5069
Muscle Change Associated with Time in Intensive Care Unit (ICU)1Clinical Research Imaging Centre, The University of Edinburgh, Edinburgh, United Kingdom, 2MRC Centre for Inflammation Research, The University of Edinburgh, Edinburgh, United Kingdom, 3Anaesthesia, Critical Care and Pain Medicine, The University of Edinburgh, Edinburgh, United Kingdom, 4The Mentholatum Company Ltd., East Kilbride, United Kingdom
Synopsis
Muscle wasting is common during critical illness. In this study, thigh muscles of previously mobile patients surviving an episode of severe critical illness were imaged by Magnetic Resonance Imaging (MRI) during convalescence and compared to healthy controls. We present preliminary findings of the first clinical study using Magnetic Resonance Elastography (MRE) to measure muscle stiffness (kPa) and muscle cross-sectional area (mm2) for Intensive Care Unit (ICU) patients. A statistically significant reduction in muscle area and muscle stiffness in patients was found when compared to the healthy control group. There was a significant cross-sectional muscle area increase following ICU patient discharge.
Introduction
Physical weakness after critical illness is common, long lasting and may be related to muscle wasting, a frequent occurrence during critical illness [1,2,3]. Muscle atrophy [4,5,6] and micro-structural changes [7,8,9] have been demonstrated in ICU survivors but not recovery of atrophy. Magnetic Resonance Imaging (MRI) analysis was used to measure cross-sectional area (mm2) and Magnetic Resonance Elastography (MRE) was used to measure muscle mechanical properties (kPa). MRE is a relatively new technique in which analysis of the propagation of sound waves through tissues can be used to measure the tissue stiffness. This is the first time MRE has been applied to study muscle stiffness in survivors of critical illness. We hypothesised that the quadriceps muscles of ICU survivors would be smaller (atrophied) compared to those of healthy controls, were resistant to regeneration, and that they would have impaired mechanical properties (manifested as an increase in muscle stiffness).Methods
14 healthy control subjects (24.1±4.3yrs) and 10 ICU patients (47.1±16.4yrs) were studied. MRI was performed once in the control patients. In the ICU patients, images were acquired close to the point of ICU discharge (within 10 days), and repeated 3 months later if the patient agreed to a repeat scan. Images were acquired using a 3T Siemens Verio MRI system (Siemens Medical Systems, Erlangen, Germany) equipped with a 32-channel receiver coil. A spin echo EPI sequence was used to acquire 3D multi-frequency MRE data (TE=1600ms, TR=54ms and 8 phase offsets) at four different actuation frequencies (i.e. 25, 37.5, 50 and 62.5 Hz), with an acquisition time of 1 minute 20 seconds for each frequency. Five 2mm thick contiguous transverse slices through the thigh (at one third of the thigh from the knee), each with a FOV of 224x224 mm and an image matrix of 112x112 pixels corresponding to a pixel resolution of 2x2x2mm, were studied.
MRE elastograms were computed using Elastography Software Pipeline (ESP) software developed in-house [7]. ESP produces Super Resolution pixel-by-pixel maps of the Magnitude of the Complex Modulus |G*| (i.e. stiffness) of tissues based on Multi-Frequency Dual Elastovisco Inversion (MDEV) [8].
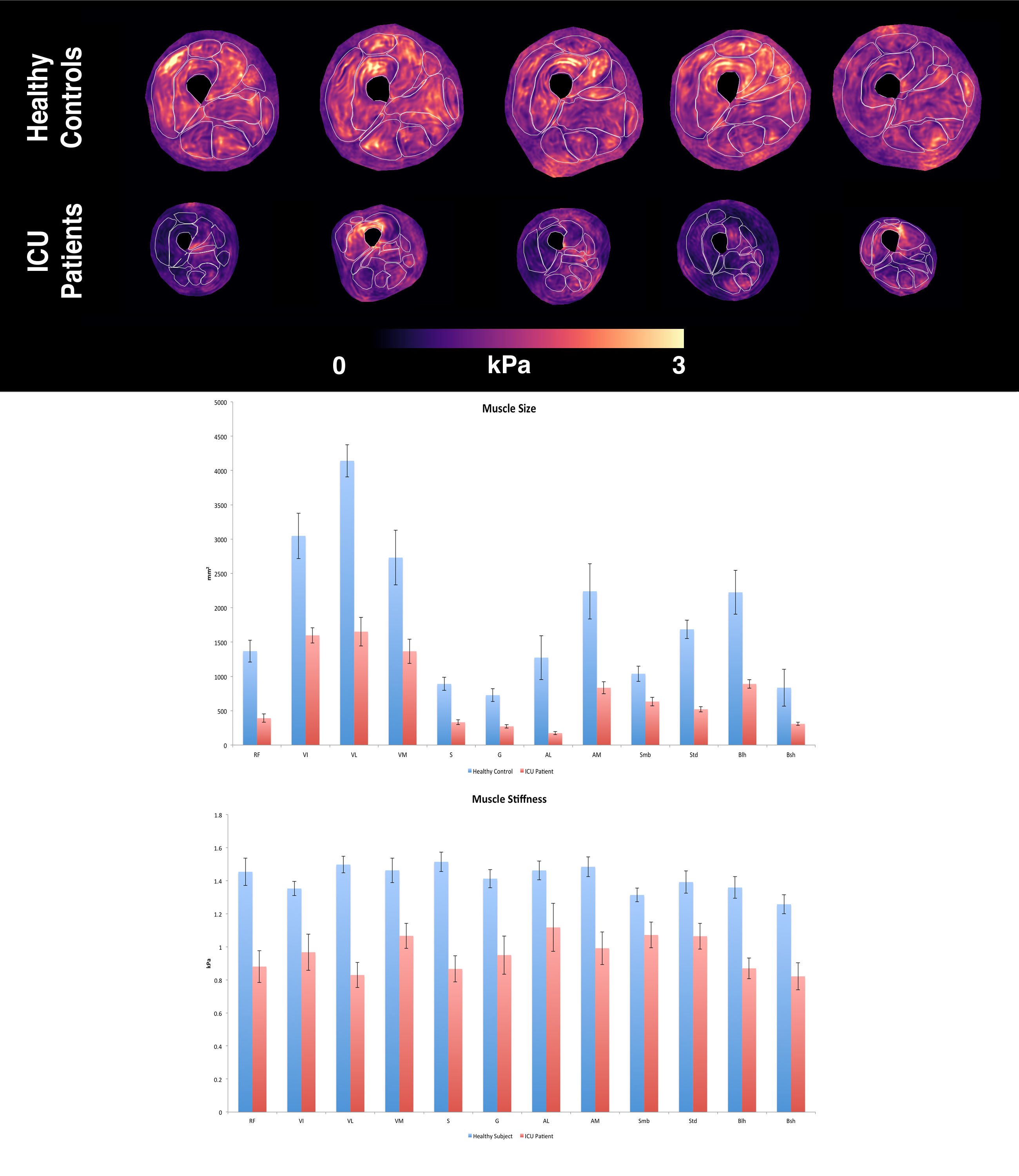
ROI’s were drawn around each muscle (n=12) in the transverse view, which were then measured to show the mean |G*| and size of the muscle. The four muscle groups that were analysed include: Quadriceps (Rectus Femoris, Vastus Lateralis, Vastus Intermedius and Vastus Medialis), Hamstrings (Semimembranosus, Semitendinosus, Bicep Long Head and Bicep Short Head), Adductors (Adductor Longus and Adductor Magnus) and also Medial muscles (Sartorius and Gracilis). Student’s T-Test was used to compare differences in |G*| between patients and controls, with a paired T-Tests between the baseline and follow-up scan in the patients.
Results
ICU patients showed an overall lower muscle cross sectional area (-60%, p<.000) with a corresponding overall lower |G*| (-32%, p<.000), when compared to healthy controls (Figure 1). The Rectus Femoris, Vastus Lateralis and Sartorius in size and stiffness between the two groups (p<.000). When the individual muscles of ICU patients were compared to the the controls, the Adductor Longus was the muscle which was most effected in size -86% (p=.006), with the Vastus Lateralis showing the greatest difference in |G*| at -43% (p>.000). The Semimembranosus showed the smallest difference in size at 39% (p=.006) and |G*| at -18% (p=.015) between the two groups.
The muscle groups that showed the largest decrease in stiffness were Medial muscles (-37%, p<0.000) and the Quadriceps (-33%, p<0.000), with the Adductor group (-28%, p<0.000) and Hamstrings showing the least change (-28%, p<0.000). However the Adductor group showed the most change in muscle size reduction (-73%, p<0.000), with the Medial group (-63%, p<0.000), Hamstrings (-57%, p<0.000) and Quadriceps (-55%, p<0.000) showing similar size changes. Overall there was a significant positive correlation between size and stiffness of muscle (r=.34, p<.000).
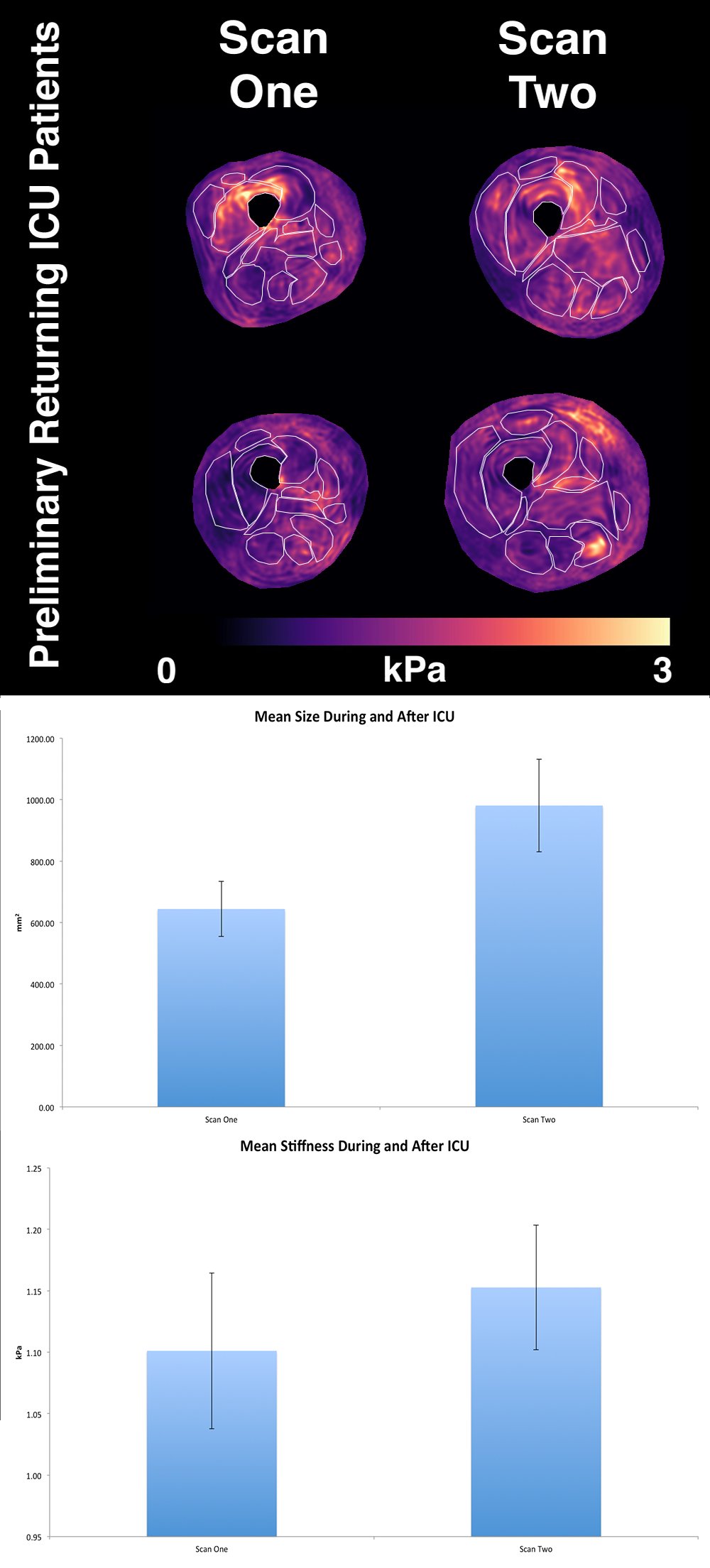
At follow-up, ICU patients (n=2) showed an increase of 52% in muscle cross-sectional area (p=.003), but only a 5% increase in |G*| (p=.407).
Discussion
This study has revealed that significant decreases in both the size and the stiffness of the thigh muscles occurs in patients at the ICU, with the muscle size had increased appreciably by 3 months after discharge, the decrease in |G*| persists. The Hamstrings muscle group (e.g. Semimembranosus) was the least susceptible to decreases in size and stiffness whereas the Quadriceps muscle group, and also the Sartorius muscle, were greatest affected.Conclusion
The observation that muscle stiffness remains significantly reduced despite muscle size having largely recovered three months after discharge from ICU provides important information to support the development of appropriate training programmes to help patients recover strength and performance.Acknowledgements
No acknowledgement found.References
1. Puthucheary, Z.A., Rawal, J., McPhail, M., Connolly, B., Ratnayake, G., Chan, P., Hopkinson, N.S., Padhke, R., Dew, T., Sidhu, P.S. and Velloso, C., 2013. Acute skeletal muscle wasting in critical illness. Jama, 310(15), pp.1591-1600.
2. Herridge MS. 2009. Legacy of intensive care unit-acquired weakness. Crit Care Med, 37(10), S457-61.
3. Herridge, M.S., Tansey, C.M., Matté, A., Tomlinson, G., Diaz-Granados, N., Cooper, A., Guest, C.B., Mazer, C.D., Mehta, S., Stewart, T.E. and Kudlow, P., 2011. Functional disability 5 years after acute respiratory distress syndrome. New England Journal of Medicine, 364(14), pp.1293-1304.
4. Gruther, W., Benesch, T., Zorn, C., Paternostro-Sluga, T., Quittan, M., Fialka-Moser, V., Spiss, C., Kainberger, F. and Crevenna, R., 2008. Muscle wasting in intensive care patients: ultrasound observation of the M. quadriceps femoris muscle layer. Journal of rehabilitation medicine, 40(3), pp.185-189.
5. Reid, C.L., Campbell, I.T. and Little, R.A., 2004. Muscle wasting and energy balance in critical illness. Clinical Nutrition, 23(2), pp.273-280.
6. Plank, L.D. and Hill, G.L., 2000. Similarity of changes in body composition in intensive care patients following severe sepsis or major blunt injury. Annals of the New York Academy of Sciences, 904(1), pp.592-602.
7. Helliwell, T.R., Wilkinson, A., Griffiths, R.D., McClelland, P., Palmer, T.E.A. and Bone, I.M., 1998. Muscle fibre atrophy in critically ill patients is associated with the loss of myosin filaments and the presence of lysosomal enzymes and ubiquitin. Neuropathology and applied neurobiology, 24(6), pp.507-517.
8. Griffiths, R.D., Palmer, T.E., Helliwell, T., Maclennan, P. and MacMillan, R.R., 1994. Effect of passive stretching on the wasting of muscle in the critically ill. Nutrition (Burbank, Los Angeles County, Calif.), 11(5), pp.428-432.
9. Burnham, E.L., Moss, M. and Ziegler, T.R., 2005. Myopathies in critical illness: characterization and nutritional aspects. The Journal of nutrition, 135(7), pp.1818S-1823S.
10. Barnhill, E., Hollis, L., Sack, I., Braun, J., Hoskins, P.R., Pankaj, P., Brown, C., van Beek, E.J. and Roberts, N., 2016. Nonlinear Multiscale Regularisation in MR Elastography: Towards Fine Feature Mapping. Medical Image Analysis.
11. Papazoglou, S., Rump, J., Braun, J. and Sack, I., 2006. Shear wave group velocity inversion in MR elastography of human skeletal muscle. Magnetic resonance in medicine, 56(3), pp.489-497.
Figures