5042
Imaging inferior alveolar neurovascular bundle using zero echo time magnetic resonance imaging1Department of Radiology, Liaocheng People’s Hospital, Shandong University, Liaocheng, People's Republic of China, 2Department of Radiology, Shandong Medical imaging research institute, 3Liaocheng People’s Hospital, Shandong University, 4Liaocheng People's Hospital, Shandong University
Synopsis
The goal of the present study was to evaluate ZTE acquisitions for the inferior alveolar neurovascular bundle (IANB) identification. For this purpose, 15 volunteers were scanned using a standard 3D ZTE sequence with a voxel size of 0.8×0.8×0.8 mm on a 3 Tesla MR unit. Both subjective and objective analyses were performed on all acquired IANB images. The results indicate that ZTE-MRI is feasible for the IANB imaging without the use of contrast material.
Objectives
Objectives: It is important to identify the inferior alveolar neurovascular bundle (IANB) before surgical procedures involving the mandible in order to avoid intraoperative complications. However, though has great clinical implications, IANB imaging is impossible with ultrasound or X-ray based imaging modalities because it courses through the bony mandibular canal. Magnetic resonance imaging (MRI) with conventional fast spin echo or gradient echo sequences is also limited in clinical practice due to low spatial resolution, long acquisition time or contrast administration. The aim of this study was to investigate whether non-contrast-enhanced zero echo time (ZTE) magnetic resonance imaging (MRI) is appropriate for imaging of the IANB.Methods
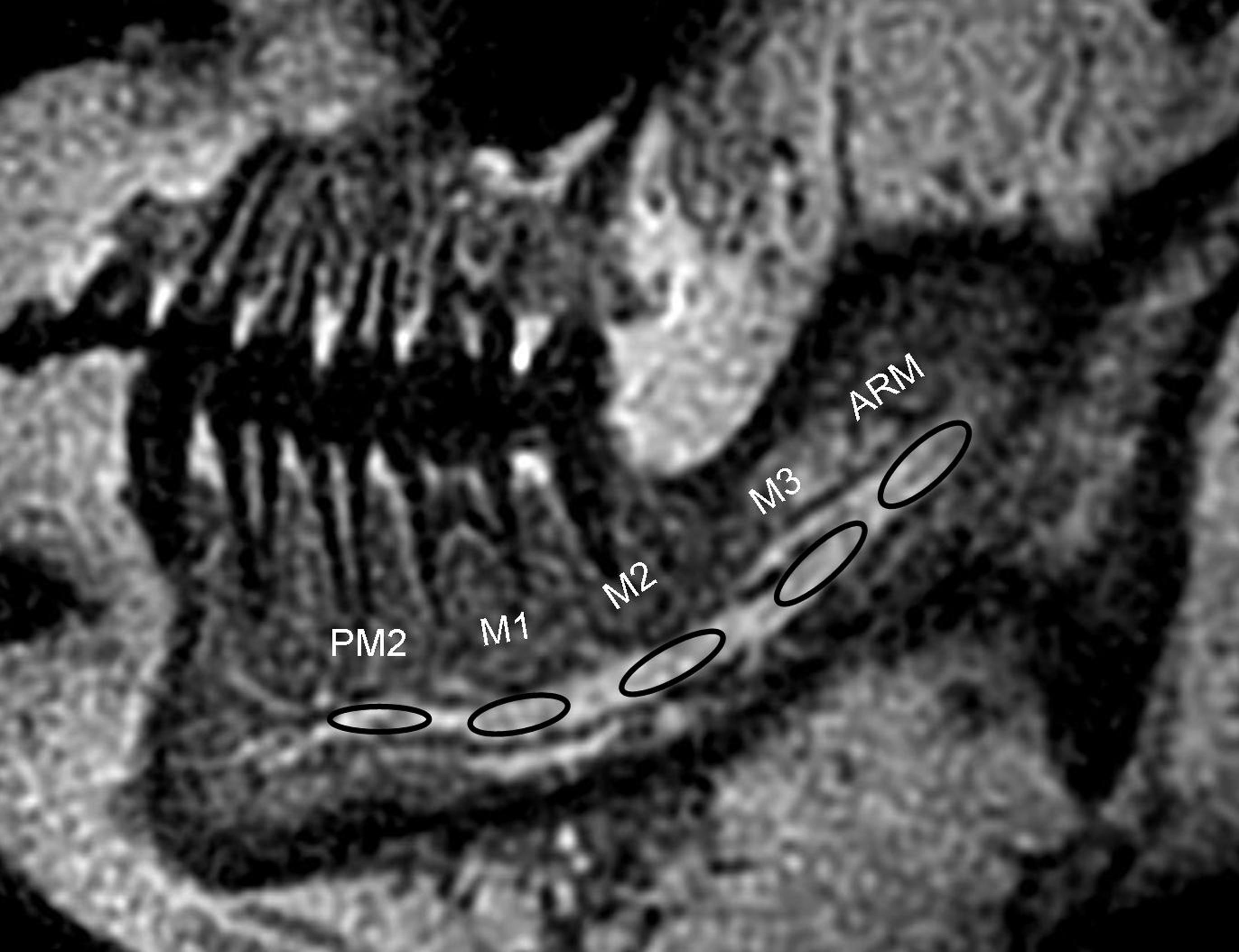
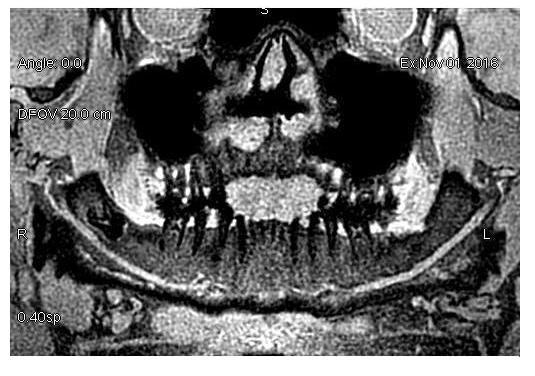
Methods: Fifteen volunteers (mean age 37.8 ± 3.8 years, range, 22 to 64 years old, 9 men/6 women) were scanned using a three-dimensional ZTE sequence with a voxel size of 0.8×0.8×0.8mm on a 3 Tesla MR unit ( Silenz; GE Healthcare). The exclusion criteria were considered as the presence of any pathology (cyst, tumor or periapical lesion), fracture or metallic implant in oral and maxillofacial regions. The parameters for acquisition in the ZTE-MRI were as follows: TE, 0 ms; flip angle, 5°; FOV, 180×180 mm; spokes per segment, 384; total number of spokes, 196608; NEX, 1.5; bandwidth, ±20 kHz; and acquisition time, 3minutes 36 seconds. Cross-sectional and panoramic reconstructions of the whole mandible were performed from the sagittal scans on the dedicated MR workstation (AW4.6, GE Healthcare). Image quality was rated on a 4-point ordinal scale (4=excellent, 3=good, 2=moderate and 1=non-diagnostic) by two independent experienced radiologists unaware of patient information and scan parameters. Signal intensities in the IANB and perineurovascular bone tissue at both side of the ascending ramus of the mandible, first, second and third molars and second premolar were measured in the multiplanar reconstruction images. Signal-to-noise ratios (SNRs) and Contrast-to-noise ratios (CNRs) were calculated. Interobserver agreements of image quality assessment per IANB were examined with κ statistics. Comparisons of SNR and CNR between the right and left INAVs were performed using paired t-tests.Results
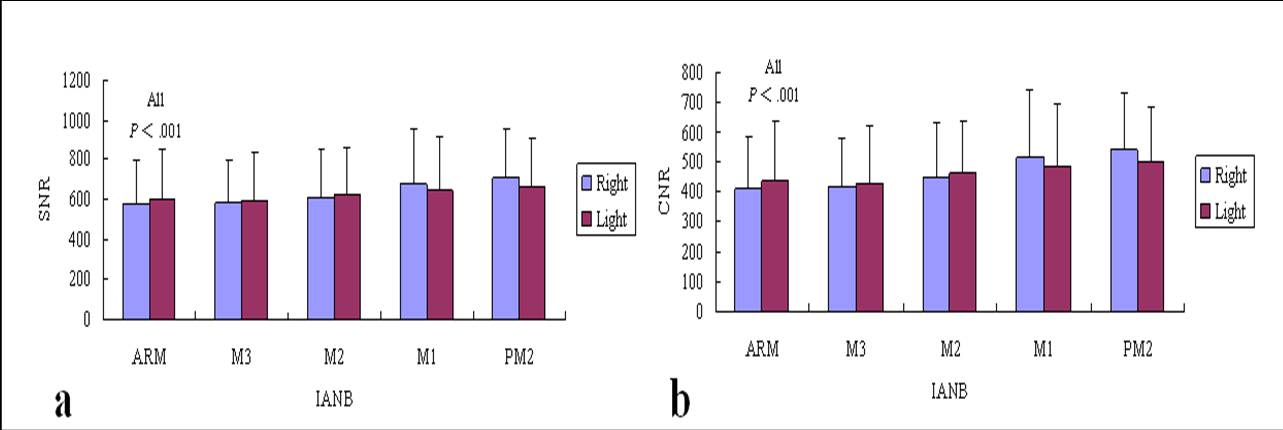
Results: All MR examinations were successfully performed in all individuals within four minutes. Image quality was rated as excellent in 63.3% (19/30) and good in 26.7% (8/30) of IANBs. Moderate image quality was present in 3 of 30 IANBs (10.0%) due to motion artifact induced by swallowing. There were excellent interobserver agreements (κ = 0.86) in grading the image quality. ZTE MRI produced high SNRs and CNRs in all INAB segments, with a mean SNR value of 629.17 ± 234.98 (range, 984.20 to 288.71) and a mean CNR value of 464.90 ± 178.89 (range, 726.86 to 185.18) in right INAB, and a mean SNR value of 624.88 ± 239.83 (range, 1010.60 to 248.71) and a mean CNR value of 460.60 ± 184.59 (range, 703.60 to 145.18) in left INAB, respectively. There were no significant differences in SNR and CNR values between right and left side INABs (p < .001).Conclusion
Conclusion: ZTE-MRI is a 3D high resolution imaging modality and possesses excellent soft and hard tissue contrast. It’s feasible for depiction of INAB without the use of contrast material in a short examination period.Acknowledgements
The authors wish to give special thanks to Yanyan Tang, Shuhua Li for contributions to the manuscript and Fengzhen Liu for statistical advice.References
1. Wiesinger F, Sacolick LI, Menini A, et al. Zero TE MR bone imaging in the head. Magn Reson Med. 2016;75(1):107-114.
2. Hövener JB, Zwick S, Leupold J, et al. Dental MRI: imaging of soft and solid components without ionizing radiation. J Magn Reson Imaging. 2012;36(4):841-846.
3. Chau A. Comparison between the use of magnetic resonance imaging and cone beam computed tomography for mandibular nerve identification. Clin Oral Implants Res. 2012;23:253–256.
Figures