5027
Improvement of 3D diffusion-prepared MR neurography in the extremities using improved diffusion-sensitized driven-equilibrium (iDSDE) with phase-cycling turbo field echo sequenceTakayuki Sakai1, Masami Yoneyama2, Atsuya Watanabe1, Iain Ball3, Toshiaki Miyati4, and Noriyuki Yanagawa1
1Eastern Chiba Medical Center, Chiba, Japan, 2Philips Electronics Japan, Tokyo, Japan, 3Philips Electronics Australia, North Ryde, Australia, 4Kanazawa University, Ishikawa, Japan
Synopsis
Diffusion-sensitized driven-equilibrium with phase-cycling T1-turbo field-echo (pc-DSDE) enables the visualization of peripheral nerves. However, pc-DSDE has several problems, such as low image stability, poor reproducibility, and partially remaining venous signals. To solve these problems, we improved DSDE pre-pulse module (iDSDE) including B1-insensitive RF pulse and orthogonally combined motion- and diffusion-sensitized gradient scheme. iDSDE showed better visualization of peripheral nerves without contamination of veins.
PURPOSE
The role of MRI in diagnosis of peripheral neuropathy is depiction of the anatomical detail of peripheral nerves and the pathological changes related to entrapment. As a preliminary, we have developed phase-cycling T1-turbo field-echo (TFE)1,2 combined with diffusion-sensitized driven equilibrium3 (pc-DSDE) that enables the visualization of peripheral nerves4 (Fig. 1). However, pc-DSDE has several limitations, such as low image stability, poor reproducibility, and partially remaining venous signals (Fig. 2). To solve these limitations, we propose a new scheme, called improved diffusion-sensitized driven-equilibrium (iDSDE). The purpose of this study was to evaluate the visualization of peripheral nerves by iDSDE in the extremities such as wrist, elbow, and knee.METHODS
Theory and pulse sequence: iDSDE includes the two improvement strategies. First, to improve the pulse efficiency in the off-center FOVs, B1-insensitive adiabatic pulses for both excitation/flipback and refocusing are applied. Second, to effectively suppress the veins while preventing signal loss of nerves which are running parallel to veins, orthogonally combined motion- and diffusion-sensitized gradient scheme proposed by Cervantes5 is adopted (optimized gradient type)(Fig.3). Expeiments: All subjects were examined using a 1.5 T whole-body clinical system and an eight-channel coil (Ingenia, Philips Healthcare). The study was approved by the local IRB, and written informed consent was obtained from all subjects. Five healthy volunteers were included for the examination of peripheral nerves in the extremities. To demonstrate the effect of iDSDE improvement strategies, we compared the two types of RF pulses and three types of motion-sensitized gradient types (unipolar, bipolar and optimized gradient type). We assessed the detectability of peripheral nerves to measure contrast-ratio (CR) among the nerves and background muscle signals, and to examine using subjective visual evaluation method by three trained radiologists. Imaging parameters were; Coronal, voxel size=1.88×1.88×1.6mm3, b-value=910s/mm2, DSDE preparation time=100ms, gradient strength phase/freq/slice=20/5/20mT/m, shot interval=2800ms, flip angle=8°, turbo factor=60, ProSet 1331, and total acquisition time=5m09s.RESULTS AND DISCUSSION
iDSDE clearly depicted the course of peripheral nerves on the MIP images. Image uniformity of iDSDE was improved, because B1-insensitive pulses were applied to improve the RF pulse efficiency in the off-center FOV. Contrast ratio of iDSDE was no different from that of current pc-DSDE. Regional venous signal was effectively suppressed by the use of B1 insensitive pulse on subjective visual evaluation (Fig. 4). Contrast ratio was no significant difference in the MPG gradient types. However, relative ranking score of optimized gradient type on subjective visual evaluation was significantly higher than those of other gradient types (Fig. 5). Because venous signals were well suppressed with optimized gradient type. The unipolar gradient type showed high nerve signals and effective background signal suppression, but venous signal was still remained. The bipolar gradient type indicated effective venous signal suppression, but overall image quality was low compared to others. The optimized gradient type, which applies weak bipolar gradient in the direction parallel to the major nerves (and vessels) and strong unipolar gradients in the direction perpendicular to those objects, showed better visualization without contamination of veins.CONCLUSION
MR neurography using iDSDE enables improved visualization of peripheral nerves with more insensitive to inhomogeneous and more suppression of venous signal than those of pc-DSDE in the extremities. Further clinical investigation is needed.Acknowledgements
No acknowledgement found.References
[1] Coremans, J Magn Reson 1997;124:323–42;
[2] Thomas, Magn Reson Med 1998;39:950–60;
[3] Obara, Proc. ISMRM 2011:4023;
[4] Yoneyama, Proc. ISMRM 2015: 0313;
[5] Cervantes, Proc. ISMRM 2015: 0101.
Figures
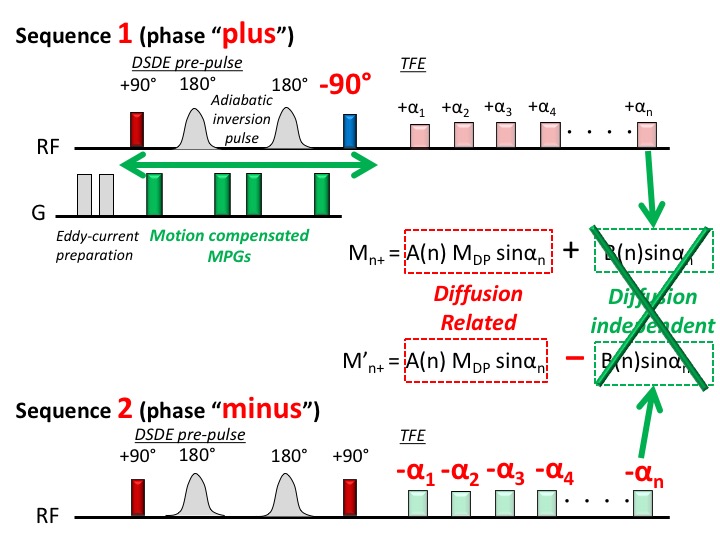
Fig. 1
Scheme of pc-DSDE T1-TFE sequence.
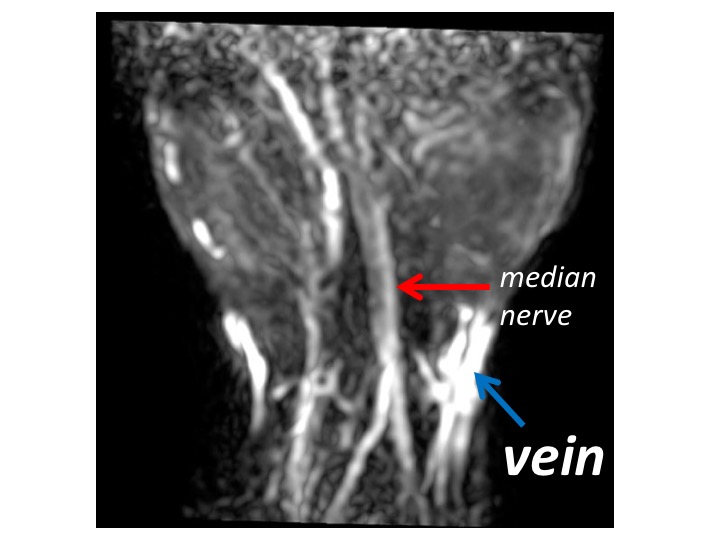
Fig. 2 Current
limitations of pc-DSDE (Low image robustness and poor reproducibility, Remained
reginal venous signal)
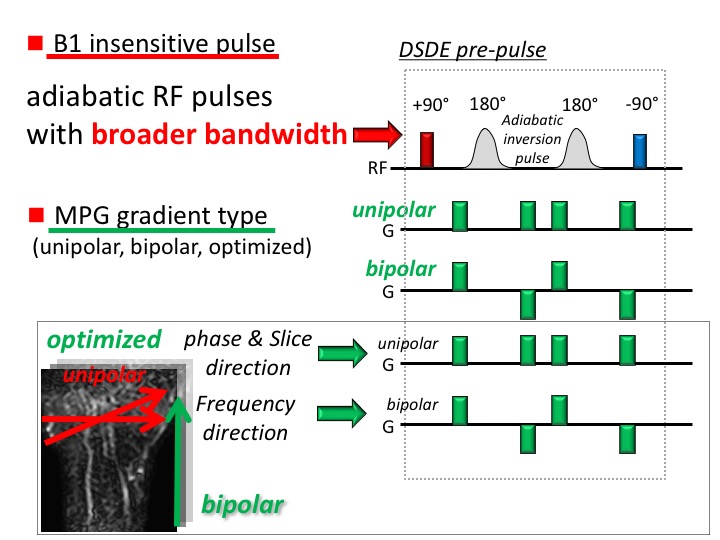
Fig. 3
Improvements of iDSDE pre-pulse

Fig. 4
Effect of B1-insensitive pulse
on subjective visual evaluation (Regional venous signal was effectively
suppressed by the use of B1-insensitive pulse with an optimized gradient type)
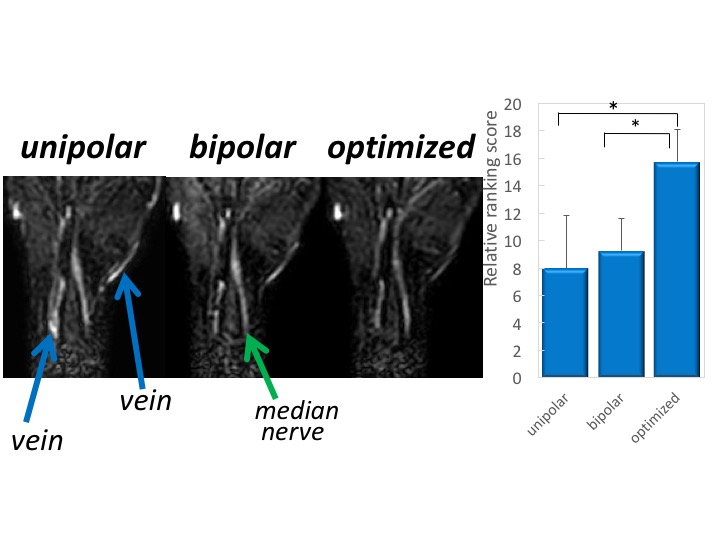
Fig. 5
Effect of MPG gradient type on
subjective visual evaluation (Venous signals were well suppressed with
optimized gradient type)