5142
The comparison of full FOV and reduced-FOV IVIM Diffusion-weighted imaging of Spinal bone marrow1Department of Radiology, Renmin Hospital of Wuhan University, Wuhan, People's Republic of China, 2GE healthcare China
Synopsis
IVIM (Intravoxel incoherent motion) provides perfusion quantification without the need for intravenous contrast injection, and has been used to the spinal bone marrow lesions1,2. However, diffusion weighted imaging is prone to image deformation, especially with a large FOV. Hence the quantitative measurement of IVIM in spinal bone morrow may be affected. Reduced FOV DWI is known to reduce the level of image distortion, and the purpose of this study is to compare the IVIM parameters obtained using full FOV or reduced FOV imaging.
Purpose
The assessment of perfusion level in spinal bone marrow is of great significance in the diagnosis and post-treatment follow-up of spinal bone lesions. IVIM (Intravoxel incoherent motion) provides perfusion quantification without the need for intravenous contrast injection, and has been used to the spinal bone marrow lesions1,2. However, diffusion weighted imaging is prone to image deformation, especially with a large FOV. Hence the quantitative measurement of IVIM in spinal bone morrow may be affected. Reduced FOV DWI is known to reduce the level of image distortion, and the purpose of this study is to compare the IVIM parameters obtained using full FOV or reduced FOV imaging.Method
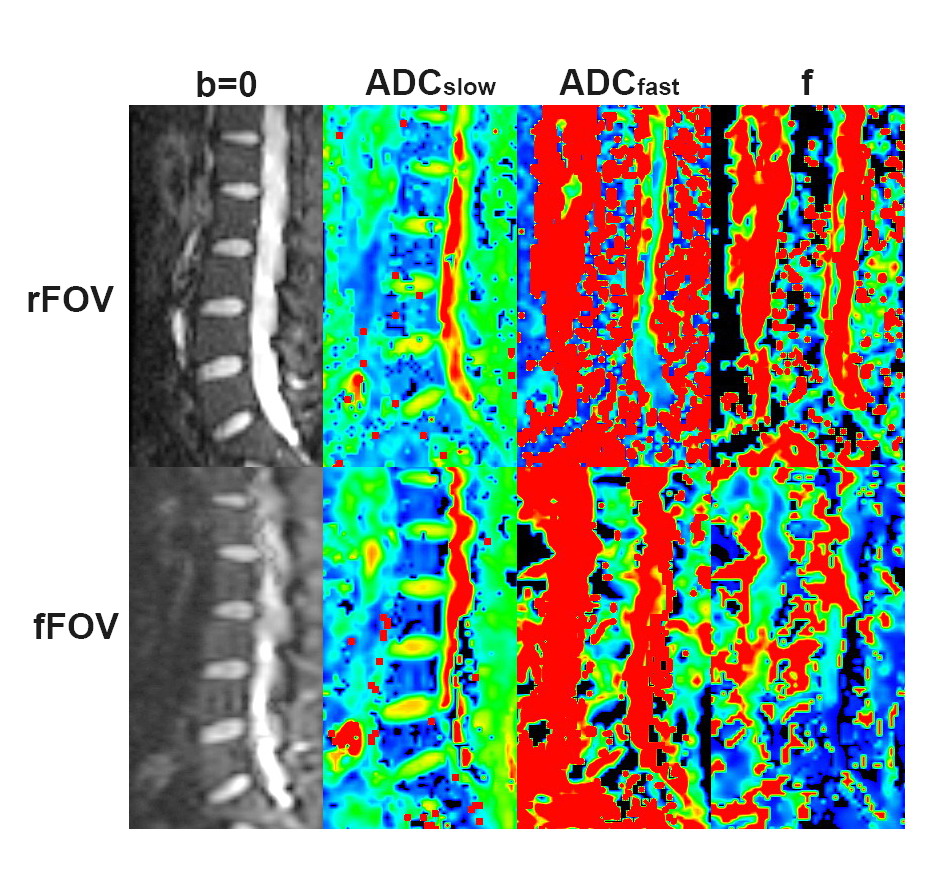
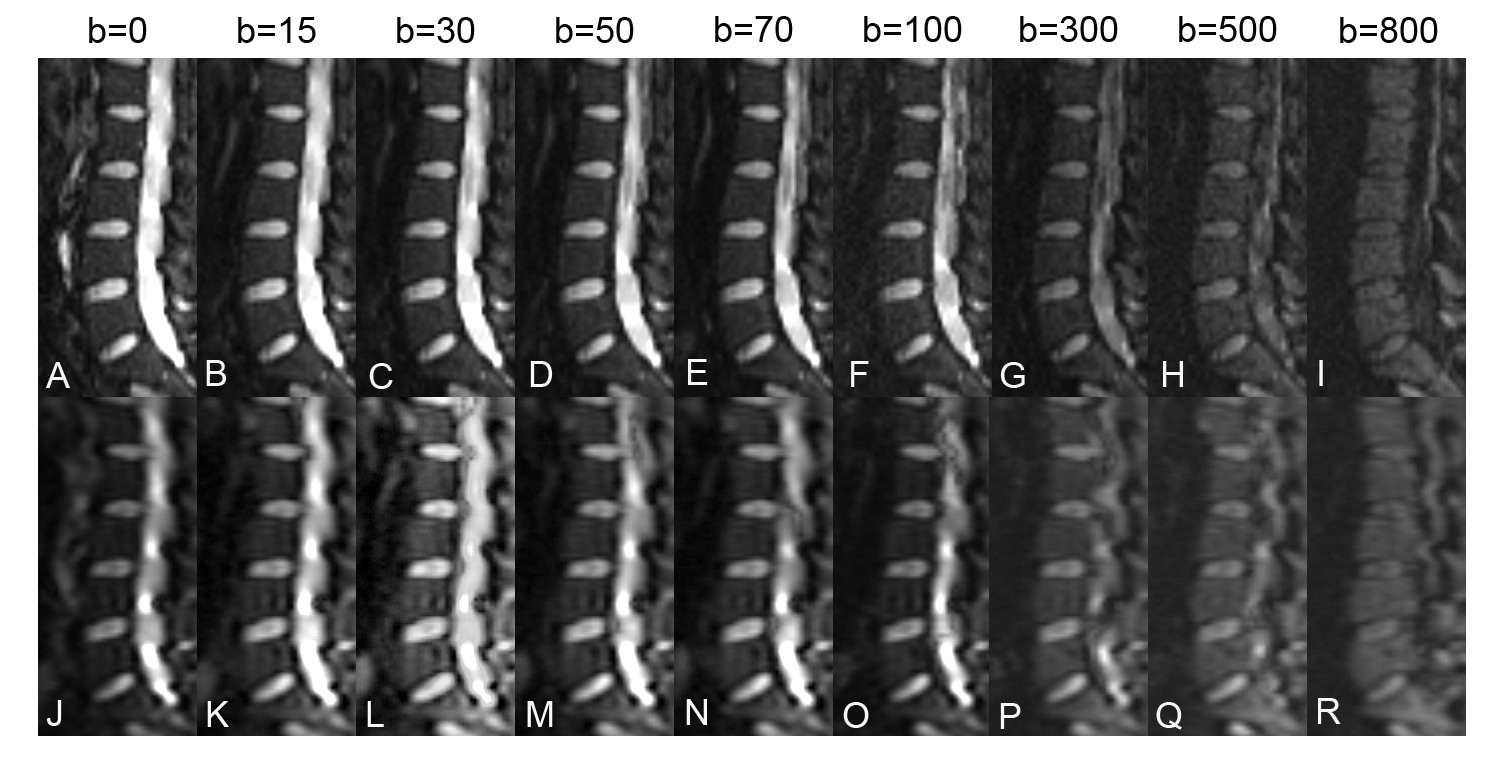
Twenty-six healthy volunteers (12 male, 14 female) with age of 41.12±14.96 years (Mean±SD) were enrolled in this retrospective study. The lumbar imaging protocol included routine anatomical imaging, rFOV IVIM DWI (FOV 32cm×12.8cm, b= 0, 15, 30, 50, 70, 100, 300, 500, 800s/mm2 ) and fFOV IVIM DWI ( FOV 32cm×32cm, b= 0, 15, 30, 50, 70, 100, 300, 500, 800s/mm2 ). Raw rFOV and fFOV IVIM DWI data were post-processed by Functool provided in Advantage Workstation (version 4.6, GE) (Fig. 1), and each vertebral body was selected as a region of interest (ROI). Image quality of rFOV and fFOV IVIM DW images were qualitatively evaluated by using a 5-point Likert scale (Fig. 2). IVIM DWI distortion was quantitatively evaluated by calculate the distortion rate of L3 vertebral body4. Distortion ratio (R) can be defined as: R=|MIVIM—MT2WI|/MT2WI, where MIVIM and MT2WI are the measurements ( area, anteroposterior and craniocaudal distances ) of IVIM DWI and T2WI respectively. IVIM Image qualitatively scale was performed by two radiologists, the parameters and distortion rate were qualitatively evaluated by a third radiologist.The IVIM parameters (ADCslow, ADCfast, f), qualitatively scores, and distortion ratio of the two IVIM DWIs were compared with paired t-test or Wilcoxon's test according to the Kolmogorov-Smirnov test, and the consistency of the two readers was also calculated.Results
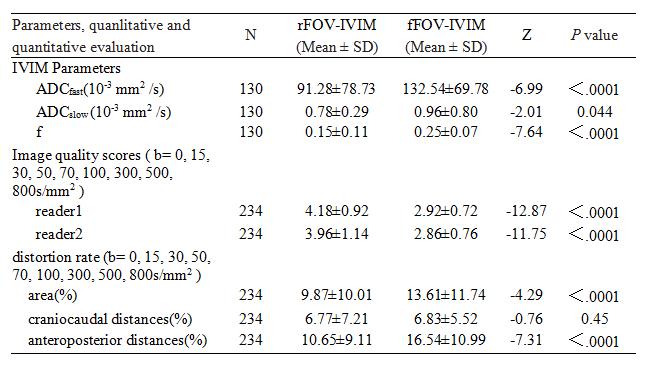
The parametric diffusion maps (ADCfast , ADCslow , f ) of full FOV and reduced FOV IVIM of a typical subject are shown in Fig.1. In this study, statistically significant difference in ADCfast , ADCslow , f , image quality scores, area distortion rate, and anteroposterior distances distortion rate between rFOV and fFOV IVIM DWI were observed, while no significant difference in craniocaudal distances distortion rate between rFOV and fFOV IVIM DWI observed, as shown in Table 1.There was good inter reader agreement in the Image qualitatively scores of rFOV-IVIM DWI (κ=0.68, P<0.001) and fFOV IVIM DWI (κ=0.73, P<0.001) .Discussion and conclusion
The results suggested that compared with fFOV IVIM, rFOV IVIM DW images of spine bone marrow obtained higher Image quality and less deformation artifacts. This phenomenon could be interpreted that IVIM DWI was a set of DWIs with different b-values, and the Standard ss-EPI which constitute fFOV IVIM suffers from severe geometric distortions and T2*-induced blurring because a significant T2* decay and phase error accumulation occurs during the long readout echo train, resulting in degrade the image quality and potentially misleading images, especially at the severe cases of spinal imaging with the magnetic field inhomogeneity around the spine, the small cross-sectional size of the spinal bone, and the increased motion in that area due to breathing and cerebrospinal fluid (CSF) pulsation3,4,5. Reduced field-of-view methods3,4,5which are used in rFOV IVIM DWI decrease the required readout duration for ss-EPI in the phase encoding direction is performed by actively exciting only the part of the rFOV that will be used for imaging. This is achieved by a 90 degree 2-dimensional EPI RF excitation followed by a 180 degree refocusing pulse. There no significant difference in craniocaudal distances distortion rate between the two IVIM DWIs could be interpreted by the less motion artifacts caused by breathing, CSF pulsation and less Susceptibility artifacts from bone-CSF interfaces in the craniocaudal direction. The lower Image quality and higher deformation rate of fFOV IVIM DWI might be the reason for the significant difference in IVIM parameters of the same vertebral body between the rFOV and fFOV IVIM.Acknowledgements
No acknowledgement found.References
1.Bourillon C, et al. Radiology,2015,277(3):773-783.
2.Marchand A J, et al. Magn Reson imaging,2014,32(9):1091-1096.
3.Saritas E U, et al. Magn Reson Med,2008,60(2):468-473.
4.Radhakrishnan R, et al. J Neuroimaging,2015.
5.Andre J B, et al. AJNR Am J Neuroradiol,2012,33(10):1860-1866.
Figures