5587
Use of MR Spectroscopy in Clinical Trials1Center for Clinical Spectroscopy, Brigham and Women's Hospital, Boston, MA, United States, 2Cancer Research UK Cambridge Institute, University of Cambridge, Cambridge, United Kingdom
Synopsis
Magnetic resonance spectroscopy (MRS) is an ideal tool for therapeutic monitoring in clinical trials although its role has not been formally examined. An initial search in a clinical trials database showed 488 studies; however the results were cross-referenced with the scientific literature to yield 61 studies demonstrating the use of MRS in clinical trials. It is most frequently used to study hepatic lipid content, followed by studies of skeletal muscle, and finally the brain, which surprisingly was only 15% of the MRS studies. A review is provided to assess its importance as a non-invasive and quantitative biomarker for disease.
Introduction
The non-invasive and quantitative nature of magnetic resonance spectroscopy (MRS) makes it an excellent endpoint for use in clinical trials of drugs or other clinical interventions. In longitudinal studies, MRS can be performed repeatedly with no harmful consequence to the patient or the clinical target, unlike biopsy or other invasive measures. As a direct or surrogate biomarker, MRS is sensitive to the effects of medications that can be readily compared and correlated to other clinical measures. Since the publication of Evidence-Based Medicine (EBM) meta-analyses1, it is encouraging to see that MRS is being used in an increasing number of clinical trials. While some studies remain small, there are now many more clinical trials with significant cohort sizes that meet EBM criteria. This educational abstract will provide an overview of the use of MRS in recent clinical drug trials2.Methods
The US National Institutes of Health (NIH)-supported ClinicalTrials.gov website is a registry of all clinical trials ongoing in the United States. As the results are not peer-reviewed, it is difficult to judge the quality of the studies from the limited information on the website. Fortunately, entries in the registry are tied to PubMed.gov, a citations database of published peer-reviewed literature. These two resources were used in combination to determine the extent of use of MRS by using “magnetic resonance spectroscopy” as a search term in ClinicalTrials.gov and then subsequently utilizing those results within PubMed by using the search terms: “clinicaltrials.gov[si]” and "magnetic resonance spectroscopy". The resulting list of publications was reviewed to eliminate those studies that did not utilize in vivo MRS (for example, the use of high resolution NMR or MRS for the characterization of blood and other body fluids, was eliminated). Individual studies were then further reviewed to include only prospective studies utilizing an intervention. For the purposes of this review, interventions included both pharmaceutical and non-pharmaceutical (i.e. diet changes or exercise changes) interventions.Results
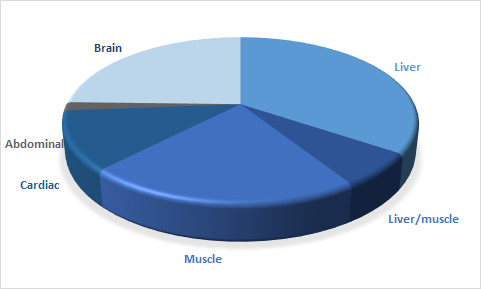
The initial search on ClinicalTrials.gov found 488 registered studies that utilize MRS as part of the study description or intervention. Of those studies, 318 (65%) were interventional studies as opposed to observational studies. 195 of the studies focused specifically on a pharmaceutical drug intervention. This result demonstrates that there is substantial interesting in using MRS in clinical trials, particularly for the evaluation of treatment effects. The initial PubMed search, which included the ClinicalTrial.gov results, yielded 96 studies. Initial review of the study abstracts showed that 74 of those studies utilized in vivo MRS methods. Of those 74 studies, 61 focused on a specific intervention as opposed to a cross-sectional study. In almost all of these studies, the study design included controls with a placebo or equivalent existing medication. The majority of the clinical drug trials focused on the use of MRS in the liver, specifically to measure hepatic lipid content in 25 studies (41%). The second largest group of studies focused on studying skeletal muscle (n 17, 28%) using 31P (n=9) and 1H MRS (n=9, including one study used both 31P and 1H) methods. The study counts of these two groups include four studies where both hepatic and skeletal muscle lipids were studied in the same patient. The next largest group of studies focused on the brain, with 15 studies (25%) using multiple endpoints such as N-acetylaspartate (NAA), cholines (Cho), glutamate (Glu), γ-aminobutyric acid (GABA), etc., and one study using 31P MRS to measure brain energetics. Similarly both 31P (n=4) and 1H MRS (n=3) were also used in seven cardiac interventional clinical trials representing 11.5% of the total studies. Finally, one study used MRS to monitor abdominal and pelvic tumors. The mean number of subjects in each study was 37, with a range of 7 to 154 subjects. 11 of the studies had 50 or more subjects and 65% of the studies showed significant differences and were therefore sufficiently powered.Discussion
Given the relative ease of acquiring spectra from the brain (with typically no need for motion correction, for example), it is somewhat surprising that there have been fewer clinical trials using MRS in the brain than in the liver and muscle. Issues such as reproducibility and differences in protocols, may play a role; however one of the main differences is that unlike liver and muscle spectroscopy, where the measures are direct assessments of lipid or energetics, neuro-spectroscopy metabolites such as NAA are putative and indirect markers of brain health. It is perhaps that in these direct measures that MRS provides the greatest clinical value.Acknowledgements
No acknowledgement found.References
1. Lin AP, Tran TT, Ross BD. Impact of evidence-based medicine on magnetic resonance spectroscopy. NMR Biomed. 2006;19(4):476-83.
2. Lin AP, Rowland B, Griffiths JR. Clinical Trials that Utilize MRS as a Biomarker. eMagRes. 2016; 5(2): 1139–1146.
Figures