5085
Slipped Capital Femoral Epiphysis Causes Early Cartilage Degeneration in Young Adults – an 11 year follow-up study with dGEMRIC1Dept of Orthopedics, Skane University Hospital, Lund, Sweden, 2Dept. of Translational Medicine, Lund University, Malmö, Sweden, 3Dept. of Medical Imaging and Physiology, Skane University Hospital, Lund, Sweden
Synopsis
The longitudinal effects of Slipped Capital Femoral Epiphysis (SCFE) on hip cartilage integrity and hip function are poorly understood. In this study, 44 hips were evaluated with delayed Gadolinium-enhanced MRI of cartilage (dGEMRIC) in average 11 years after SCFE. A low dGEMRIC index was detected in SCFE hips compared to unaffected hips, with gradually lower dGEMRIC index anteriorly in the hip joint. Furthermore, a low dGEMRIC index correlated both with impaired hip function and femuroacetabular impingement (FAI), which further strengthens the theory of FAI as a mediator of osteoarthritis after SCFE.
Purpose
Slipped capital femoral epiphysis (SCFE) is the most common hip disorder in adolescent children.1 In a long-term perspective, SCFE has been associated with an increased risk of osteoarthritis (OA).2 Femuroacetabular impingement (FAI) has been suggested as a risk factor for OA development, although longitudinal studies are lacking to support this contention.3 Delayed gadolinium-enhanced magnetic resonance imaging of cartilage (dGEMRIC) is probably the most validated imaging technique to evaluate cartilage quality, in particular the glycosaminoglycan (GAG) content.4 The main purpose of the present study was to assess the status of hip joint cartilage in very young adults who had been treated for SCFE in childhood. We also wanted to investigate whether radiographic signs of FAI and clinical parameters correlate with measures of cartilage quality.Methods
We investigated 22 young adults (44 hips) (mean age 24 years, range 18-27) treated for SCFE in southern Sweden between 2001 and 2009. All subjects had been treated by in-situ pinning with the Hansson hook pin5 (mean slip angle: 36º, range 9-62). Subsequent removal of the pin was necessary in order to be eligible for MRI. All subjects were examined using a 1.5 T MR system (Siemens Magnetom AvantoFit, Erlangen, Germany). dGEMRIC was performed after an I.V. injection of double dose Magnevist® (Gd-DTPA2-, 0.4 ml/kg) using a 3D variable flip angle (VFA) method for T1 quantification (Flip angles 5 and 30 degrees). Slice thickness 3mm, pixel size 0.6 x 0.6 mm2. dGEMRIC indices were obtained in nine different regions. Three coronal slices in the femoral head with 9 mm intervals were analyzed: anterior, central and posterior. Each slice was then divided in three regions of interest (ROI): lateral, central and medial (Fig 1). ROI measurements and dGEMRIC index analysis were made using the software Medmap (Spectronic medical AB). Total dGEMRIC index was measured as the mean of the nine ROIs. For FAI evaluation, the alpha angle6 was measured in diagnostic images. Data of BMI and original slip severity were collected. A questionnaire of patient reported hip function outcome (HAGOS)7 was answered by all patients. Student’s t-test and correlation coefficient was used for the statistical analyses.Results
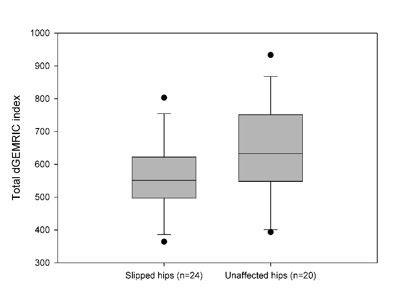
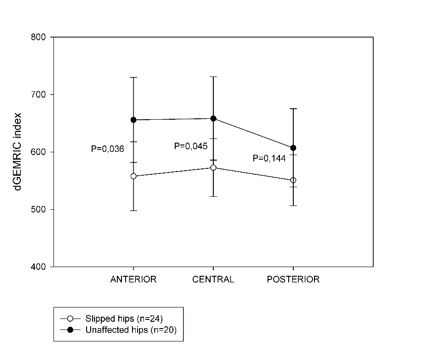
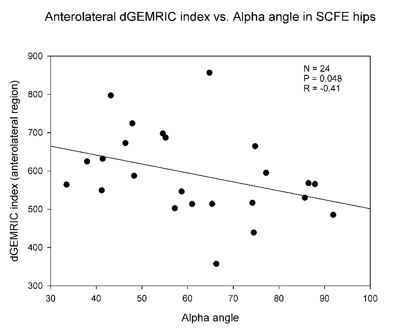
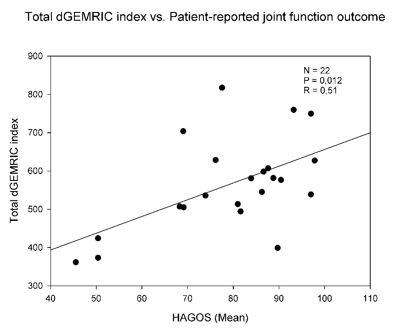
13 males and 9 females were examined. The mean interval from surgery to follow-up was 10.7 years (range 7-15 years). Two patients had bilateral SCFE. Mean BMI was 30.0 kg/m2 (range 22.4-45.6). The alpha angle was higher in slipped (n=24) compared to contralateral (n=20) hips, 61.5 º (CI 53.9-69.1) vs 45.6 º (CI 43.6-47.6), P<0.001. The total dGEMRIC index was lower in SCFE hips compared to unaffected hips, 560 ms (CI 512-608) vs. 640 ms (CI 572-706), P=0,05 (Fig 2). In hips with SCFE, the dGEMRIC index tended to decrease gradually from the posterior to anterior regions (Fig 3). The alpha angle correlated negatively with the total dGEMRIC index in all hips (P = 0.03, R=-0.31) and with the anterolateral cartilage regions in slipped hips (P=0.048, R=-0.41) (Fig 4). The clinical evaluation (HAGOS) correlated with the dGEMRIC-index (P=0.001). No statistically significant correlation could be revealed between the dGEMRIC index and BMI, original slip severity or gender.Discussion
Our findings confirm an increased risk of persistent FAI after SCFE. More interestingly, the negative correlation between the alpha-angle and dGEMRIC supports that FAI is a risk factor for future OA, and that this is detectable already in the early 20’s! Our data indicates that the cartilage degeneration caused by FAI starts in the anterior aspect of the joint where the anterior part of the femoral head-neck junction abuts against the acetabular rim. Furthermore, the correlation between the dGEMRIC index and the HAGOS clinical score indicates that early cartilage degeneration also leads to impaired hip function. This suggests that FAI should be monitored actively and treated early after skeletal maturity. However, we could not confirm any correlation between early cartilage degeneration and other potential risk factors for OA, such as slip severity, BMI or gender.Conclusion
Already one decade after SCFE, cartilage degeneration can be visualized by dGEMRIC. The early degenerative changes are related both to impaired hip function and FAI. dGEMRIC is a sensitive method to evaluate the impact of SCFE and FAI in adults.Acknowledgements
No acknowledgement found.References
1. Hansson LI, Hagglund G, Ordeberg G. Slipped capital femoral epiphysis in southern Sweden 1910-1982. Acta orthopaedica Scandinavica Supplementum 1987; 226: 1-67.
2. Carney BT, Weinstein SL, Noble J. Long-term follow-up of slipped capital femoral epiphysis. The Journal of bone and joint surgery American volume 1991; 73(5): 667-74.
3. Hosalkar HS, Pandya NK, Bomar JD, Wenger DR. Hip impingement in slipped capital femoral epiphysis: a changing perspective. Journal of children's orthopaedics 2012; 6(3): 161-72.
4. Tiderius CJ, Jessel R, Kim YJ, Burstein D. Hip dGEMRIC in asymptomatic volunteers and patients with early osteoarthritis: the influence of timing after contrast injection. Magnetic resonance in medicine 2007; 57(4): 803-5.
5. Hansson LI. Osteosynthesis with the hook-pin in slipped capital femoral epiphysis. Acta orthopaedica Scandinavica 1982; 53(1): 87-96.
6. Notzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, Hodler J. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. The Journal of bone and joint surgery British volume 2002; 84(4): 556-60.
7. Thorborg K, Holmich P, Christensen R, Petersen J, Roos EM. The Copenhagen Hip and Groin Outcome Score (HAGOS): development and validation according to the COSMIN checklist. British journal of sports medicine 2011; 45(6): 478-91.
Figures