5029
Musculoskeletal imaging of the extremities with a compact 3T MRI with high-performance gradients1Radiology, Mayo Clinic, Rochester, MN, United States, 2GE Healthcare, 3MRI, GE Global Research, Niskayuna, NY, United States
Synopsis
A compact, low-cryogen 3T MRI system with high-performance gradients has been developed and tested on healthy volunteers. This compact 3T MRI unit has the potential to dramatically impact MRI by offering simplified siting and strong gradient performance at lower cost. In addition to brain and pediatric imaging, the scanner offers an ideal platform for musculoskeletal (MSK) imaging of the extremities.
Purpose
Clinical demand continues to increase for high quality extremity MRI for evaluation of sports related athletic injuries and age-related degenerative changes. At the same time, there are several important limitations to incremental growth of MRI access, including difficulty obtaining liquid helium and costly siting of standard MRI units. The purpose of this study is to demonstrate the compact 3T scanner’s capability as an extremity MSK scanner for knee and wrist imaging.Methods
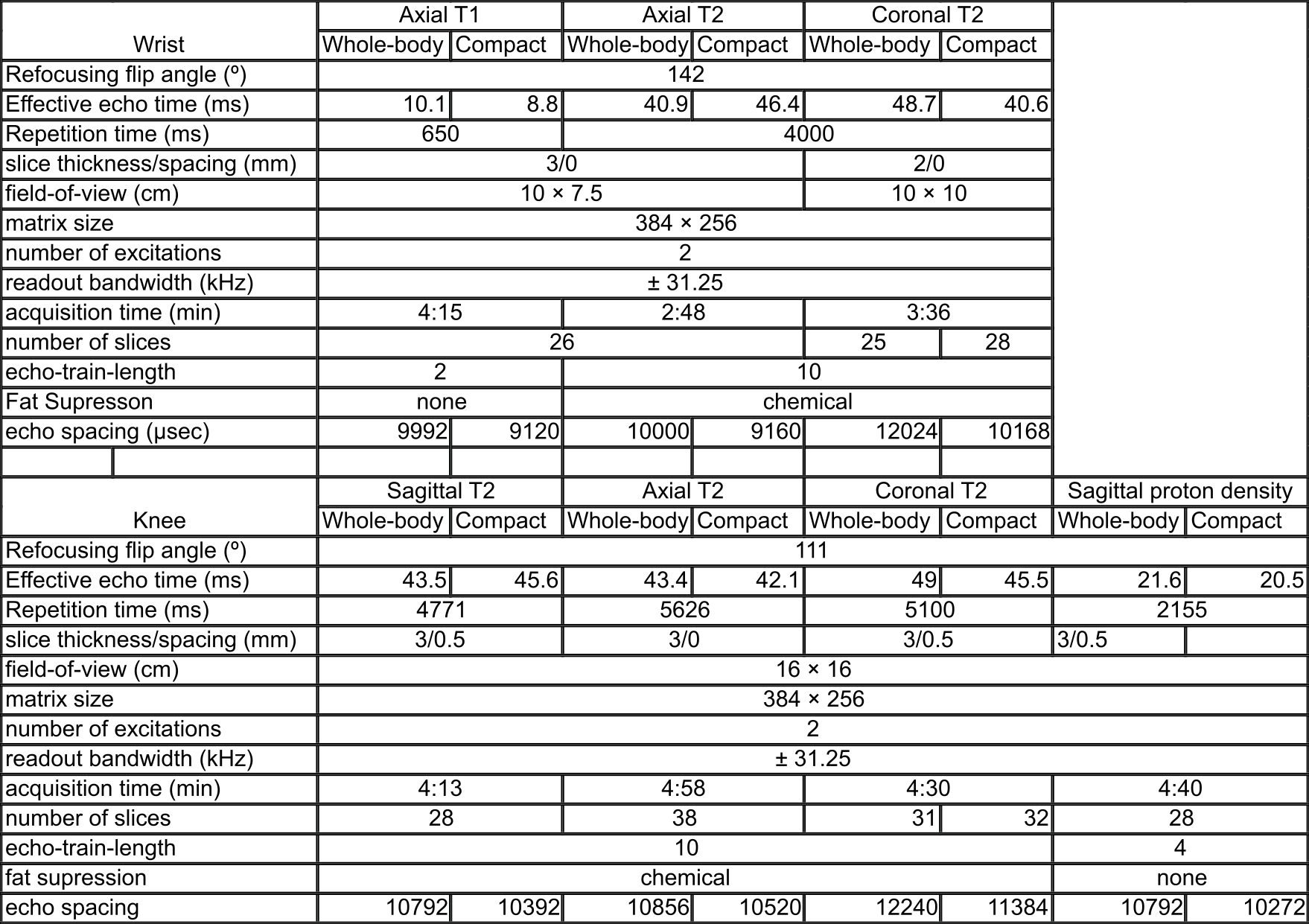
A compact 3T MRI scanner (GE Global Research Center, Niskayuna, NY) with an 37 cm bore diameter asymmetric gradient system capable of 80 mT/m and 700 T/m/s has been developed[1–3]. With IRB approval, healthy volunteers were scanned using a 16-channel, large flex coil using our standard protocol on a 3T MRI scanner (750 GE Healthcare, Waukesha, WI) and the compact 3T scanner. The compact 3T used real-time gradient pre-emphasis[4] and frequency shifting to compensate additional concomitant fields All images were graded independently by a fellowship trained MSK radiologist with 12 years of experience and a MSK radiology fellow. Images were compared in a blinded fashion for sharpness, artifact and contrast for the following anatomic features in the wrist ( extensor tendons, median nerve in carpal tunnel, articular cartilage of the pisotriquetral joint, cortical margins of the distal radio-ulnar joint, flexor tendons, triangular fibrocartilage, scapholunate ligament, and 1st carpometacarpal joint) and knee ( menisci, articular cartilage, patellar cartilage, medial patellar retinaculum, trochlear cortical margin, medial collateral ligament, patellar tendon). Acquisition times were normalized, and when necessary, the repetition time (TR) of the compact 3T was extended artificially to ensure the whole-body system could cover the same slice prescription with identical TR even though the echo spacing with the compact 3T was reduced. Imaging was performed using sequence parameters detailed in Table 1. All radiologic grading was pooled within anatomic region scanned, and compared with the one-sided Wilcoxon signed rank test.Results
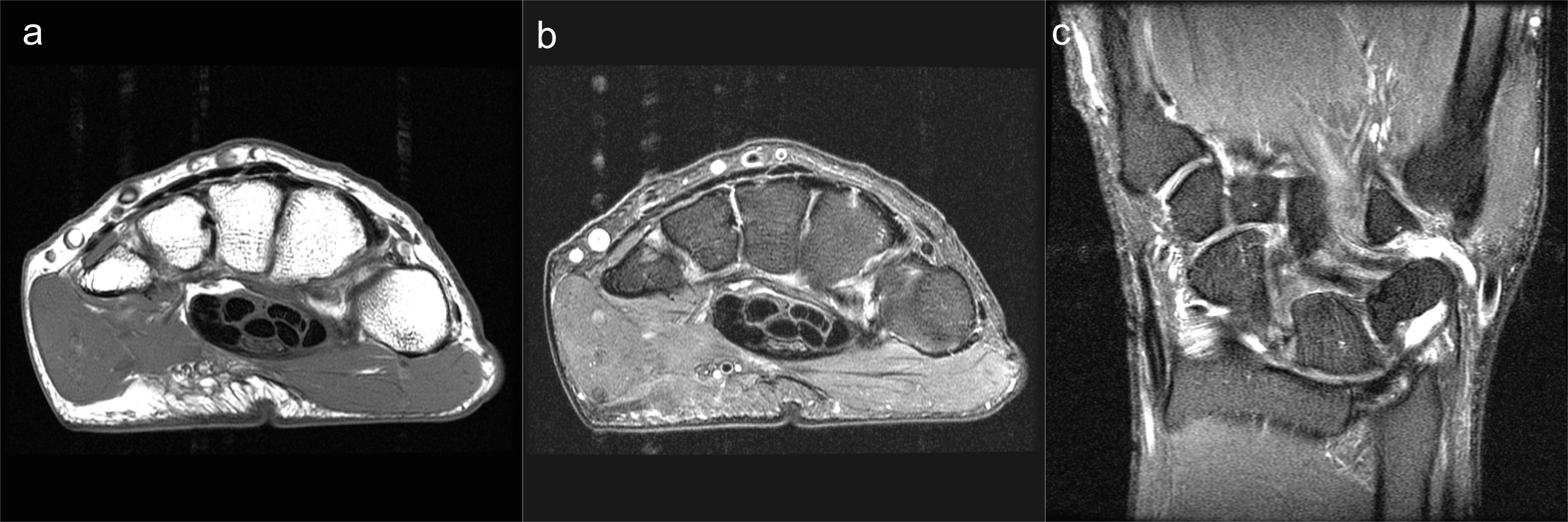
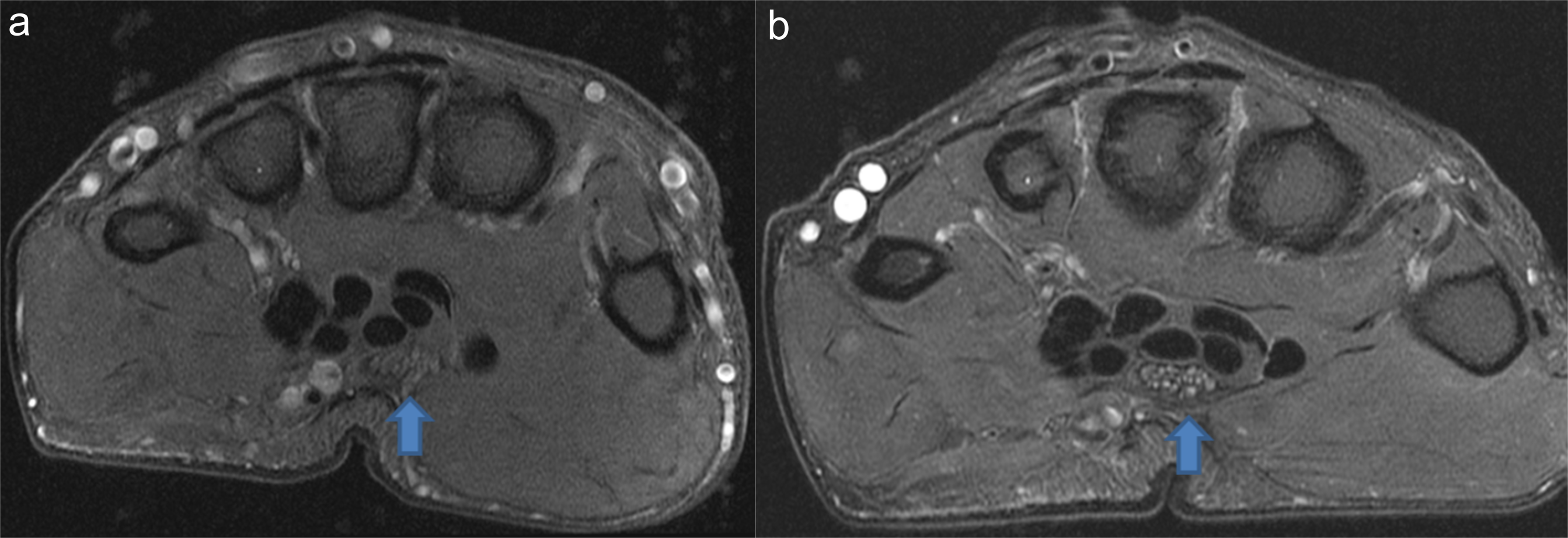
Volunteer scans with high-performance gradients demonstrated excellent image quality across the spectrum of T1, proton density and fat-suppressed T2-weighted fast spin echo (FSE) sequences for the knee, and T1 and T2 weighted sequences for the wrist. Wrist images from the compact system are shown in Figure 1, and knee images shown in Figure 2. Wrist imaging was statistically determined to be equivalent or better (p < 0.05) between the compact and whole-body systems, but no statistical significance was achieved for knee imaging. Figure 3 illustrates an image quality improvement between the two scanners for the wrist, with the compact system image showing increased conspicuity of the individual median nerve fascicles. The volunteer reported similar levels of comfort in each scanner for each exam.Discussion/Conclusion:
This compact, high-performance 3T MRI system is shown to generate images of the wrist of equal or superior quality to those obtained on a conventional 3T MRI. This may be attributed to the increased gradient performance which results in decreased echo spacing in the FSE sequence resulting in increased signal-to-noise ratio. These initial results are not unexpected, since small-FoV imaging such as that of the wrist, especially benefits from the increased gradient performance (80 mT/m, 700 T/m/s on the compact 3T, versus 50 mT/m, 200 T/m/s on the whole body system). The absence of proton density wrist images reflects the usual clinical protocol. Further comparison studies are needed to determine the significance of this difference for MSK imaging in particular, and will be undertaken.Acknowledgements
This work was supported in part by NIH grant RO1EB010065.References
[1] Weavers PT, Shu Y, Tao S, Huston J, Lee S-K, Graziani D, et al. Technical Note: Compact three-tesla magnetic resonance imager with high-performance gradients passes ACR image quality and acoustic noise tests. Med Phys 2016;43:1259–64. doi:10.1118/1.4941362.
[2] Foo TKF, Tan ET, Schenck JF, Graziani D, Laskaris E, Vermilyea M, et al. Novel High Performance, Compact 3.0T MRI System for Imaging the Brain. Mil. Heal. Syst. Res. Symp., Orlando: 2016.
[3] Lee S-K, Mathieu J-B, Graziani D, Piel J, Budesheim E, Fiveland E, et al. Peripheral nerve stimulation characteristics of an asymmetric head-only gradient coil compatible with a high-channel-count receiver array. Magn Reson Med 2015:n/a-n/a. doi:10.1002/mrm.26044.
[4] Tao S, Weavers PT, Trzasko JD, Shu Y, Huston J, Lee S, et al. Gradient pre-emphasis to counteract first-order concomitant fields on asymmetric MRI gradient systems. Magn Reson Med 2016;0. doi:10.1002/mrm.26315.
Figures