4996
Normalized STEAM-based DTI parameters allow robust assessment of muscle tears in football players.1Department of Biomedical Imaging and Image-guided Therapy-MR Centre of Excellence, Medical University of Vienna, Vienna, Austria, 2Department of Biomedical Imaging and Image-guided Therapy, Medical University of Vienna, Vienna, Austria, 3Orthopedic Department, Evangelisches Krankenhaus Wien, Vienna, Austria
Synopsis
STEAM-based DTI was applied to investigate lower limbs’ muscle tears in athletes using the contralateral muscles as reference.To account for possible physiological differences in DTI metrics between right and left limb, a ratio between two ROIs on the injured side (i.e.,one on the tear and one on a healthy area) and two ROIs on the contralateral limb (i.e.,both on healthy areas) was used. The ratio showed that structural changes, expressed by modifications in MD, FA, RD, fibers’ number and length, occur in muscle tears and are quantifiable by DTI.These findings are expected to improve the therapeutic management of muscle injuries.
PURPOSE
To investigate acute muscle tears affecting the lower limb of football players with Stimulated Echo Diffusion Tensor Imaging (STEAM-DTI).METHODS
Football players with clinically diagnosed acute muscle tear of the lower limb were investigated on a 3T TIM Trio MRI Scanner (Siemens Healthcare, Erlangen, Germany) using an 8-channel knee coil or a combination of 4-channel matrix array coil/12-channel spine coil.For the morphological assessment, axial, coronal and sagittal proton density fat-sat and axial T1-weighted TSE sequences were applied. Both limbs were also investigated using a prototype ss-EPI STEAM-DTI sequence: diffusion time 200ms, GRAPPA-2, FatSat, b-values 0 and 500s/mm2, 6 averages, 12 directions; 30 adjacent axial slices of 3.5mm thickness.Since STEAM-DTI images are affected by random artifacts due to involuntary muscle contraction, we applied a previously tested correction method based on the weighted mean of voxels’ signal intensity[1]. Each injury was rated according to the Munich Consensus classification[2] using morphological images. DSI Studio (http://dsi-studio.labsolver.org) was used for the DTI analyses. DTI metrics (i.e.,fractional anisotropy (FA), mean-(MD), radial-(RD) and axial (AD) diffusivity, number, length and volume of fiber tracks) were collected, after manual segmentation, from the entire injured muscle and from the healthy contralateral corresponding muscle and then compared (Student’s t-test). Freehand ROIs were drawn along the borders of each muscle tear (ROItear) and the same ROI was applied on the corresponding healthy contralateral muscle (ROIhc_t).Additionally, two other ROIs were drawn to rule out any physiological difference between right and left limb:one on a healthy area ipsilateral to the injury (ROIhi) and one on a corresponding contralateral area (ROIhc_i). To evaluate possible changes in DTI metrics due to the tear or laterality even in healthy tissue, all ROIs were compared using one-way ANOVA test Greenhouse-Geisser post-hoc Bonferroni corrected. Ratios of DTI metrics of the injured side (ROItear/ROIhi) and of the corresponding contralateral healthy areas (ROIhc_t/ROIhc_i) were performed and compared (Student’s t-test).RESULTS
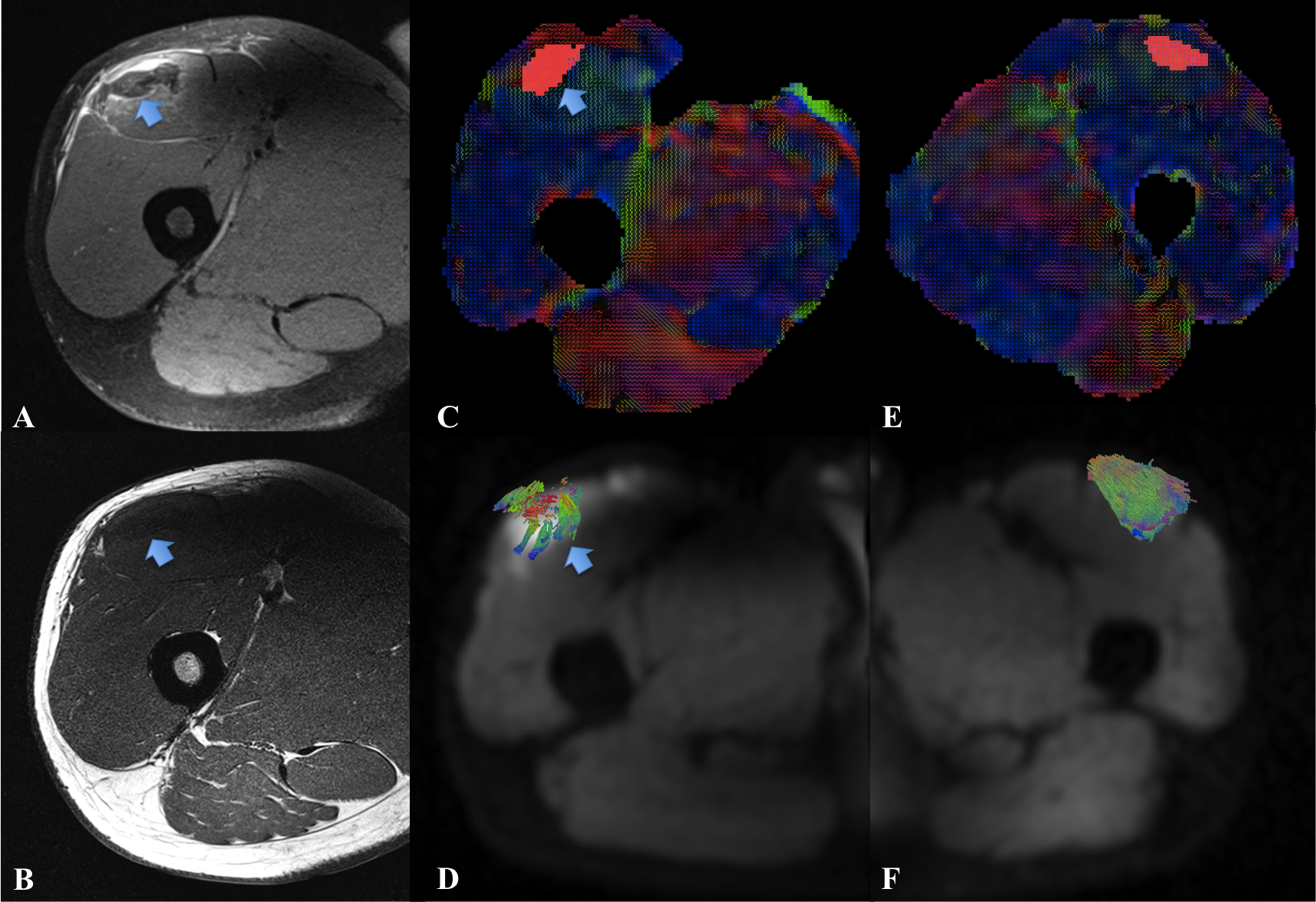
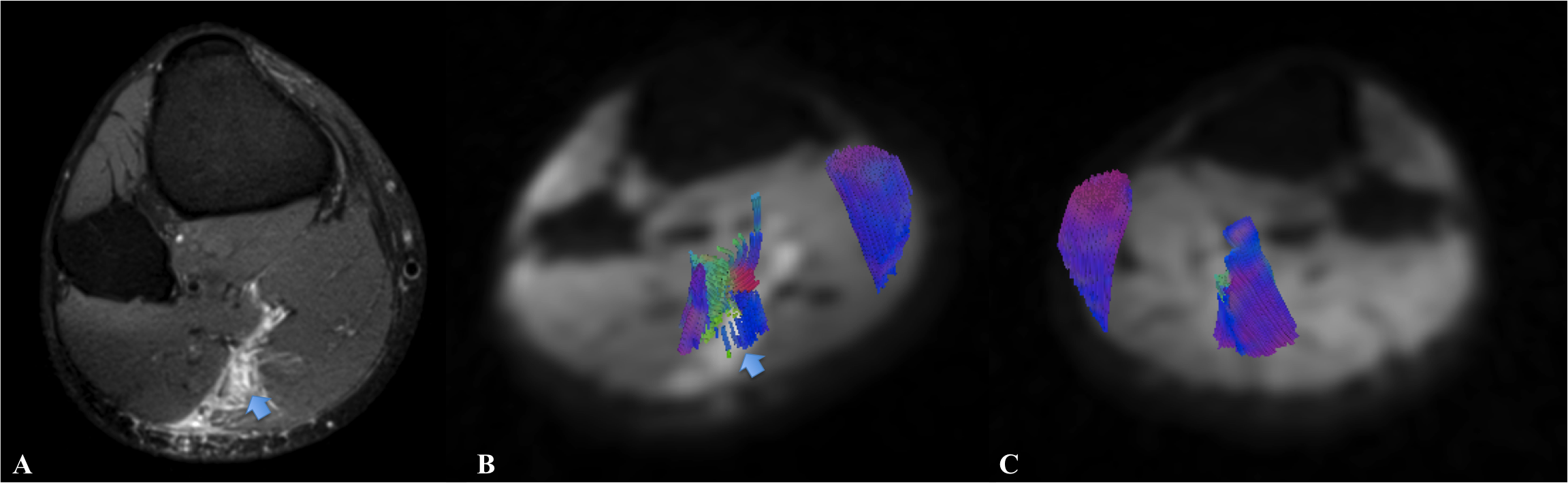
Eight patients with acute muscle tear were examined (all males, age range 20-36 years).Five showed an injury of the thigh and three of the calf. Seven lesions affected the right side and one the left.According to the Munich Consensus classification, two tears were rated as minor partial and six as moderate. No significant differences occurred comparing the entire injured muscle with the contralateral (p>0.05, each) except for higher AD values (+3.76%;p=0.048)(Fig. 1). No differences in DTI metrics occurred among all ROIs placed in healthy areas (p>0.05, each). ROItear showed higher MD (+10.32%, +12.31% respectively) and AD values (+6.60%, +9.08%, respectively)(p<0.05, each) than ROIhc_t and ROIhc_i but no differences emerged with ROIhi (all p>0.05). FA was lower in ROItear than in ROIhc_t and ROIhi (-11.49%, -19.81%;p<0.05, each) but no differences emerged with ROIhc_i (p>0.05). RD was higher in ROItear than in all other healthy areas (+13.14%, +10.46%, +14.73%;p<0.05) whereas no differences emerged for fibers’ number, length and volume (p>0.05). Greater differences occurred after normalizing the data.The comparison of the ratios (i.e., ROItear/ROIhi and ROIhc_t/ROIhc_i) revealed higher MD and RD (+6.02% and +8.69%) and lower FA (-19.51%) as well as a reduced number and length of fibers on the injured side (-55.65% and -39.47%) (p<0.05, each).No significant changes emerged for AD and fibers’ volume (p>0.05,each)(Fig. 2).DISCUSSION
Acute muscle injuries are very common in elite and non-elite athletes[3,4] but the prevalent MRI-based classification is still based on a rough quantification of the amount of torn fibers[5]. DTI already demonstrated to be highly suitable for the anatomical assessment of muscles but only a few studies investigated muscle tears. Indeed, Zaraiskaya et al.[6] showed lower FA and higher MD but only in two patients with acute lesions of the gastrocnemius whereas Froeling et al.[7] successfully evaluated muscle changes in marathon runners. For the first time, we used STEAM-based DTI to investigate muscle tears in athletes using the contralateral healthy side as reference and applying a normalization of the data.Indeed, physiological differences between right and left muscles may occur and affect DTI metrics but the application of a ratio provided robust results demonstrating that structural changes, affecting not only MD, FA and RD but also fibers’ number and length, occur in the tears and are quantifiable using DTI.CONCLUSIONS
STEAM-based DTI allowed a robust characterization and quantification of the injured fibers in athletes especially when a ratio between the injured and the contralateral muscles was applied. Aiming to improve the current imaging-based classification of muscle tears as well as to increase the accuracy of the therapeutic and prognostic management of injured athletes, future studies including a larger population and evaluating muscle tears also during the follow-up, are necessary.Acknowledgements
No acknowledgement found.References
1. Giraudo C, Motyka S, Trattnig S, Bogner W. Towards robust Diffusion Tensor Imaging of skeletal muscles via an automatic artifact removal tool. ISMRM 24th Annual Meeting, 2016, Singapore.
2. Mueller-Wohlfart H, Haensel L, Mithoefer K, et al. Terminology and classification of muscle injuries in sport: The Munich consensus statement. Br J Sports Med 2013;47:342-350.
3. Page P. Pathophyisiology of acute exercise-induced muscular injury:clinical implications. Journal of Athletic Training 1995;Vol 30;1.
4. Lee JC, Mitchell AWM, Healy JC. Imaging of muscle injury in the elite athlete. BJR 2012;85:1173-1185.
5. Hamilton B, Valle X, Rodas G, et al. Classification and grading of muscle injuries: a ?narrative review. Br J Sports Med 2015;49:306.
6. Zaraiskaya T, Kumbhare D, Noseworthy M. Diffusion Tensor Imaging in evaluation of human skeletal muscle injury. JMRI 2006;24:402-408.
7. Froeling M, Oudeman J, Strijkers GJ, et al. Muscle changes detected with diffusion-tensor imaging after long-distance running. Radiology 2015;274(2):548-562.
Figures