5017
Metal Artifact Reduction MRI around Cobalt-Chromium Arthroplasty Implants: The Negative Effect of Long Echo Trains on Implant-related Artifact1Radiology, Johns Hopkins Hospital, Baltimore, MD, United States, 2Radiology, Johns Hopkins Hospital
Synopsis
We demonstrate the negative effects of increasing echo train lengths on total implant-related artifact in a setting of controlled bandwidth, echo spacing and effective echo time. For the practical purpose of metal artifact reduction sequence MR imaging with use of turbo spin echo pulse sequences, high receiver bandwidth can be recommended as the first line means, whereas long echo train length may not be recommended and used cautiously due to the potential of substantial degradation of image quality.
Purpose
To quantitatively and qualitatively assess the effects of echo train length as well as bandwidth and echo spacing on MR metal artifact using a Cobalt-Chromium arthroplasty implant system.
Introduction
Sufficient reduction of susceptibility artifacts induced by metallic implants is required for optimized MR imaging evaluation of periprosthetic bone and soft tissues [1]. Factors that reduce the magnitude of metal-induced susceptibility artifacts on turbo spin echo (TSE) images include the use of 1.5 Tesla field strength, high receiver bandwidth and thin slice thickness [2]. Multiple articles additionally recommend long echo train length (ETL) to reduce metal implant-induced artifacts [3-7]. However, the effect of ETL on metal artifacts has not been proven and remains elusive.Materials and Methods
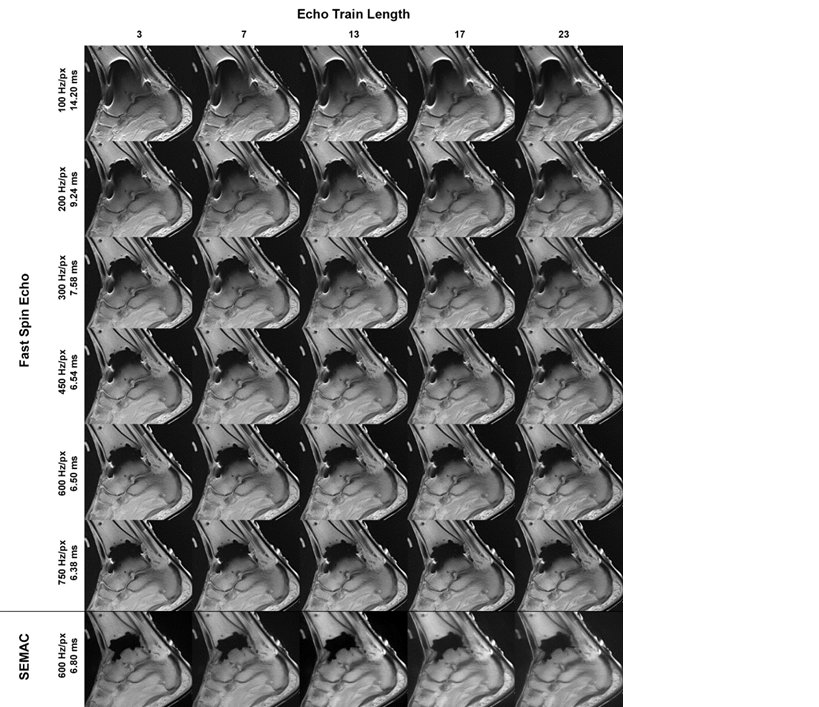
A Cobalt-Chromium based total ankle arthroplasty system was implanted into a human cadaver ankle. Using a clinical 1.5 Tesla MR imaging system, sagittally oriented, conventional 2-dimensional turbo spin echo (TSE) pulse sequences were acquired with ETL ranging from 3 to 23 as well as BW from 100 to 750 Hz/pixel and corresponding echo spacing from 6.38 to 14.2 ms. For each combination of ETL and BW/echo spacing, sequence parameters such as effective echo time and spatial resolution were controlled. A sagittally oriented, compressed-sensing TSE pulse sequence (CS-SEMAC) with 19 phase-encoding steps, BW of 600 Hertz/pixel and otherwise identical parameters was acquired with ETL ranging from 3 to 23 to isolate additional effects of increasing ETL and as the standard of reference (ETL 3) [8,9,10]. The primary endpoint variable was the total implant-related artifact area, normalized to the calcaneal area of the index slice. Secondary endpoint variables included normalized implant-related signal void areas on sagittal and coronal image reformats. Two raters evaluated the overall image quality and preference across varying BW and ETL. Two-factor-ANOVA, Friedman, and Kruskal-Wallis tests, Pearson correlation and inter-rater agreement were used. P-values of less than 0.05 were considered statistically significant.
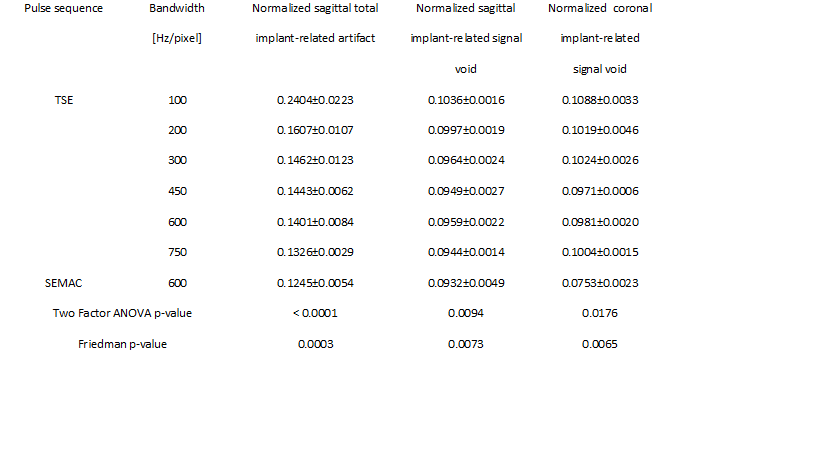
Results
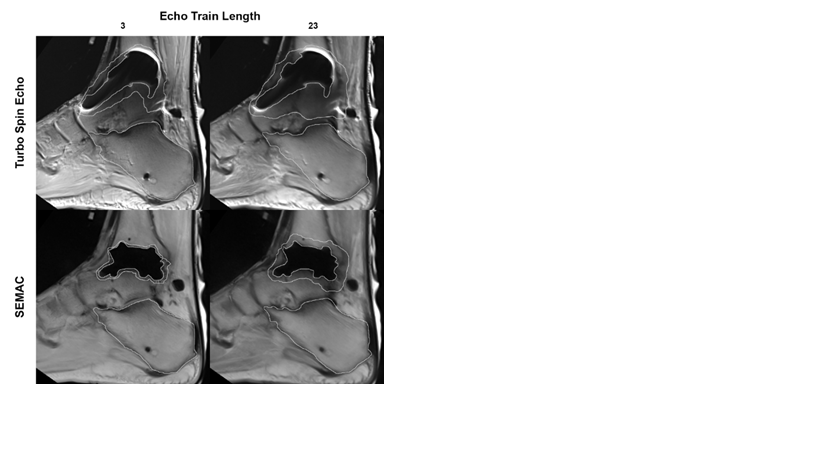
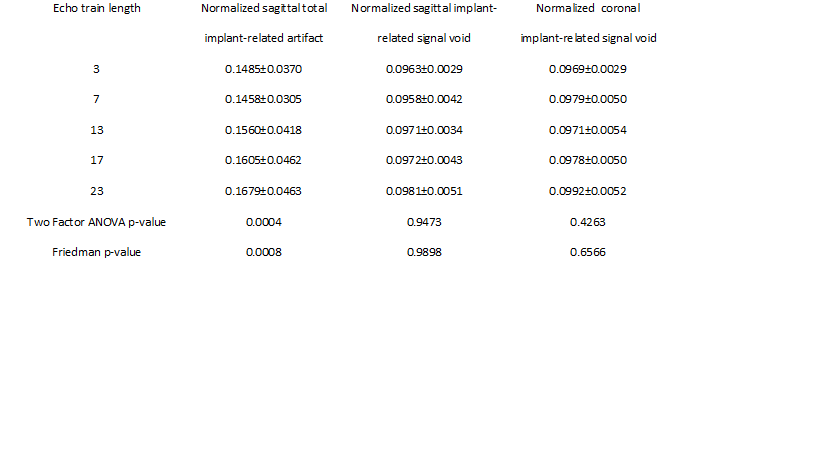
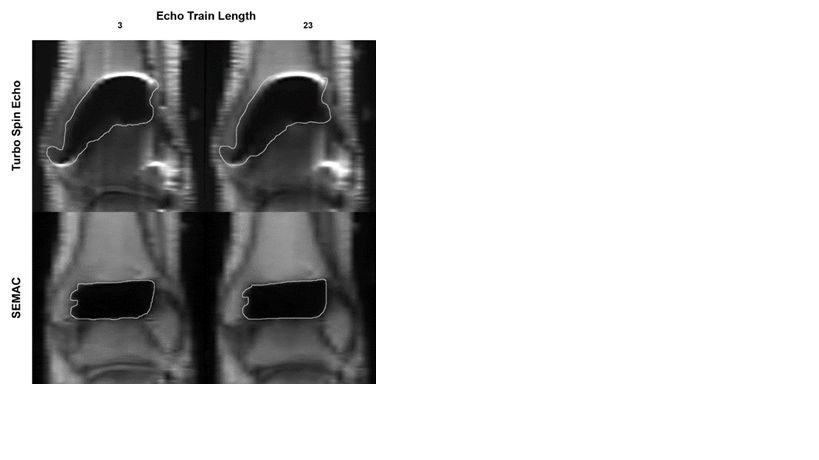
The two arms of the experiment resulted in a 5 x 6 matrix with one axis of increasing BW and one axis of increasing ETL, as well as one CS-SEMAC series of increasing ETL (Figure 1). Observer ratings showed significantly higher rankings (p < 0.0001) of MR images obtained with high BW and short ETL. Nemenyi pairwise comparisons showed significant difference between the group of ETL of 3 and 7 and the group of ETL of 17 and 23 (p < 0.0001, respectively). Inter-rater variability was excellent for BW with a weighted kappa coefficient of 1 and moderate for ETL with a weighted kappa coefficient of 0.57, which is probably due to smaller differences between adjacent ETL increments. The normalized total implant-related artifact ranged from a minimum of 0.119 for the CS-SEMAC pulse sequence with a BW of 600 Hz/pixel and ETL of 3 to a maximum of 0.265 for the turbo spin echo sequence with BW of 100 Hz/pixel and ETL of 23. The calcaneal area measurements that were used to normalize the artifact areas showed a low degree of variation from 25.02-25.50 cm^2 for the range of tested BW and 25.11-25.23 cm^2 across the tested ranges of ETL. Longer echo trains significantly increased the total implant-related artifact when averaged across all respective BW (p = 0.0004) (Figures 1, 2, 3), whereas higher BW significantly decreased the total implant-related artifact when averaged across all respective ETL (p<0.0001) (Figures 1 and 5). On CS-SEMAC images, there was a significant positive correlation between ETL and the total implant-related artifact (Pearson coefficient = 0.9, p = 0.036). Inter-observer agreement of the total implant-related artifact was excellent with a weighted kappa coefficient of 0.78. Sagittal and coronal implant-related signal void areas were not significantly affected by longer echo trains (p=0.95 and p=0.43, respectively) (Figures 2, 3, 4), but were significantly reduced with higher BW (p < 0.0001 and p < 0.0001, respectively) (Figures 1 and 5). There was no significant correlation between ETL and through-plane signal void length (Pearson coefficient = -0.15, p = 0.80), but there was significant negative correlation between BW and through-plane signal void length (Pearson coefficient = -0.85, p = 0.034).Conclusion
We demonstrate the negative effects of increasing ETL on total implant-related artifact in a setting of controlled BW, echo spacing and effective echo time. The use of BW in excess of 500 Hz/pixel is a powerful means to achieve meaningful metal artifact reduction, whereas increasing ETL beyond 7 causes local degradation of image quality around the implant through the introduction of contrast and spatial blurring and resultant larger appearing artifact, rather than a reduction of susceptibility artifact.Acknowledgements
No acknowledgement found.References
1. Fritz J, Lurie B, Miller TT, Potter HG. MR imaging of hip arthroplasty implants. Radiographics. 2014;34(4):E106-32.
2. Hargreaves BA, Worters PW, Pauly KB, Pauly JM, Koch KM, Gold GE. Metal-induced artifacts in MRI. AJR Am J Roentgenol. 2011;197(3):547-55.
3. American College of Radiology. ACR–SPR–SSR Practice Parameter for the Performance and Interpretation of Magnetic Resonance Imaging (MRI) of the Hip and Pelvis for Musculoskeletal Disorders 2016 [updated 2016; cited 2016 11/2/2016]. Available from http://www.acr.org/~/media/fc429e5a40eb4513a6934d8037445473.pdf
4. American College of Radiology. ACR–SPR–SSR Practice Parameter for the Performance and Interpretation of Magnetic Resonance Imaging (MRI) of the Knee 2015 [updated 2015; cited 2016 11/2/2016]. Available from: http://www.acr.org/~/media/ACR/Documents/PGTS/guidelines/MRI_Knee.pdf.
5. Talbot BS, Weinberg EP. MR Imaging with Metal-suppression Sequences for Evaluation of Total Joint Arthroplasty. Radiographics. 2016;36(1):209-25.
6. Lee MJ, Kim S, Lee SA, Song HT, Huh YM, Kim DH, et al. Overcoming artifacts from metallic orthopedic implants at high-field-strength MR imaging and multi-detector CT. Radiographics. 2007;27(3):791-803.
7. Eustace S, Goldberg R, Williamson D, Melhem ER, Oladipo O, Yucel EK, et al. MR imaging of soft tissues adjacent to orthopaedic hardware: techniques to minimize susceptibility artefact. Clin Radiol. 1997;52(8):589-94.
8. Lu W, Pauly KB, Gold GE, Pauly JM, Hargreaves BA. SEMAC: Slice Encoding for Metal Artifact Correction in MRI. Magn Reson Med. 2009;62(1):66-76.
9. Sutter R, Ulbrich EJ, Jellus V, Nittka M, Pfirrmann CW. Reduction of metal artifacts in patients with total hip arthroplasty with slice-encoding metal artifact correction and view-angle tilting MR imaging. Radiology. 2012;265(1):204-14.
10. Fritz J, Ahlawat S, Demehri S, Thawait GK, Raithel E, Gilson WD, et al. Compressed Sensing SEMAC: 8-fold Accelerated High Resolution Metal Artifact Reduction MRI of Cobalt-Chromium Knee Arthroplasty Implants. Invest Radiol. 2016;51(10):666-76.
Figures