5553
Investigation of Phase-only Cross Correlation (POCC) for Passive Marker Tracking with a limited Number of Projections1Dept. of Radiology, Medical Physics, Medical Center – University of Freiburg, Freiburg, Germany
Synopsis
In MR-guided interventions passive markers serve as needle guides for percutaneous biopsies and can be followed automatically to visualize the planned needle trajectory. This is achieved by tracking techniques which acquire two cross-sectional Cartesian tracking images of a cylindrical marker to determine the position information. We show that the implementation of radially undersampled tracking images might be used to reduce the duration of percutaneous needle procedures by about 80%.
Introduction
In percutaneous MR-guided interventions, localization of the interventional device can be achieved with passive markers. For percutaneous biopsies, cylindrical markers with a central opening serving as a needle guide are favorable since they can be safely used in closed bore high field MR systems1. To automatically follow the needle guide and to visualize the planned needle trajectory, passive tracking sequences were proposed to determine the 3D position of the marker from cross-sectional images via a phase-only cross correlation (POCC) algorithm2-4. In its current implementation, the tracking sequence serially acquires full cross-sectional images to localize the passive marker. Unfortunately, serial acquisitions are time-consuming which can lead to suboptimal temporal resolution of the tracking technique and thus prolong the entire interventional procedure.
In this work, we investigate an acceleration method for POCC detection using radial projections to replace conventional Cartesian acquisitions. Cross-sectional marker images are reconstructed from a reduced number of projections and the effect of radial undersampling on the tracking accuracy is assessed.
Methods
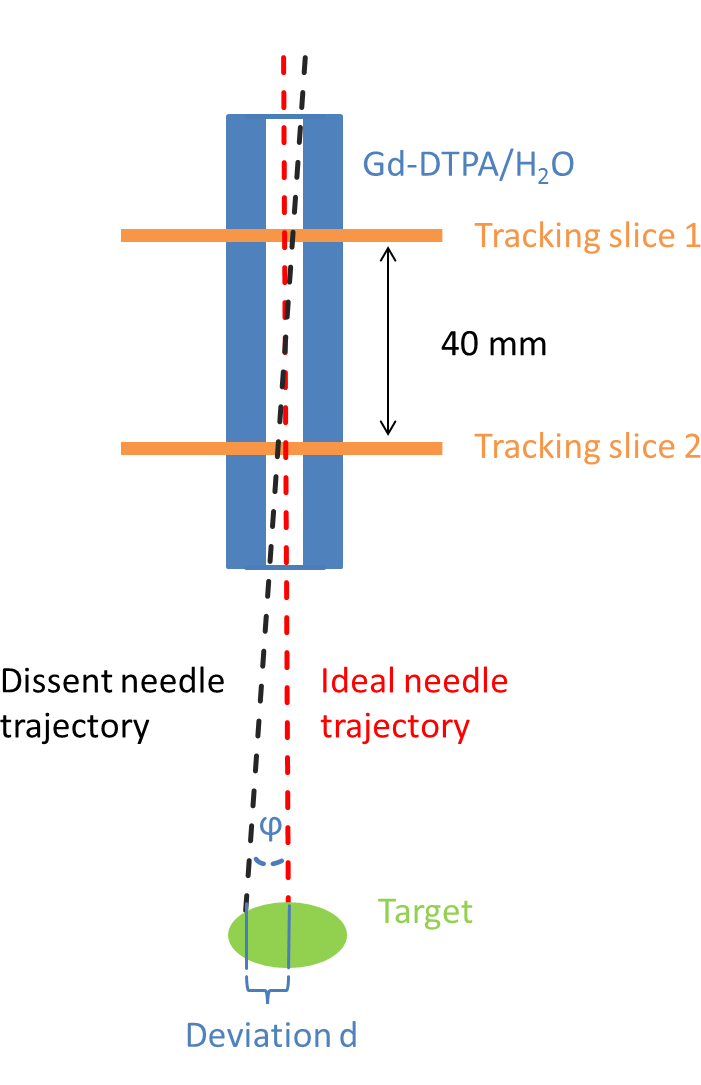
A conventional tracking sequence based on a POCC algorithm2 serially acquires two FLASH images perpendicular to the symmetry axis of a cylindrical passive marker filled with a contrast agent (Gd-DTPA/H2O 1:100). The tracking images display the passive marker as a ring structure which can be detected automatically by the POCC algorithm. The position information is then used to align a subsequent targeting image (bSSFP contrast) in parallel to the marker’s axis and visualize the planned needle trajectory in real-time. The duration of one tracking cycle (two FLASH and one bSSFP acquisition) and therefore 2/3 of the targeting procedure depends on the acquisition of the tracking images.
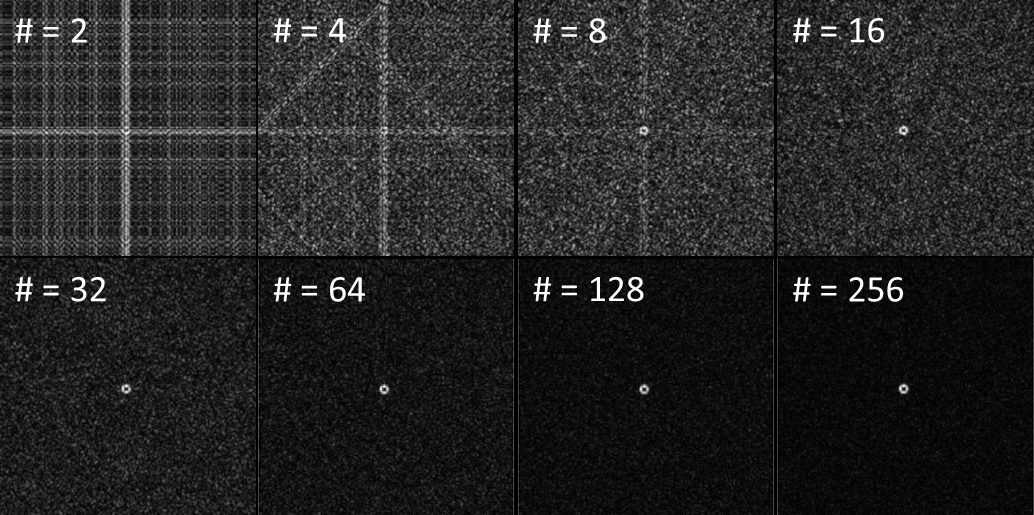
To investigate if the conventional Cartesian tracking images can be replaced by faster radial imaging reconstructed from a limited number of projections, we performed an initial accuracy study on a raw data set acquired in a 3T whole body MR system (Siemens Prisma) using a loop coil for signal reception. The raw data set consisted of a series of 20 images. Each image collected 512 evenly spaced radial projections (TR/TE = 5/3 ms, α = 20°, FOV: 300×300mm, matrix: 192×192) and was oriented perpendicular to the symmetry axis of a commercially available passive marker (Invivo GmbH, Schwerin, Germany).
Radially undersampled images were reconstructed from the raw data in subsets with 2n radial spokes (n=1,…,8, Fig. 1). Radial image reconstruction was done via Kaiser-Bessel regridding and subsequent Fourier-Transform. To assess the acceleration limits, the position of the marker was determined with subpixel precision based on a POCC algorithm for each image using an ideal (i.e. noiseless) theoretical marker image as reference. The mean positions averaged over each subset of 20 images, the standard deviations sx and sy as well as the root-mean-square error $$$Δz=\sqrt{s_x^2+s_y^2}$$$ were calculated. To estimate the position error caused at a distal target, the marker position was first determined in the high resolution radial images with 512 radial spokes. From this data, the deviation of the needle trajectory could be estimated at a target distance of 80 mm (conventional needle length, Fig. 3).
Results & Discussion
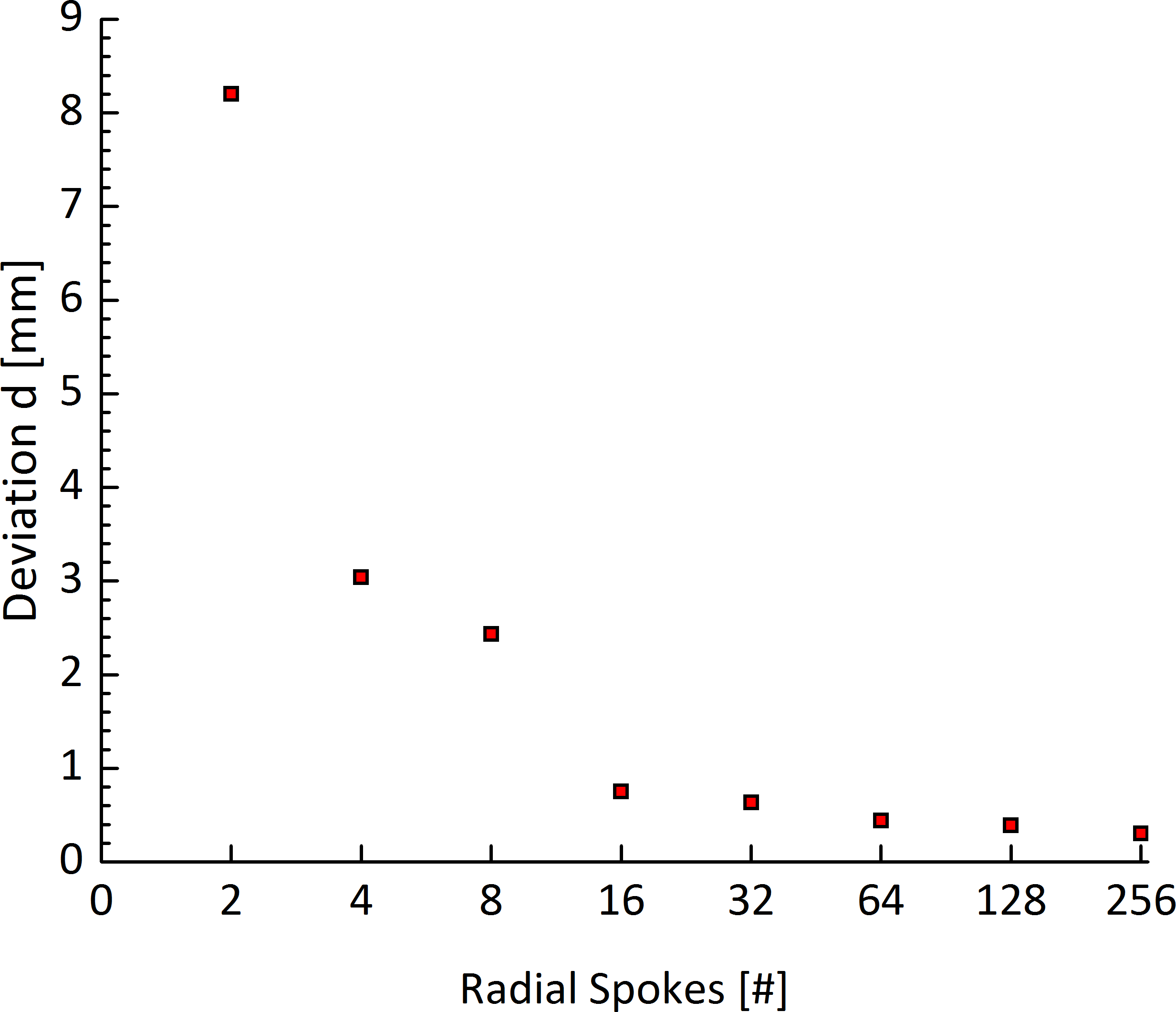
By decreasing the number of projections from 256 down to 16, only a minor increase of up to 0.8mm could be observed in the estimated target deviation $$$d$$$. For an even lower number of projections, the deviation is rapidly increasing.
Compared to the targeting accuracy of 1.5±0.9mm measured for the standard tracking sequence2-3, a deviation of 0.8 mm appears acceptable for clinical applications4. However, our result only represents a best-case scenario (e.g. no distortions from marker movements or surrounding anatomy), and should therefore be verified experimentally in more realistic experimental settings. We also did not take into account that signal intensity can vary between the different tracking slice positions which could downgrade or –in the case of a better receiving coil – improve the POCC detection. In future, an improvement in POCC-based marker detection in undersampled images could be achieved by incorporating a reference image which takes the corresponding point spread function into account5.
Our initial study demonstrates that it is technically possible to decrease the number of radial projections to as less as 16 while maintaining a reasonable targeting accuracy. The implementation of radially acquired tracking images could decrease the acquisition duration to 16/192 per tracking image or even less. This acquisition technique might be used to achieve an 80% acceleration of one tracking cycle and thus to reduce the overall duration of percutaneous needle procedures.
Acknowledgements
We would like to thank for the grant support from the DFG under grant number HA 7006/1-1.References
1. Beyersdorff, D. et al. MR Imaging–guided Prostate Biopsy with a Closed MR Unit at 1.5 T: Initial Results. Radiology 234, 576–581 (2005)
2. de Oliveira A, et al. Automatic passive tracking of an endorectal prostate biopsy device using phase-only cross-correlation. Magn Reson Med 59:1043–1050 (2008)
3. Krafft AJ, et al. Passive marker tracking via phase-only cross correlation (POCC) for MR-guided needle interventions: Initial in vivo experience. Physica Medica 29:607-614 (2013)
4. Zamecnik P, et al. Automated Real-time Needle-Guide Tracking for Fast 3-T MR-guided Transrectal Prostate Biopsy: A Feasibility Study. Radiology 273:879-886 (2014)
5. Scheffler, K. & Hennig, J. Reduced circular field-of-view imaging. Magn. Reson. Med. 40, 474–480 (1998)
Figures