5117
SEMAC-VAT MR Imaging Increases Clinical Detection Rates of Local Lesions in Patients with Titanium Screws at 3T1Radiology, the Third Hospital of Hebei Medical University, Shijiazhuang, People's Republic of China, 2MR Collaboration NE Asia, Siemens Healthcare, Shanghai, People's Republic of China, 3Siemens Healthcare, Erlangen, Germany
Synopsis
To compare the clinical detection rates in local lesions using the slice-encoding for metal artifact correction (SEMAC) & view angle tilting (VAT) Turbo Spin Echo (TSE) with the standard TSE sequence in patients with titanium screws. Following surgery, patients with reported discomfort at the operation site were examined with both TSE and SEMAC-VAT TSE imaging. They were also examined by digital radiography (DR) and computed tomography (CT). All images were assessed and scored. Despite the long scan time, SEMAC-VAT TSE reduced metal-induced artifacts and may improve the diagnostic sensitivity compared to standard TSE, DR and CT.
Purpose
This study was conducted in patients with titanium screws who had reported symptoms of discomfort at the operation site. The aim was to compare the slice-encoding for metal artifact correction (SEMAC) & view angle tilting (VAT) 1-3 Turbo Spin Echo (TSE) sequence with the standard TSE sequence in terms of detection rates in local lesions, and discuss the clinical value of this technique.Methods
Nineteen patients with musculoskeletal disorders (13 males and 6 females; mean age, 41.3±6.0 years; range, 14-56 years) with titanium screws in the spine (n=8), femur (n=8) and tibiofibula (n=3) after their operation, were examined because of discomfort using a 3T MR scanner (MAGNETOM Verio, Siemens, Erlangen, Germany). The examination included conventional TSE and a SEMAC-VAT TSE sequence. The acquisition parameters for TSE were: FOV of 180×180 mm2 for spine and 300×300 mm2 for extremity, matrix of 320×256, slice thickness of 3 mm, flip angle of 120 degrees, turbo factor of 3. T1-weighted imaging was performed with TE/TR of 6.5/886 ms; T2-weighted imaging was performed with TE/TR of 70/6000ms. T2-weighted imaging with fat suppression was performed with TE/TR of 70/6000ms, TI of 150 ms. The slice-encoding steps were 15 for SEMAC-VAT TSE. All patients were also examined by digital radiography (DR) and computed tomography (CT). Three radiologists, each with more than 10 years experience in musculoskeletal imaging, independently evaluated the image quality using 5-grade scores, based on the metal artifacts, delineation of the prosthesis, and delineation of the peri-prosthesis structures. They then counted the detected lesions on different images based on MR findings, needle aspiration biopsy, and pathology findings.Results
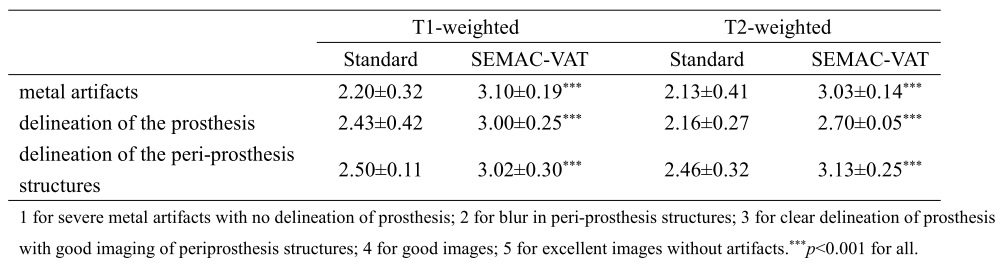
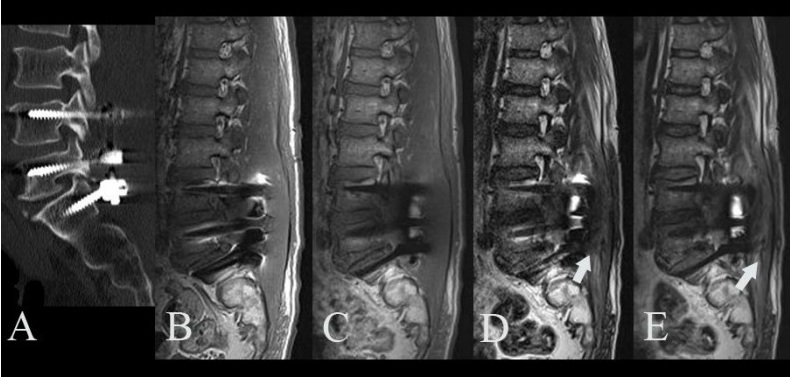
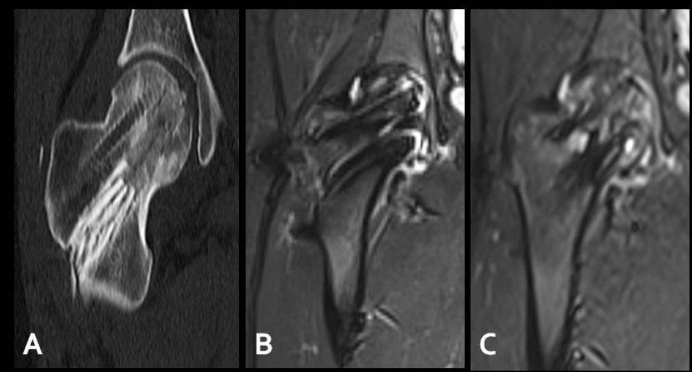
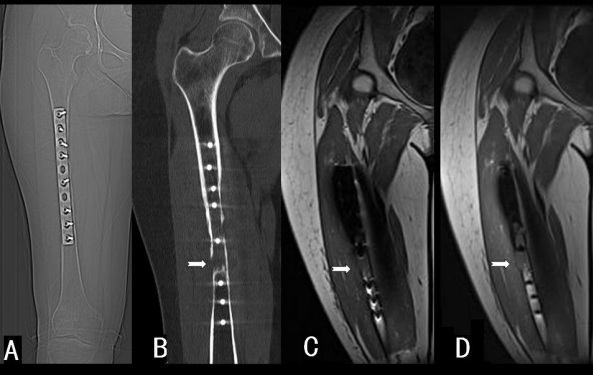
Compared with standard TSE images, visualization of all peri-prosthetic anatomic structures were significantly improved in SEMAC-VAT TSE (p<0.01) (Table 1). Figure 1 shows a case of a patient with reported back pain one week after spinal surgery. The hyperintense regions surrounding the implant were metal-induced artifacts. They were largely suppressed in SEMAC-VAT TSE images, allowing the edema surrounding the screws to be visualized (arrow). Figure 2 shows a case of a patient with a history of fracture in the neck of the femur. Femoral head necrosis was confirmed on SEMAC-VAT TSE images, but was not visible in standard TSE images. Figure 3 shows a patient with recurring tumor around the metal implant in the middle femur. The tumor was visible on SEMAC-VAT TSE images, but was missed on standard TSE imaging due to metal-induced artifact. 17 out of the 19 SEMAC-VAT TSE scans accurately demonstrated lesions (detection rate=89.5%), including eight with local infection and surrounding edema, six with femoral head necrosis, and three with recurring tumors. For postoperative infection with edema in soft tissue, the detection rate using DR was 37.5% (n=3), CT or standard TSE was 62.5% (n=5), and SEMAC-VAT TSE was 100% (n=8). For femoral head necrosis, there were eight suspected cases revealed by DR and one by CT. However, two suspected cases were false positives using these two methods. They were both excluded by SEMAC-VAT TSE, while standard TSE missed one. For recurring tumors, only MR successfully revealed the lesions, two revealed by standard TSE and three by SEMAC-VAT TSE.Discussion
TSE imaging with SEMAC-VAT technique not only reduced metal-induced artifacts, but also improved the diagnostic sensitivity in postoperative patients. The diagnosis rate of the local lesion was higher in SEMAC-VAT TSE than in standard TSE, DR and CT. However, the acquisition time was significantly longer in SEMAC-VAT than in standard TSE (T1w, 1min 6s; T1w- SEMAC-VAT, 5mins 18s; T2w, 1mins 17s; T2w- SEMAC-VAT, 8mins 12s).Conclusion
This study demonstrated that SEMAC-VAT provides a higher clinical diagnosis rate than standard TSE, DR and CT in routine musculoskeletal postoperative examination for patients reporting discomfort near the operation site. Future advances in MR technique to reduce scan time, such as through compressed sensing, will benefit the use of SEMAC-VAT in clinical practice.Acknowledgements
No acknowledgement found.References
1.Ai T, Padua A, Goemer F, et al. SEMAC-VAT and MSVAT-SPACE sequence strategies for metal artifact reduction in 1.5T magnetic resonance imaging. Invest Radiol. 47(5): 267-76 2012.
2. Friedrich B, Wostrack M, Ringel F, et al. Novel Metal Artifact Reduction Techniques with Use of Slice-Encoding Metal Artifact Correction and View-Angle Tilting MR Imaging for Improved Visualization of Brain Tissue near Intracranial Aneurysm Clips. Clin Neuroradiol. 26(1):31-7 2014.
3. Shun Qi, Wu AG,Mu YF, et al. SEMAC-VAT MR Imaging Unravels Peri-instrumentation Lesions in Patients With Attendant Symptoms After Spinal Surgery. Medicine. 95(14):e3184 2016
Figures