5444
Neurological MRI protocols for patients with DBS equipment in situ consistent with new B1+RMS -limited MR Conditional product label1Lysholm Department of Neuroradiology, National Hospital for Neurology and Neurosurgery, University College London Hospital, London, United Kingdom, 2Department of Brain Repair and Rehabilitation, Institute of Neurology, University College London, London, United Kingdom, 3Translational Imaging Group, Centre for Medical Image Computing (CMIC), Department of Medical Physics and Bioengineering, University College London, 4Unit of Functional Neurosurgery, Institute of Neurology, University College London
Synopsis
We modified routine clinical head MRI protocols to be compliant with a new MR conditional product label for deep brain stimulation (DBS) devices limiting B1+RMS to ≤2.0μT. 12 healthy volunteers were scanned using the routine and modified protocols. Quantitative signal to noise (SNR) and contrast to noise ratio (CNR) analysis was performed, as well as blinded rating of images by a neuroradiologist. Routine and B1+RMS -limited sequences yielded very similar SNR and grey vs. white matter CNR values, indicating that the B1+RMS condition had been achieved with minimum impact on image quality, consistent with the neuroradiologist’s qualitative assessment.
PURPOSE:
To date patients with deep brain stimulation (DBS) devices have effectively been denied formal access to MRI due to safety concerns. For certain devices product label-compliant MRI had been limited to brain imaging only using a transmit/receive head coil and very low specific absorption rate (SAR<0.1W/Kg). These restrictions meant that relatively few centres offered MRI to patients with MR conditional DBS implants, and then with compromised diagnostic quality. Scanner-reported B1+RMS has been proposed as an alternative metric to control RF power deposition for specific implants1,2. In 2015 Medtronic introduced significant changes to the MR Conditional labelling for their DBS systems. In particular, DBS patients with eligible systems can now be scanned anywhere in the body using the whole body transmit coil up to a B1+RMS limit of 2.0μT in addition to other restrictions detailed in the product labelling. The purpose of this study was to establish in healthy volunteers the feasibility of clinical routine brain MRI protocols compliant with B1+RMS≤2.0μT, taking into account acquisition time compromises and the resulting image quality.METHODS:
Twelve healthy adult volunteers underwent MRI at 1.5T (Siemens Avanto) in whole-body transmit mode with the standard 12-channel receive only head coil. Coronal T2 weighted, coronal FLAIR and axial T1 weighted brain scans were acquired for each subject with both clinical sequences used routinely in our neuroradiology centre, and locally optimised sequences where the B1+RMS was limited to 2.0μT, without repositioning between scans. The SNR, CSF vs. brain CNR, grey vs. white matter CNR, image sharpness and artefacts were rated by an experienced neuroradiologist who was blinded to the sequence type. Additionally for each data set quantitative analysis was performed based on anatomical labelling using a geodesic information flow approach3: the total white matter and cortical grey matter SNRs and the total white vs. cortical grey matter CNR were computed, to enable statistical comparison between the routine and B1+RMS -limited protocols.RESULTS:
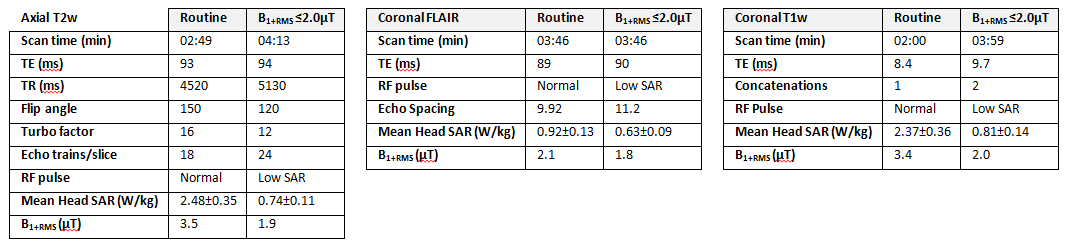
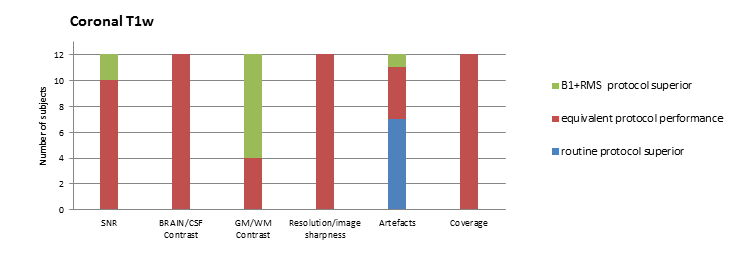
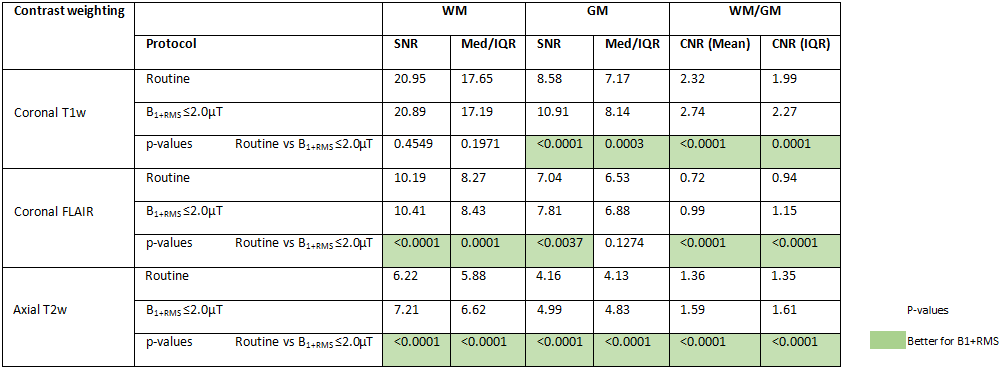
For both T2 and T1-weighted sequences scan time was increased in the B1+RMS limited versions compared to the original due to changes in TR, Turbo factor and number of concatenations, whilst for the FLAIR the B1+RMS reduction was achieved simply by changing the RF pulse type, thus scan time remained the same (Table 1). There was a 28.7% increase in total scan time with the modified protocol. For the B1+RMS limited sequences, head SAR varied between 0.5-1.1 W/kg according to body-weight and other contributing factors, whilst the B1+RMS as expected was essentially constant between subjects. All images were considered to be of a clinically diagnostic standard: the per-subject inter-scan differences were in general small, for nearly all assessments in each of the three contrast-weightings, for the majority of subjects the quality of the B1+RMS limited scans was either equivalent to, or exceeded, the performance of our routine protocols. For the B1+RMS-limited T1 weighted scans an increase in artefacts mainly related to motion was observed presumably due to the increased number of concatenations and consequently longer scan time, but this also led to reduced slice-slice cross talk compared with the equivalent routine protocol. Quantitative analysis for the routine and B1+RMS -limited sequences yielded very similar SNRs and GM/WM CNRs, indicating that the B1+RMS condition had been achieved with minimum impact on these measures. SNR, CNR and p-values from paired tests are shown on Table 2.DISCUSSION /CONCLUSION:
B1+RMS limited product-label compliant versions of routine brain protocols were created by adjusting sequence parameters while aiming to maintain image quality. Quantitative image analysis and radiologist image review showed new sequences produce images of similar or marginally better image quality to the routine protocols currently being used in our centre. This protocol will allow a growing number of patients with in situ DBS systems to undergo neurological MRI examinations.Acknowledgements
Medtronic PLC provided research funding; the work was supported by the NIHR UCLH Biomedical Research Centre.References
1. EN 60601-2-33:2010 A1:2015 Medical electrical equipment Part 2-33: Particular requirements for the basic safety and essential performance of magnetic resonance equipment for medical diagnosis;
2. ISO/TS10974:2012 Assessment of the safety of magnetic resonance imaging for patients with an active implantable medical device;
3. M. J. Cardoso, M. Modat, R. Wolz, A. Melbourne, D. Cash, D. Rueckert, and S. Ourselin, Geodesic Information Flows: Spatially-Variant Graphs and Their Application to Segmentation and Fusion, 2015 IEEE Transactions on Medical Imaging, vol. 34, no. 9, pp. 1976-1988
Figures