5316
Etomidate anaesthesia for fMRI in mice revisited: Subcutaneous administration facilitates experimental procedures1Pharma Research and Early Development, Roche Innovation Center Basel, F. Hoffmann-La Roche Ltd, Basel, Switzerland
Synopsis
Etomidate has recently been proposed as a hypnotic for high-fidelity fMRI in mice. It largely preserves cerebrovascular autoregulation and basal perfusion, thus providing a large window for hemodynamic-based fMRI readouts. However, commercially available formulations of etomidate come at low concentration and are suitable only for intravenous infusion, hence resulting in large infusion volumes and difficult procedures in small rodents. Here, we demonstrate that fMRI-compatible anaesthesia can be readily achieved upon subcutaneous administration of etomidate formulated as aqueous solution. We further propose to substitute etomidate with its short-acting analogue cyclopropyl-methoxycarbonyl metomidate to avert long recovery times due to subcutaneous depot formation.
PURPOSE
Etomidate has recently been proposed as a hypnotic with favourable properties for high-fidelity fMRI across mouse strains. In contrast to the vascular side-effects of commonly used volatile anaesthetics, etomidate preserves cerebrovascular autoregulation and averts anaesthesia-related vasodilation, thus providing a large window for fMRI readouts based on hemodynamics and cerebrovascular coupling [1]. However, commercially available formulations of etomidate come at low concentrations and are suitable only for intravenous infusion, hence resulting in large infusion volumes and a rather intricate experimental setup in small rodents. Also, etomidate was reported in non-rodent species to have metabolic side-effects due to adrenocortical suppression [2]. Here, we addressed these current limitations with a two-pronged approach: (i) etomidate was reformulated at higher concentration in an aqueous vehicle suitable for subcutaneous delivery and (ii) etomidate was subsequently replaced with shorter-acting analogues, with purportedly lower metabolic liabilities [3, 4]. This approach, and its suitability for fMRI, was assessed with extensive pharmacokinetic and pharmacodynamic studies.METHODS
Etomidate (Sigma Aldrich, Steinheim, Germany), its pyrrole analogue, carboetomidate (in-house synthesis) and the spacer-linked etomidate ester-analogue cyclopropyl-methoxycarbonyl metomidate (CPMM, in-house synthesis) were formulated ready-to-use up to 10 mg/ml in aqueous solution using either hydroxypropyl beta cyclodextrin (up to 25% w/v) or the surfactant Kolliphor HS 15 (up to 25% w/v) as solubilizing agents. Studies were conducted in male C57Bl/6 mice (25-35g) with n≥3 individuals per condition. The respective anaesthetics were injected subcutaneously in the nape of the neck, either as single bolus or as bolus-primed continuous infusion. Anaesthetic depth was evaluated every 5 minutes and scored (0-7) by tests for nociceptive (tail pinch and tactile stimulation of the ear canals), withdrawal (toe pinch) or palpebral (medial eye canthus) reflexes and the response to vibrissal (mechanical deflection) and loud sound stimuli (hand clapping) as well as by the breathing rate and loss of the righting reflex (LORR). Anaesthetic potency of the test compounds was evaluated for different bolus doses, and pharmacokinetic parameters were determined based on multiple micro blood samples (20uL), collected over the time course. Perfusion-MRI was carried out on a BioSpec 9.4T/20cm MR system (Bruker BioSpinMRI, Germany) equipped with a volume resonator for transmission and a surface coil for reception. Perfusion imaging was performed based on continuous arterial spin labelling (CASL) with centred-RARE readout (TR/TE=3s/5.4ms, RARE=32, 128x64 matrix, 20mm x 20mm field of view, 0.6mm slice thickness, 8 slices, 2 averages, 3s labelling, 0.4s post labelling delay).RESULTS AND DISCUSSION
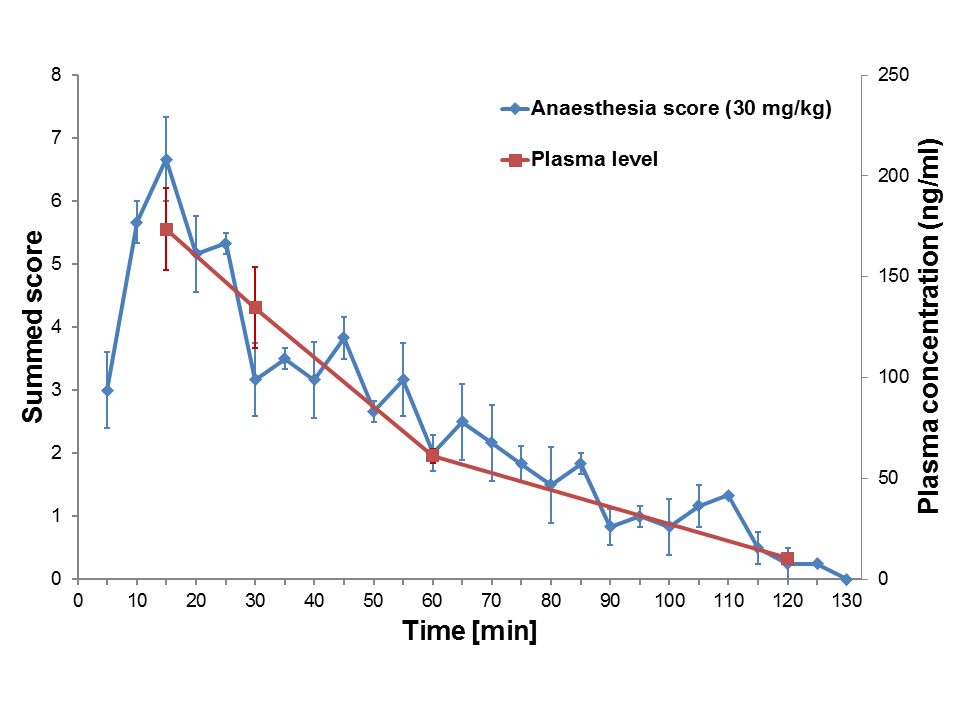
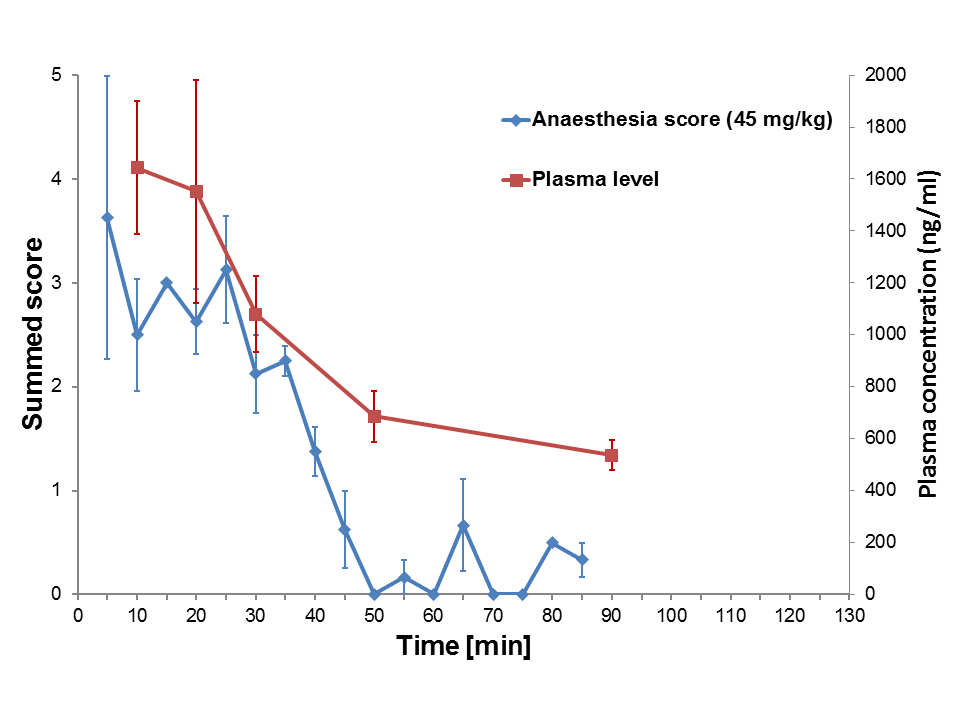
Etomidate administered subcutaneously as a bolus of 30mg/kg elicited adequate anaesthetic potency in mice. LORR was maintained over 85 ±14min (mean ±SD). The further recovery to full consciousness lasted for another ~50min. These pharmacodynamic effects were closely related to the drug’s pharmacokinetics (t1/2=28min) (Fig. 1). Based on these results, an infusion schedule for sustained anaesthesia over 1h was inferred (23 mg/kg bolus, followed by subcutaneous infusion of 0.6 mg/kg/min). However, after discontinuation of anaesthesia, the animals remained half-conscious for a prolonged period; most likely due to slow release of etomidate from a subcutaneous depot. Hence, we resorted to shorter-acting analogues of etomidate for a remedy. Carbo-etomidate up to a dose of 100 mg/kg was ineffective as anaesthetic in mice and thus, was abandoned. On the other hand, CPMM proved almost equipotent to etomidate and, as expected, had a substantially shorter duration of LORR (37 ±5min at 45mg/kg) associated to the rapid initial drug decline (Fig. 2). The subsequent full recovery of consciousness took another ~30min, compatible with the lower rate of terminal elimination of CPMM. As CPMM is a close analogue of etomidate comparable effects on basal perfusion and cerebrovascular reserve capacity can be assumed, though needs to be confirmed experimentally.CONCLUSION
We have demonstrated that fMRI-compatible anaesthesia in spontaneously breathing mice can be readily achieved with etomidate when administered subcutaneously as an aqueous formulation. Yet, slow release from the subcutaneous application site leads to unduly long recovery times. We therefore propose to substitute etomidate with its ester-analogue, CPMM, which can be expected to combine the propitious effects of etomidate on neuro-vasculature along with short-lasting anaesthetic effects.Acknowledgements
R.K. was supported by the Roche Internship for Scientific Exchange (RiSE) programReferences
1 Petrinovic, M.M., et al., A novel anesthesia regime enables neurofunctional studies and imaging genetics across mouse strains. Sci Rep, 2016. 6: p. 24523.
2 Cotten, J.F., et al., Closed-loop continuous infusions of etomidate and etomidate analogs in rats: a comparative study of dosing and the impact on adrenocortical function. Anesthesiology, 2011. 115(4): p. 764-73.
3 Husain, S.S., et al., Modifying methoxycarbonyl etomidate inter-ester spacer optimizes in vitro metabolic stability and in vivo hypnotic potency and duration of action. Anesthesiology, 2012. 117(5): p. 1027-36.
4 Pejo, E., et al., Sedative-Hypnotic Binding to 11beta-hydroxylase. Anesthesiology, 2016.
Figures