4979
The Limitation in Predicting Lymph Nodes Stage by Using Magnetic Resonance Imaging on the Criterion of Size with Histopathological Analysis as Reference1Radiology, People’s Hospital, Peking University, Beijing, People's Republic of China, 2People’s Hospital, Peking University, Beijing, People's Republic of China
Synopsis
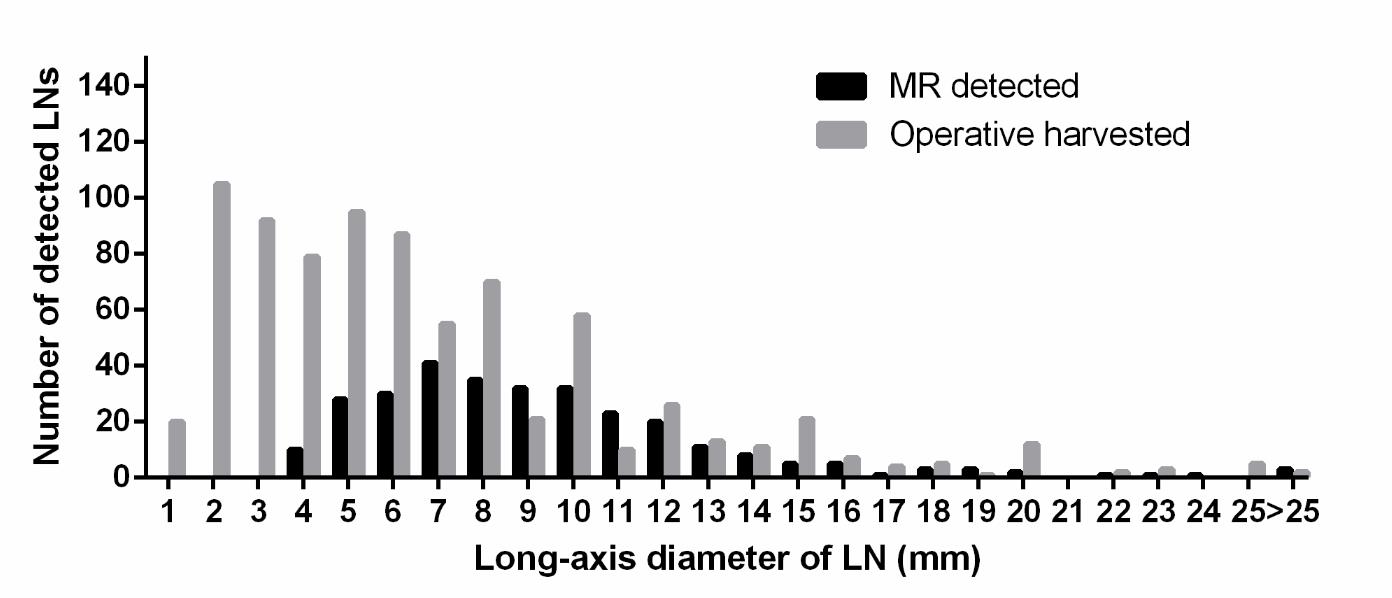
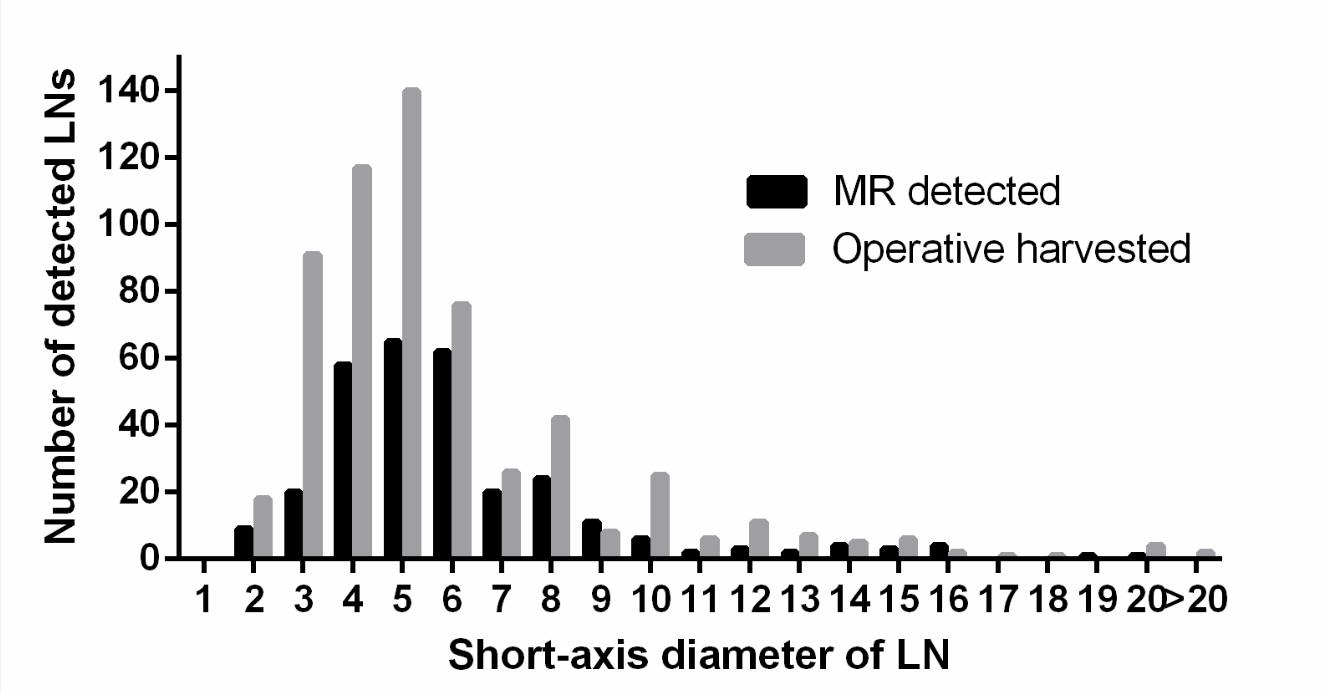
In spite of LN status is critical to the prognosis of patients with gastric cancer, MDCT and MRI cannot accurately assess metastatic LNs prior to surgery.In our study, 802 LNs of 30 patients with gastric carcinoma were harvested.during D2 lymphadenectomy. Only 36.7% (295/802) LNs were detected on preoperative MRI.. 31.5% (217/688) LNs (<8mm) were identified as malignant by pathology, whereas, 44.7% (51/114) LNs (≥8mm) were defined as metastatic. Forty-one metastatic LNs (19%, 41/215) with(≦3mm) were found in 7 patients (23.3%, 7/30) and caused N stage upstaging in 3 patients, which could not be detected by MRI.
Purpose
Lymph nodes (LN) status has been demonstrated as one of the most critically independent predictors of survival in patients with gastric cancer[1,2]. With the increase in N stage, survival rates dramatically decrease from 86.1% to 5.9% [3]. Extended lymphadenectomy (D2) considered as the standard surgical resection have been shown to decrease the rate of local recurrence (LR) and increase the rate of overall survival (OS)[4], however, conflicting results are achieved , such as a significant increase in anastomotic leaks, higher postoperative complication and reoperation rates, increased length of hospital stay and a 30-day mortality rate [5].
Accurate assessment of metastatic LNs prior to surgery is essential to determining appropriate therapeutic strategies and personalized surgery[6]. However, based on recently published meta-analyses on predicting lymph node stage (N stage), both MDCT and MRI,which are used to distinguish benign and metastatic gastric cancer , cannot be used to reliably confirm or exclude the presence of LN metastasis before operation.This study aims to investigate the limitation of MRI in predicting metastatic LNs in patients with gastric cancer based on size criterion by using MRI with pathological analysis as reference.
Methods
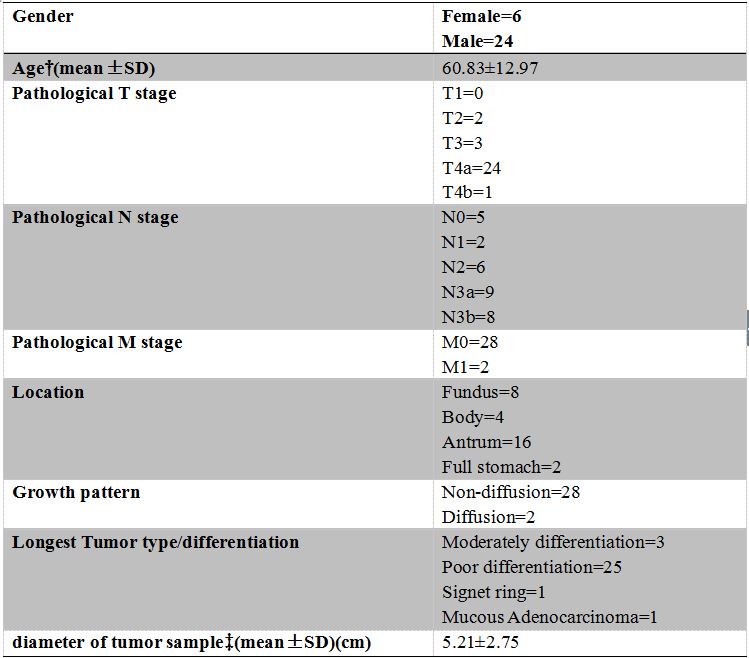
This prospective maintained study included 30 patients with pathologically proven gastric carcinoma between October 2010 and March 2011. Every patient underwent abdominal MRI before curative gastrectomy and D2 lymphadenectomy. LN was detected and measured on MRI by radiologists in consensus. Short-axis diameter of LN (≥8mm) was identified as metastatic LN on MRI [7-12]. Based on histopathological examination, the harvest number and diameter of each LN were measured. The differences in diameter of metastatic and benign LNs were compared by Mann-Whitney U test.Results
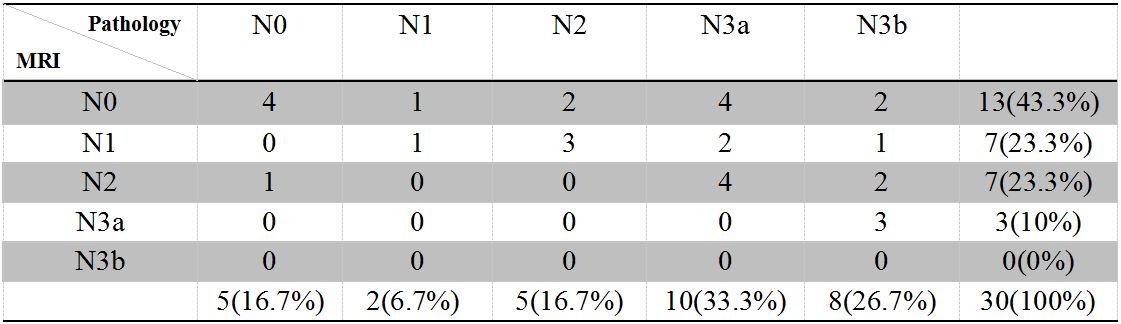
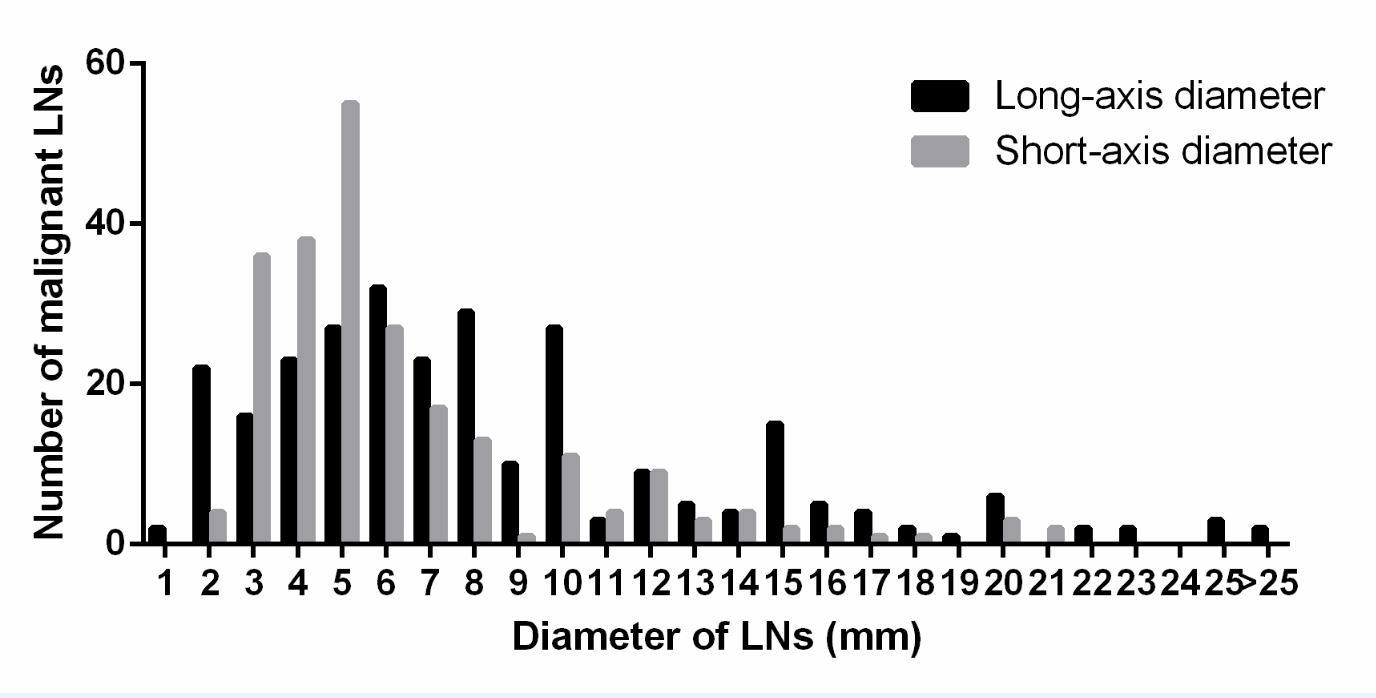
Two hundred ninety-five (36.7%, 295/802) LNs were detected and 187 LNs (≥8mm) identified as malignancy by MRI. In comparison, 802 LNs was harvested by surgery and 268 metastatic LNs (33.4%, 268/802) were identified according to pathological criteria. Moreover, 31.5% (217/688) LNs (<8mm) were identified as malignant by pathology, whereas, 44.7% (51/114) LNs (≥8mm) were defined as metastatic LNs. Forty-one metastatic LNs (19%, 41/215) with long-axis diameter≦3mm were found in 7 patients (23.3%, 7/30) and caused N stage upstaging in 3 patients, which could not be detected by MRI. In addition, MRI demonstrated all of the LNs belonged to group 2 [13, 14]and the missed LNs belonged to group 1Conclusion
In conclusion, MRI is limited in predicting metastatic LNs in gastric cancer. Small LNs (long-axis diameter ≤3mm) with a high frequency of metastases couldn’t be detected on MRI and less than half of LNs (short-axis diameter ≥8mm) were malignancy. In the future, we might focus on the identification of high-risk factors related to patient prognosis by using medical imaging in patients with locally advanced gastric cancer.Disscusions
Consistent with the present study, the ability of imaging modalities in predicting metastatic lymph nodes preoperative by using such criteria remains poor with overall accuracy of 66.1% (CT) and 53.4% (MRI), sensitivity of 77.2% (CT) and 85.3% (MRI), and specificity of 78.3% (CT) and 75.0% (MRI), respectively [6]. There may be two reasons explain these limitations. First, metastatic LNs are not always enlarged, as demonstrated by prior studies and the present study [15, 16]. In this study, a metastatic rate of 31.5% was obtained in the group of LNs smaller than 8mm in short-axis diameter. Moreover, a metastatic rate of 19% was detected in the group of LNs equate to or smaller than 3mm, which were too small to be detected by MRI caused by a limitation of special resolution. Secondly, peritumoral reactive changes as an immune response to tumorous tissue may lead to an enlargement of LNs[15-17]. As shown in this study, more than half LN ≥8mm in short-axis diameter (55.3%, 63/114) were benign nodes in accordance with pathological criteria. According to the MR and pathologic correlations, all group 2 LNs were detected on MR, which could be due to the fact that group 2 LNs were larger than group 1 LNs (median: 7.0 vs. 5.0). Metastatic LNs showed more irregular borders, heterogeneous enhancement patterns, higher attenuation, and lower ADC values compared with benign nodes. However, these characteristics could only be obtained with reproducibility in the LNs [8, 18] that were considerably enlarged, generally equal to or larger than 10mm in short-axis diameter. Compared to LNs harvested by pathological analyses, 63.2% could not be detected by MRI. Therefore, the majority of LNs could not be analyzed by above morphological criteria.Acknowledgements
The authors would like to express their sincere thanks to Bethany Hubbard (Manager of Medical Editing and Writing, iCoreMed Technology and Service LLC) who conducted a linguistic revision of this manuscript.References
[1] Son T, Hyung WJ, Lee JH, Kim YM, Kim HI, An JY et al. Clinical implication of an insufficient number of examined lymph nodes after curative resection for gastric cancer. Cancer. 2012; 118:4687-93.
[2] Zhao LY, Zhang WH, Chen XZ, Yang K, Chen XL, Liu K et al. Prognostic Significance of Tumor Size in 2405 Patients With Gastric Cancer: A Retrospective Cohort Study. Medicine. 2015; 94:e2288.
[3] Zhang XF, Huang CM, Lu HS, Wu XY, Wang C, Guang GX et al. Surgical treatment and prognosis of gastric cancer in 2,613 patients. World J Gastroenterol. 2004; 10:3405-8.
[4] El-Sedfy A, Dixon M, Seevaratnam R, Bocicariu A, Cardoso R, Mahar A et al. Personalized Surgery for Gastric Adenocarcinoma: A Meta-analysis of D1 versus D2 Lymphadenectomy. Ann Surg Oncol. 2015; 22:1820-7.
[5] Memon MA, Subramanya MS, Khan S, Hossain MB, Osland E, Memon B. Meta-analysis of D1 versus D2 gastrectomy for gastric adenocarcinoma. Ann Surg. 2011; 253:900-11.
[6] Chua YJ, Cunningham D. The UK NCRI MAGIC trial of perioperative chemotherapy in resectable gastric cancer: implications for clinical practice. Ann Surg Oncol. 2007; 14:2687-90.
[7]Seevaratnam R, Cardoso R, McGregor C, Lourenco L, Mahar A, Sutradhar R et al. How useful is preoperative imaging for tumor, node, metastasis (TNM) staging of gastric cancer? A meta-analysis. Gastric Cancer. 2012; 15 Suppl 1:S3-18.
[8]Fukuya T, Honda H, Hayashi T, Kaneko K, Tateshi Y, Ro T et al. Lymph-node metastases: efficacy for detection with helical CT in patients with gastric cancer. Radiology. 1995; 197:705-11.
[9]Chen CY, Hsu JS, Wu DC, Kang WY, Hsieh JS, Jaw TS et al. Gastric cancer: preoperative local staging with 3D multi-detector row CT--correlation with surgical and histopathologic results. Radiology. 2007; 242:472-82.
[10]Habermann CR, Weiss F, Riecken R, Honarpisheh H, Bohnacker S, Staedtler C et al. Preoperative staging of gastric adenocarcinoma: comparison of helical CT
[11]Monig SP, Zirbes TK, Schroder W, Baldus SE, Lindemann DG, Dienes HP et al. Staging of gastric cancer: correlation of lymph node size and metastatic .
[12]Sohn KM, Lee JM, Lee SY, Ahn BY, Park SM, Kim KM. Comparing MR imaging and CT in the staging of gastric carcinoma. AJR Am J Roentgenol. 2000; 174:1551-7.
[13].Japanese Gastric Cancer A. Japanese Classification of Gastric Carcinoma - 2nd English Edition. Gastric Cancer. 1998; 1:10-24.
[14].Dicken BJ, Bigam DL, Cass C, Mackey JR, Joy AA, Hamilton SM. Gastric adenocarcinoma: review and considerations for future directions. Ann Surg. 2005; 241:27-39.
[15].Kwee RM, Kwee TC. Imaging in assessing lymph node status in gastric cancer. Gastric Cancer. 2009; 12:6-22.
[16].Dassen AE, Lips DJ, Hoekstra CJ, Pruijt JF, Bosscha K. FDG-PET has no definite role in preoperative imaging in gastric cancer. Eur J Surg Oncol. 2009; 35:449-55.
[17]Mahdi H, Munkarah AR, Ali-Fehmi R, Woessner J, Shah SN, Moslemi-Kebria M. Tumor size is an independent predictor of lymph node metastasis and survival in early stage endometrioid endometrial cancer. Arch Gynecol Obstet. 2015; 292:183-90.
[18]Cheng J, Wang Y, Deng J, McCarthy RJ, Wang G, Wang H et al. Discrimination of metastatic lymph nodes in patients with gastric carcinoma using diffusion-weighted imaging. J Magn Reson Imaging. 2013; 37:1436-44
Figures