4968
Feasibility of Performing Dynamic and Delayed Enhancement and Magnetization Transfer Ratios in pediatric patients undergoing clinically-indicated MRE: pilot study to assess image quality for quantitative evaluation1Department of Diagnostic Imaging, The Hospital for Sick Children, Toronto, ON, Canada, 2Department of Medical Imaging, University of Toronto, Toronto, ON, Canada, 3Department of Radiology, Great Ormond Street Hospital, London, United Kingdom, 4Department of Radiology, The Royal Brisbane and Women's Hospital, Brisbane, Australia
Synopsis
Purpose: Assess feasibility of applying magnetization transfer (MT) and dynamic and delayed enhancement (DCE) sequences during MR Enterography(MRE) in children.
Methods: REB approved, in this prospective study, patients =/< 18 years undergoing MRE for suspected or proven inflammatory bowel disease were consented for application of MT and DCE sequenced in addition to standard clinical sequences. These were assessed and prospectively recruited and imaging sequences applied. Imaging was subjectively analysed by two radiologists or a radiologists and physicist in the first arm by consensus for sequence modification.
Results: Inter and intra-reader analysis was undertaken.
Conclusion: DCE is robust, MTR requires further modification.
Purpose: This feasibility study was designed to optimise magnetic resonance enterography (MRE) sequences targeting fibrosis - magnetization transfer (MT) and dynamic/delayed contrast enhanced (DCE) sequences - adapted for use in pediatric inflammatory bowel disease (IBD) patients, assessing image quality for reproducibility of quantitative analysis.
Background: Inflammatory bowel diseases - Crohn’s disease (CD), ulcerative colitis (UC) and indeterminate IBD (IBD-U) – have up to 25% onset in childhood and adolescence.1 Characterized by inflammation and fibrosis, which often co-exist, inflammation usually responds to medical therapy while fibrosis often requires surgery. Conventional MRE sequences have shown sensitivities and specificities in excess of 90% in detecting small bowel disease in pediatric IBD, less reliable in identifying fibrosis. A recent study by Rimola et al2 in adult IBD patients using DCE, showed bowel wall enhancement gain at 7 minutes vs. 70 seconds distinguished mild from moderate to marked fibrosis, even in the presence of inflammation. Additional studies in adults and animals applying MT sequences have demonstrated fibrosis through indirect measurement of macromolecules.3-5 Both DCE and MT sequences require subtraction to measure signal enhancement ratios (SER) and MT ratios (MTR), necessitating sequence modification to minimise motion artefacts - peristaltic, patient and respiratory motion, all compounded in children - additional to antiperistaltic agents. This feasibility study has been undertaken to optimise MT and DCE sequences in pediatric IBD patients, assessing diagnostic image quality and reproducibility of quantitative assessments, as a precursor to applying these sequences pre-operatively in patients undergoing bowel resection for validation against surgical pathology specimens for fibrosis.
Methods: Patients Pediatric patients ≤ 18 years with suspected or proven IBD undergoing clinically indicated magnetic resonance enterography (MRE) were included in this REB-approved prospective study. Exclusions were inability to complete a MT or DCE sequence set. Standard MRE Protocol The standard institutional protocol was applied6, using weight-based oral and intravenous gadolinium-based contrast and antispasmodic agents, with cine and static steady-state free-precession, single-shot T2 and 3D T1 weighted gradient echo (3DT1GE) sequences, the latter pre and post contrast (45 seconds), in axial and coronal planes, performed on a 1.5T MRI Scanner using body coils.
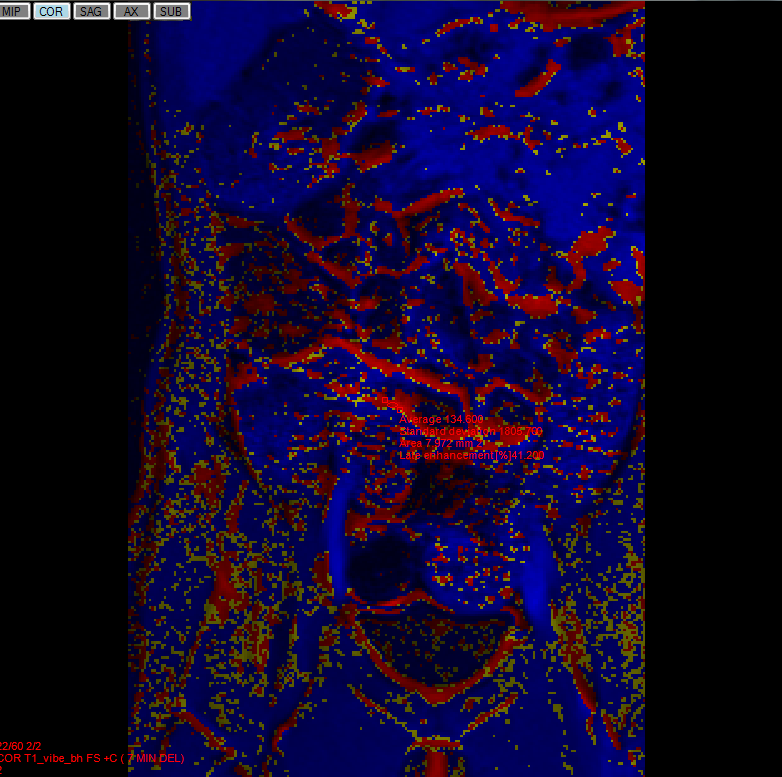
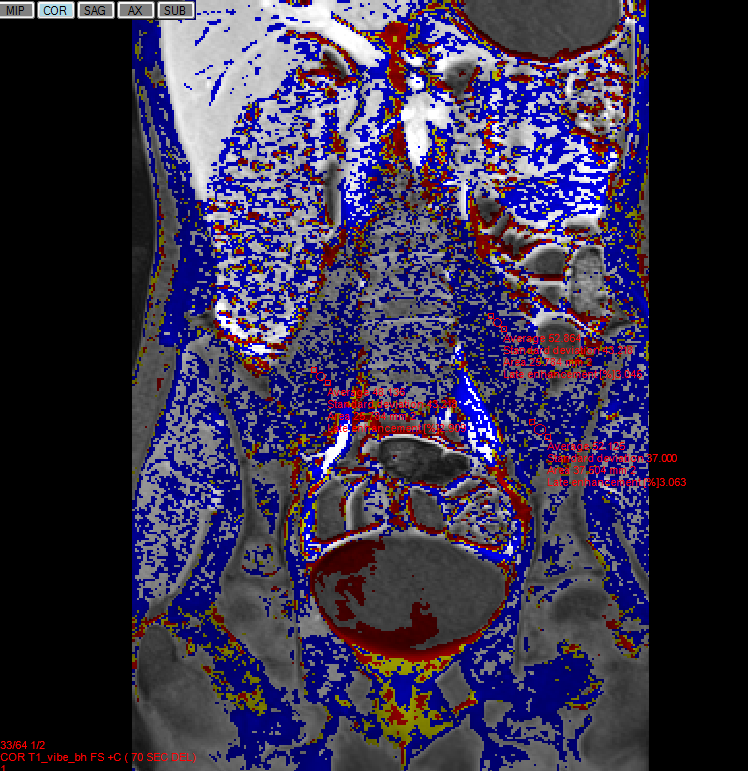
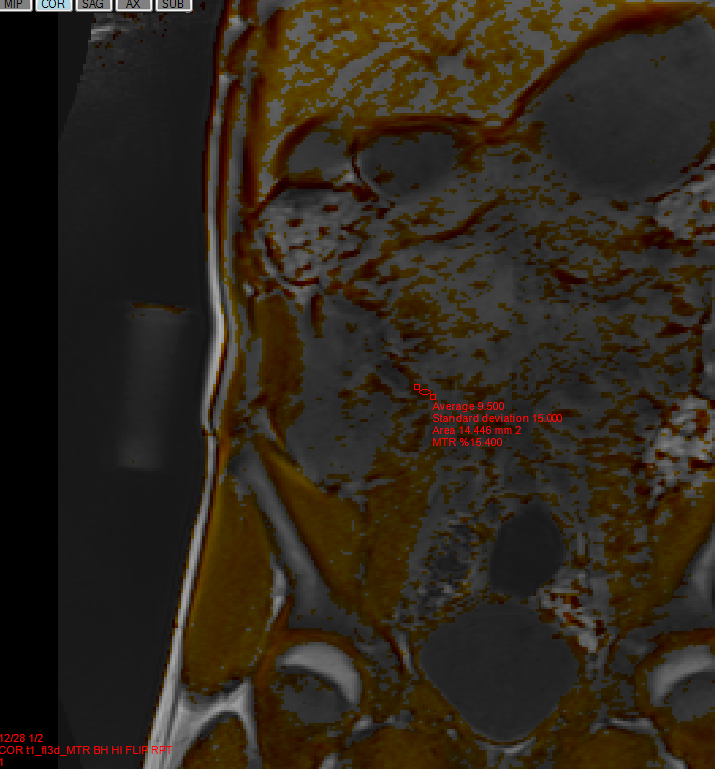
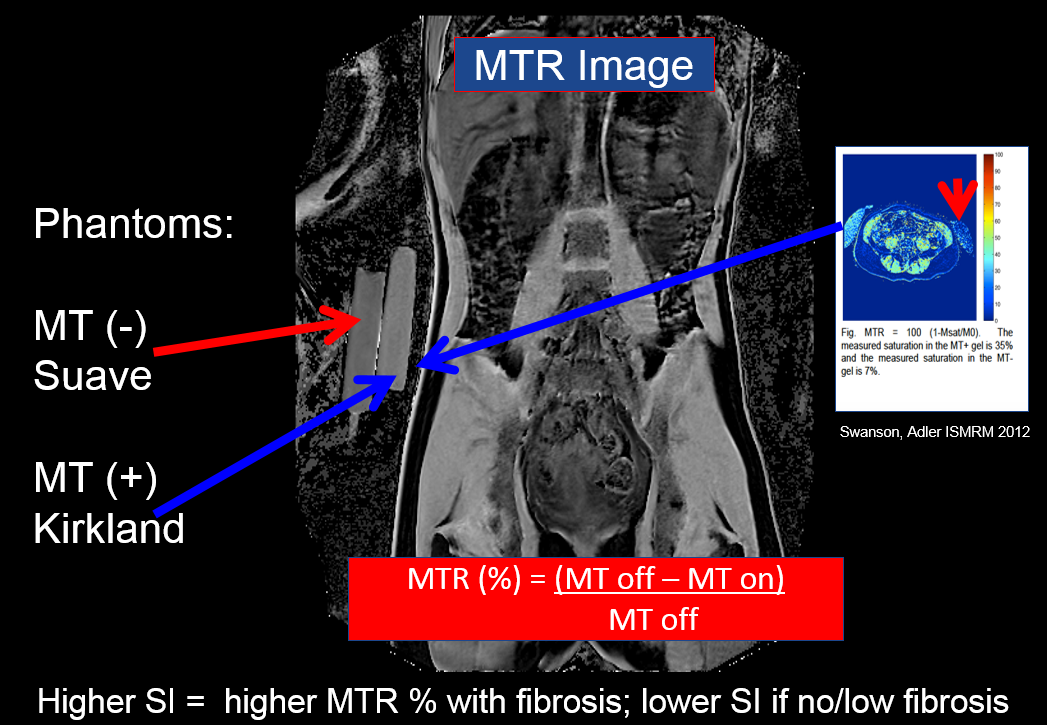
Supplementary Sequences DCE: Coronal 3DT1GE scans were also acquired at 70 seconds and 7 minutes; dynamic phase immediately post injection +/- after 7 minutes. MT: Coronal and limited axial (centered at iliac crests) 3DT1GE breath-hold scans were acquired with MT preparation pulse on and off with variable matrix and increasing flip angles. Optimization in the initial cohort was informed by qualitative assessment of bowel wall definition from consensus review by a radiologist and radiology fellow or medical physicist. Post-processing/Image Analysis Set DCE and MT sequence parameters were applied in a second cohort and quantitative analysis undertaken independently by a radiologist (Reader 1) and radiology fellow (Reader 2). A customised software package generated DCE and MT subtraction images as follows: MTR (%) [= (MT off – MT on)/MT off] and DCE SER Gain (%) [= [(WSI 7 min - WSI 70s)/(WSI 70s)*100] measuring 3 regions of interests each (ROI) in the terminal ileum (TI), psoas muscles (PM) and for MTR external phantoms.2,4,7 Intra- and inter-reader reliability were assessed using Cohen’s Kappa co-efficient.8
Results: Demographics In all, 27 patients were recruited with 25 included (13 females), 2 excluded, mean age 13.0 years (range 7.17-17.08). Of these, 23/25 (92%) completed all supplementary sequences, 2 (8%) either MT or DCE sequences, limited by patient movement, anxiety and/or vomiting. Majority of scans (17) were for new diagnosis or follow-up of CD.
Sequence Modification DCE timing was set after an initial few patients. MT scans variables were post- then pre-contrast acquisition, and variable matrix and flip angles (10-25 degrees). A final cohort of 10 patients with set DCE and MTR parameters underwent quantitative analysis.
Validation Data Inter-reader (Reader 1 vs. Reader 2): MTR - TI: k = 0.22, PM: k = 0.67; DCE - TI: k = 0.50, PM: k = 0.74. Intra-reader (Reader 1): MTR - TI: k = 0.40, PM: k = 0.62; DCE - TI: k = 0.65, PM: k = 0.72. (Figures 1-4)
Discussion/Conclusion: Motion artefact can lead to misregistration when performing subtraction imaging of bowel, particularly in children. If normal with mural thickness < 3 mm, visualization can be limited introducing error in quantification, though likely better appreciated in IBD with wall thickening. Inter- and intra-reader reliability for TI is higher for DCE than MTR, moderate to substantial and bordering on fair to moderate respectively, and lower than internal references for both, suggesting further sequence modification is warranted before proceeding to the surgical arm of this study.
Acknowledgements
No acknowledgement found.References
1. Benchimol EI, Fortinsky KJ, Gozdyra P et al. Epidemiology of pediatric inflammatory bowel disease: a systematic review of international trends. Inflamm Bowel Dis. 2011 Jan; 17(1):423-39.
2. Rimola J, Planell N, Rodríguez S et al. Characterization of inflammation and fibrosis in Crohn's disease lesions by magnetic resonance imaging. Am J Gastroenterol. 2015 Mar;110(3):432-40.
3. Dillman JR, Swanson SD, Johnson LA et al. Comparison of noncontrast MRI magnetization transfer and T2 -Weighted signal intensity ratios for detection of bowel wall fibrosis in a Crohn's disease animal. J Magn Reson Imaging. 2015 Sep;42(3):801-10.
4. Adler J1, Swanson SD, Schmiedlin-Ren P et al. Magnetization transfer helps detect intestinal fibrosis in an animal model of Crohn disease. Radiology. 2011 Apr;259(1):127-35.
5. Pazahr S, Blume I, Frei P et al. Magnetization transfer for the assessment of bowel fibrosis in patients with Crohn's disease: initial experience. MAGMA. 2013 Jun;26(3):291-301.
6. Greer ML. How we do it: MR enterography. Pediatr Radiol. 2016 May;46(6):818-28.
7. Swanson et al. Proc. Intl. Soc. Mag. Reson. Med. 2012; 20 (abstract).
8. Landis, J.R.; Koch, G.G. . The measurement of observer agreement for categorical data. Biometrics. 1977, 33 (1): 159–174
Figures