4986
The utilization of DDC value in detecting the status of LVI in rectal cancer patients at 3.0T MRI1Xijing Hospital, xi'an, People's Republic of China, 2Xijing Hospital, People's Republic of China
Synopsis
In this study, we aimed to investigate the value of DDC in assessing the status of lymphovascular invasion in patients with rectal cancer. Ninety-eight patients with rectal adenocarcinoma underwent DWI with 16 b-values at 3.0T MR system. We found there was an significant difference in DDC value between the LVI presence group (DDC=0. 893±0.151×10-3mm2/s, n=46) and the LVI absent group (DDC=0. 825±0.127×10-3mm2/s, n=52), (P=0.018). We speculate that DDC value derived from multi-b value DWI could be a useful functional parameter in detecting the status of LVI in rectal cancer patients.
Introduction and Purpose
Lymphovascular invasion (LVI) has been widely accepted as an independent pathological prognosis factor for patients with rectal cancer. Patients with LVI generally have a higher risk of disease progression and poorer prognosis1. In this study, we aimed to investigate the value of multi-b value DWI as a potential non-invasive tool for assessing the tumor aggressiveness with rectal cancer by analyzing the relationship between DDC value derived from SEM (stretched exponential model) and the evidence of the lymphovascular invasion confirmed by immunohistochemistry.Methods
Ninety-eight consecutive patients with pathologically confirmed rectal adenocarcinoma underwent DWI with 16 b-values (0,10,20,30,40,60,80,100,150,200,400,800,1000,1200,1500,2000s/mm2) at 3.0T MR system (MR750, GE healthcare company). Finally, forty-six LVI present patients and fifty-two LVI absent patients were included in our study, which were confirmed by immunohistochemistry (CD34 and D2-40). The distributed diffusion coefficient (DDC) derived from SEM model were generated by the MADC programs on an AW 4.6 workstation provided by the manufacturer (GE Healthcare). A Student’s Test was utilized to compare DDC value between the lymphovascular invasion presence group and the absent group. Statistical analyses were performed using SPSS version 19.0 and P values <0.05 were considered significant.Results
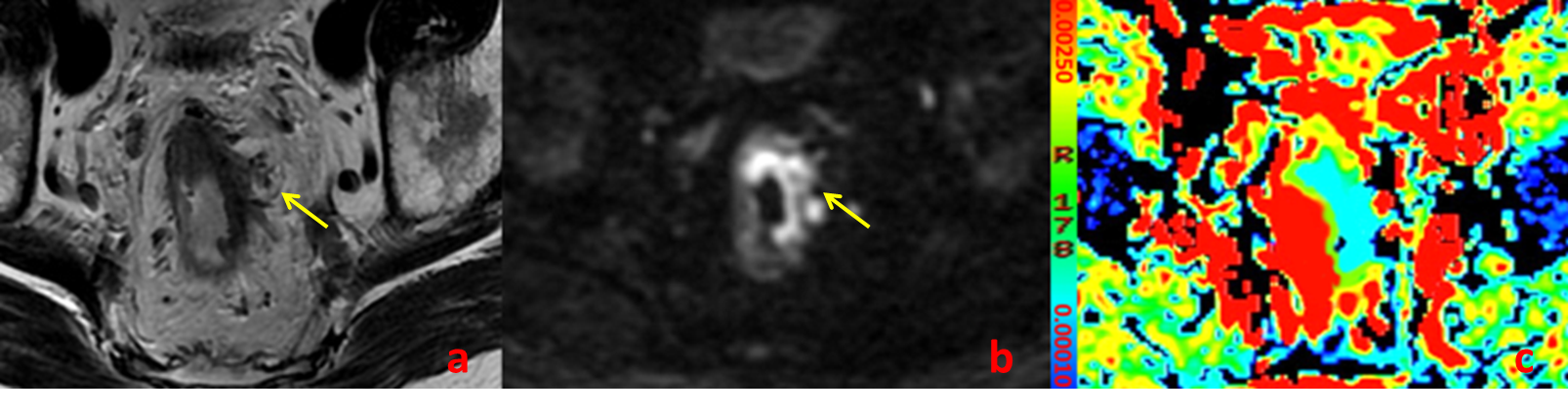
There was an significant difference in DDC value between the LVI presence group (DDC=0. 893±0.151×10-3mm2/s, n=46) and the LVI absent group (DDC=0. 825±0.127×10-3mm2/s, n=52), (P=0.018).The T2WI, DWI and pseudo-colored functional parameter (DDC) images of a patient with LVI were shown in Figure 1.Discussion
On the basis of our study, the patients with LVI had higher DDC value than those without LVI, which is consistent with the study by Akashi M2, but inconsistent with the study by Curvo-Semedo L3. Moreover, previous studies2, 3 had showed that ADC value was not useful in indicating the status of LVI, which might be attributed the reasons that the Gaussian diffusion model could not depict accurately the water molecule diffusion in vivo and few patients were included in their studies.
In our preliminary study, because the DDC value adjusted by α (alpha, the heterogeneity of intra-voxel diffusion) can reflect the true average of the heterogeneous intra-voxel diffusion rates, and in SEM model the number of contributing water pools is not concerned compared IVIM model and Gaussian diffusion model 4, we had demonstrated that SEM could assess tissue properties more reasonably than IVIM model and the Gaussian diffusion model with multi-b-values DWI. Therefore, the present study might carry more conviction in displaying and assessing the LVI invasion by DDC value.
As a general rule, the more aggressive tumor should present lower diffusion coefficient because of the increased cell density, ratio of nucleus to cytoplasm and decreased cell membrane permeability5. But in our study, we found a contradictory result that the DDC value is higher in patients with LVI than those without. We speculate it may be correlated with the more necrosis and distorted angiogenesis6 generated within tumor tissue in the LVI present patients and these characters would raise the value of diffusion coefficient7.
Conclusion
DDC value derived from multi-b value DWI could be a useful functional parameter in detecting the status of LVI in rectal cancer patients. And this will be benefit for the preoperative multidisciplinary team (MDT) discussion and alternative treatment strategies determination.Acknowledgements
This study is supported by the department of pathology. We appreciate Dr. Xin Fu, a professional pathologist, for his contribution in analyzing the pathology slices.References
[1] Compton CC, Fielding LP, Burgart LJ, et al. Prognostic factors in colorectal cancer. College of American Pathologists Consensus Statement 1999. Arch Pathol Lab Med 2000;124(7):979-94.
[2] Akashi M, Nakahusa Y, Yakabe T, et al. Assessment of aggressiveness of rectal cancer using 3-T MRI: correlation between the apparent diffusion coefficient as a potential imaging biomarker and histologic prognostic factors. Acta Radiol 2014;55(5):524-31.
[3] Curvo-Semedo L, Lambregts DM, Maas M, Beets GL, Caseiro-Alves F, Beets-Tan RG. Diffusion-weighted MRI in rectal cancer: apparent diffusion coefficient as a potential noninvasive marker of tumor aggressiveness. J Magn Reson Imaging 2012;35(6):1365-71.
[4] Bennett KM, Schmainda KM, Bennett RT, Rowe DB, Lu H, Hyde JS. Characterization of continuously distributed cortical water diffusion rates with a stretched-exponential model. Magn Reson Med 2003;50(4):727-34.
[5] Le Bihan D. Apparent diffusion coefficient and beyond: what diffusion MR imaging can tell us about tissue structure. Radiology 2013;268(2):318-22.
[6] Carmeliet P, Jain RK. Angiogenesis in cancer and other diseases. Nature 2000;407(6801):249-57.
[7] Bollineni VR, Kramer G, Liu Y, Melidis C, deSouza NM. A literature review of the association between diffusion-weighted MRI derived apparent diffusion coefficient and tumour aggressiveness in pelvic cancer. Cancer Treat Rev 2015;41(6):496-502.
Figures