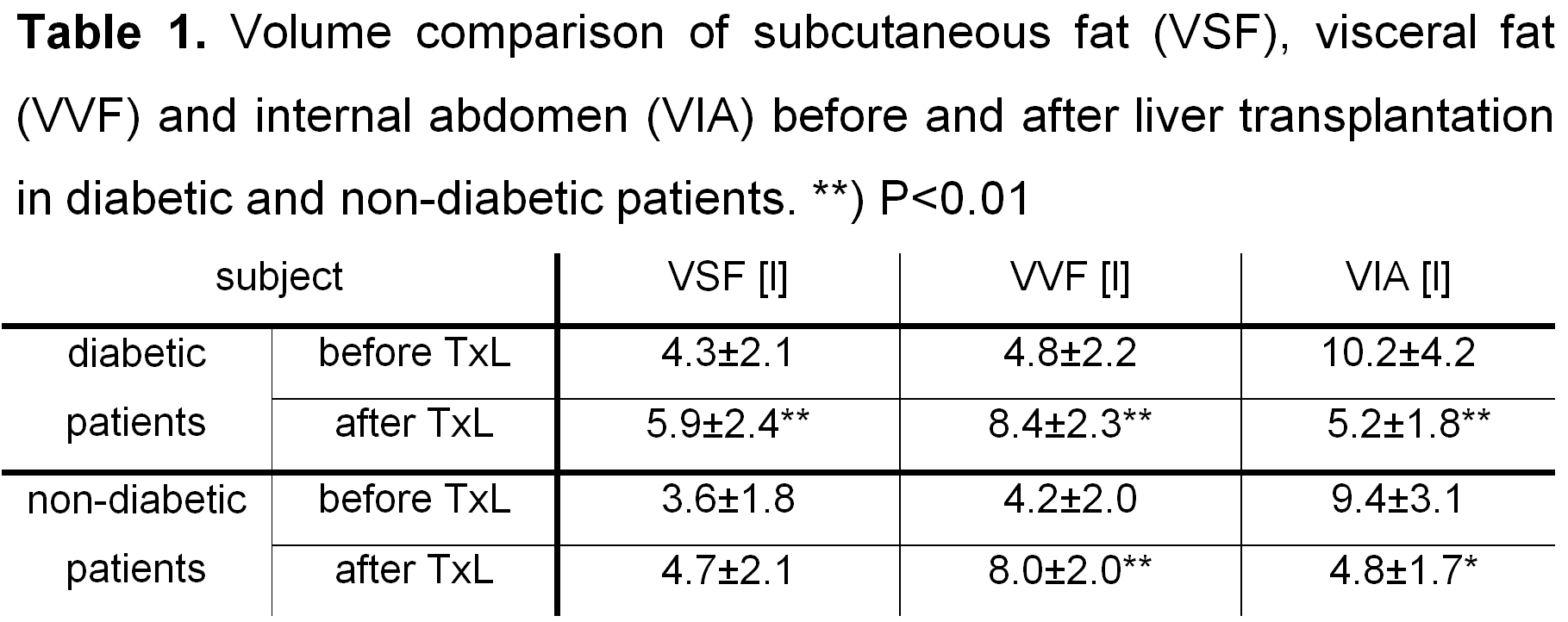
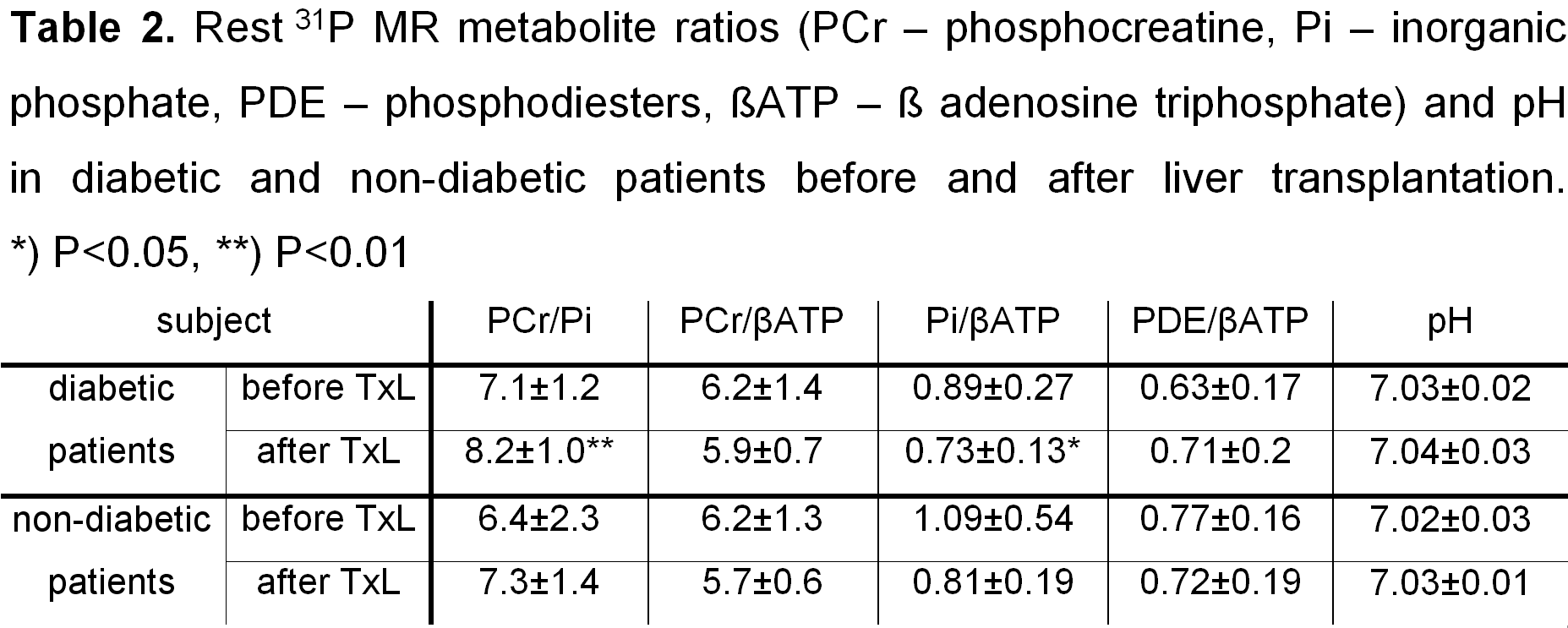
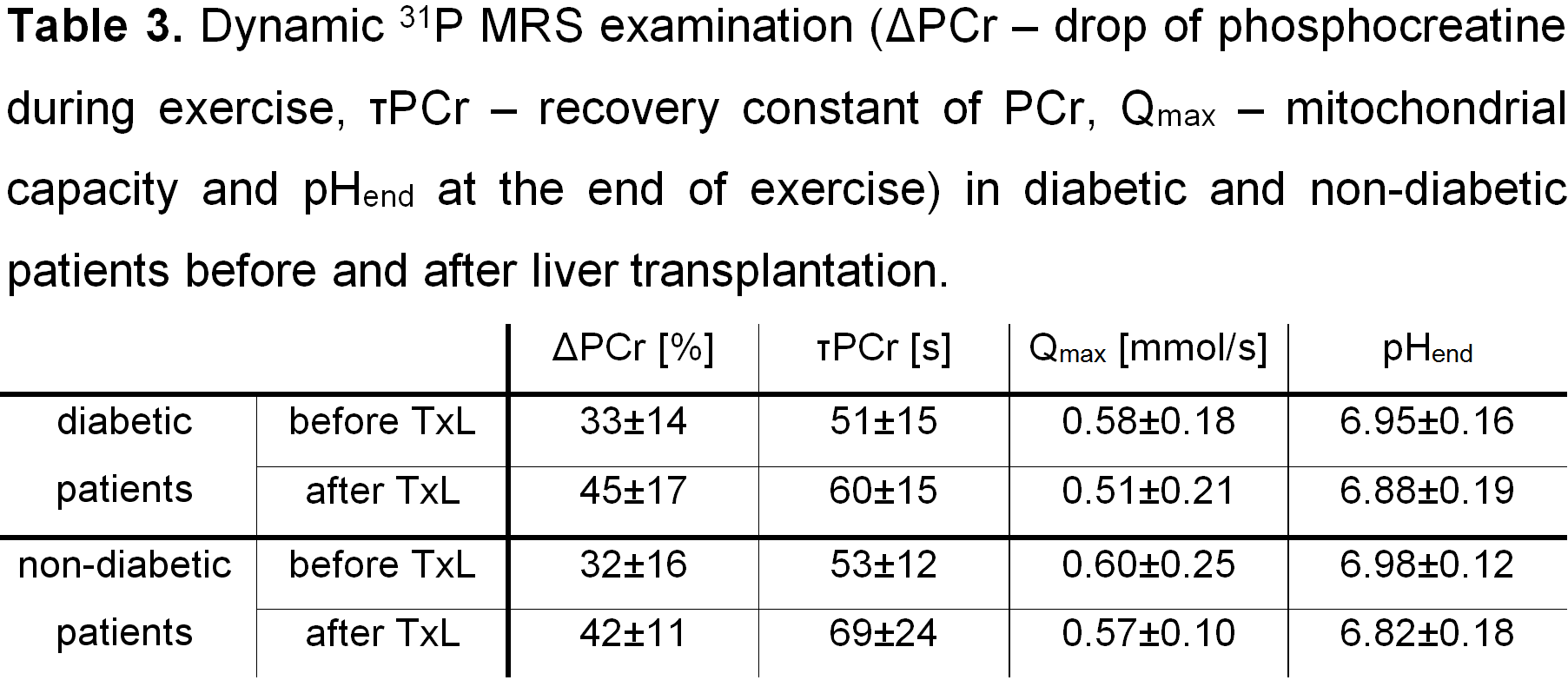
Significant changes were found in the volume of abdomen adipose tissue after TxL (see Table 1). Non-diabetic patients had higher VVF but in diabetic patients even VSF increased after TxL. In muscles, significant positive changes in energy metabolism (see Table 2) were found only at rest in diabetic patients (PCr/Pi increase and Pi/βATP decrease after TxL). Dynamic examination showed the same mitochondrial capacity before and after TxL.Discussion
The volume of visceral fat increased nearly twice compared to the values before TxL in both diabetic and non-diabetic groups, probably due to improved nutritional status after TxL and immunosuppressive treatment. The volume of internal abdomen was reduced mainly due to the absence of ascites. An increasing PCr/Pi and decreasing Pi/βATP indicate an improvement of rest muscle metabolism after TxL in diabetic patients. Nevertheless, oxidative metabolism (mitochondrial capacity) evaluated by dynamic 31P MR spectroscopy remained unchanged or even decreased both in diabetics and non-diabetics after TxL. It can indicate that there can be a development of post-transplant mitochondrial myopathy resulting from long-term immunosuppressive therapy which can also contribute to the development of insulin resistance and DM in TxL patients [2].Conclusion
31P MRS and MRI are suitable methods for the clinical examination of muscles and the volume of abdomen fat in transplanted patients. Our pilot results show that TxL leads to an improvement of resting muscle metabolism in diabetic patients and an increase of volume visceral fat in a short term (six months) after transplantation. Longer follow-up and a higher number of examined patients after TxL is necessary for a more detailed assessment of the TxL impact on muscle and liver metabolism.Acknowledgements
The study was supported by Ministry of Health, Czech Republic AZV:15-26906A and 00023001 IKEM; Institutional support.References
[1] Sedivy P, et al. Dynamic 31P MR spectroscopy of plantar flexion: Influence of ergometer design, magnetic field strength (3 T and 7 T), and RF-coil design. Med Phys. 2015; 42:1678-1689.
[2] Kallwitz ER. Sarcopenia and liver transplant: The relevance of too little muscle mass. World J Gastroenterol. 2015; 21(39):10982-93.
Figures