4938
Enabling high resolution MRE images of the breast1Division of Imaging Sciences and Biomedical Engineering, King's College London, London, United Kingdom, 2Department of Research Oncology, Guy's and St Thomas' NHS Foundation Trust, London, United Kingdom, 3Division of Cancer Studies, King's College London, London, United Kingdom, 4Department of Imaging Chemistry and Biology, King's College London, London, United Kingdom
Synopsis
Achieving high-resolution MR-Elastography images of the breast is a challenge due to shear wave attenuation and shadowing effects in breast tissue resulting in loss of wave energy and hence poor signal to noise ratio. We present a novel breast transducer set-up to ensure complete wave penetration throughout the entire breast. Waves reach even far upwards to enable quantification of axillary lymph nodes. Mechanical vibrations are generated via a novel concept utilizing an eccentric rotor that yields inherently constant amplitude with driving frequency. Volunteer results of wave speed and attenuation at 2mm isotropic resolution are presented including the axilla region.
Introduction
The application of MR-Elastography for the characterization of suspicious breast lesions has demonstrated very promising initial results (1-3). Various transducer concepts have been developed (4): Mayo Clinic proposed an acoustic shear elastography for clinical utility as quantitative diagnostic imaging tool adjunct to ultrasound (5), whilst Dartmouth College and KCL have been focusing their efforts on electromagnetically driven MRE transducer solutions (6,7). Yet, attenuation and shadowing effects due to loss of wave energy result often in low shear wave amplitudes. Usage of higher driving frequencies (80Hz and beyond) have been hampered due to reduced transducer amplitude, frequency and phase impurities of the systems. Another limitation in existing MRE set-ups is the lack of quantifying the axillary region due to absent shear waves. Here, we present a combination of novel hardware and acquisition software that allowed for bilateral, high resolution MRE of the entire breast in approximately 10 min scan time.Purpose
To present a novel flexible concept for performing MRE in the breast using a gravitational transducer concept that enables high-resolution imaging of the entire breast including the axillary region.Materials & Methods
Breast MRE set-up
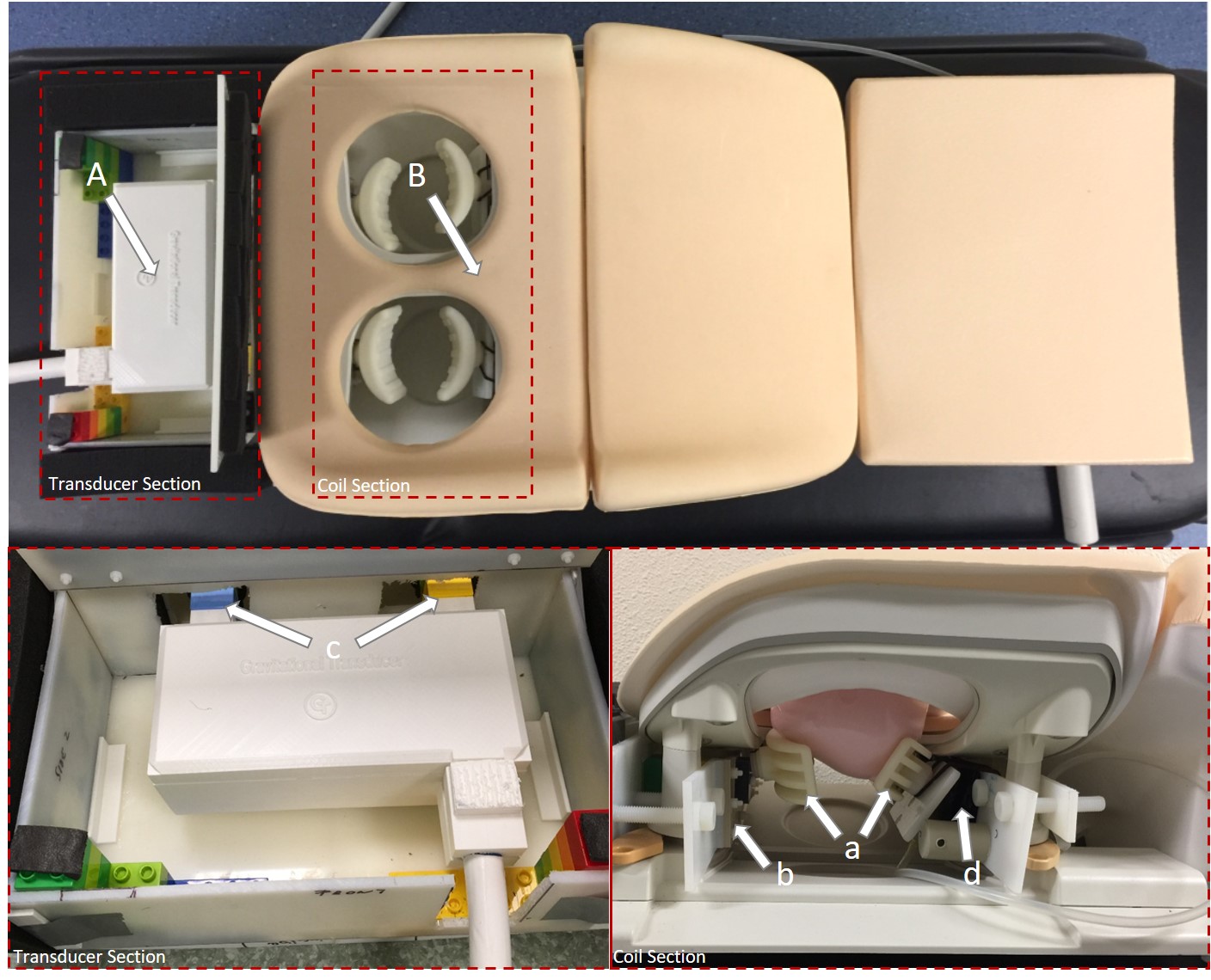
Our approach for generating mechanical vibrations is based on a commonly utilised technology in the mobile phone industry: a rotating eccentric mass that converts acceleration to centrifugal force and efficiently transmits the vibrations via the bearings into the casing. This “gravitational transducer” system (gT) is presented in Fig. 1. Here, the gT (A, 8) is integrated into the Philips Breast RF coil (B). C-shaped driving pistons (a) are mounted on PEEK lamellas (b) located on the cranial patient side and directly connected to the transducer unit (c). A second pair of movable C-shaped pistons is located on the opposite caudal patient side. They can rotate via hand-operated pneumatic pumps (d) and thereby fixate the breasts against the driving pistons. They serve as load-bearing structures. As presented in (8), this transducer approach yields inherently constant amplitude with frequency. Here, calibration and in vivo data have been acquired at 36Hz driving frequency.
Frequency response measurements
Acceleration measurements (Fig. 2) were performed at fVIB=36Hz driving frequency using 3D accelerometer chips mounted to the driving pistons. The system was mechanically loaded using breast phantoms and water bottles to simulate the patient weight. The frequency response is basically a delta-function of the system demonstrating excellent linearity of the system.
In vivo Data
Bilateral MRE of the breast on healthy volunteers was performed on a clinical 3T MR Scanner (Achieva, Philips Healthcare, The Netherlands). Total acquisition time was 5mins providing entire breast coverage (FOV=384mm) at 2mm isotropic resolution covering 8 slices in FH-direction. Neither SENSE (factor 2) nor Multiband excitation (factor 3) was used. Thus, the entire breast could easily be covered in 10mins. A motion sensitized FLASH sequence (9) was used with fractional encoding (fMEG = 160 Hz) using an in-phase echo-time of TE=6.9ms and a vibrational frequency of fVIB=36 Hz. All 3-motion directions were encoded and eight wave images were acquired per wave cycle.
Results and Discussion
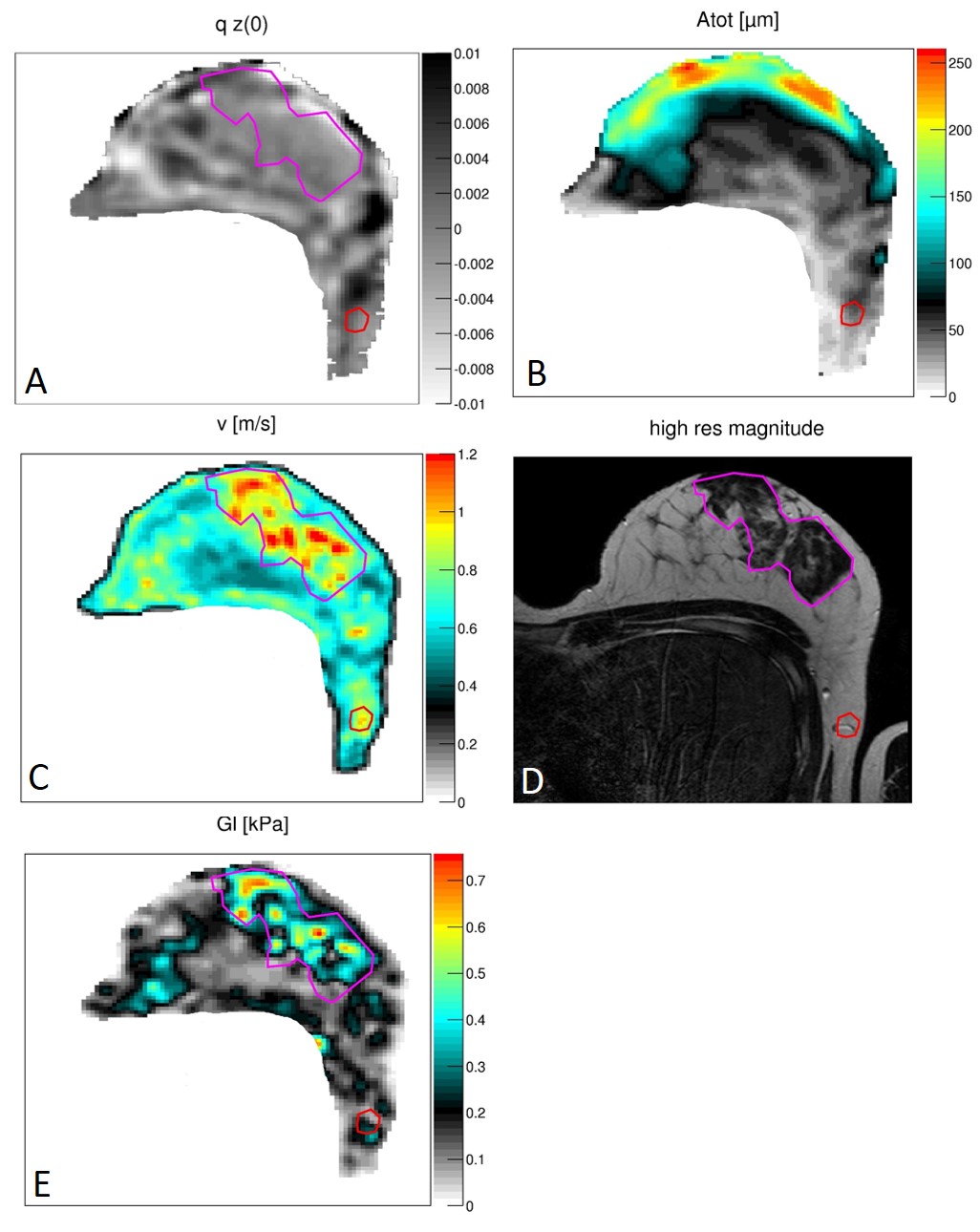
Fig. 3A depicts the z-component of the curl demonstrating excellent shear wave coverage throughout the entire breast. Fig. 3B shows the total wave amplitude: at the surface amplitudes >250mm are registered. At larger tissue depth, wave amplitude hovers around 50mm. The axilla region is properly illuminated enabling now the quantification of biomechanical properties. The reconstructed shear wave speed is presented in Fig. 3C: excellent correlation to anatomy is appreciated (fat/parenchyma) and the lymph node is perfectly depicted (red ROI in the anatomical image in Fig. 3D). Equally, the image of the viscosity Gl in Fig. 3E shows excellent correlation to anatomical structures with the lymph node exhibiting elevated values.Conclusion
A compact and easy to handle breast MRE set-up was successfully designed, built and tested. The gT approach yields excellent frequency purity and enables high resolution breast MRE within 10mins.Acknowledgements
This work was funded by the European Union’s Horizon 2020 research and innovation programme under grant agreement No 668039References
1. Lorenzen J, Sinkus R, Lorenzen M, et al. MR elastography of the breast:preliminary clinical results. Fortschr Röntgenstr. 2002;174:830-834.
2. Chen J, Kugel J, Yin M, Venkatesh SK. Magnetic Resonance Elastrography of Other Organs. In: Venkatesh SK, Ehman RL, eds. Magnetic Resonance Elastography. New York, NY: Springer New York; 2014:119-133.
3. Sinkus R, Lorenzen J, Schrader D, Lorenzen M, Dargatz M, Holz D. High-resolution tensor MR elastography for breast tumour detection. Phys Med Biol. 2000;45:1649-1664.
4. Uffmann K, Ladd ME. Actuation Systems for MR Elastography. IEEE Engineering in Medicine and Biology Magazine. 2008;27:28-34.
5. Denis M, Mehrmohammadi M, Song P, et al. Comb-Push Ultrasound Shear Elastography of Breast Masses: Initial Results Show Promise. PLoS ONE. 2015;10:e0119398.
6. Sinkus R, Holub O, Lambert S, CLOUGH R. Vibration inducing apparatus for magnetic resonance elastography. Google Patents; 2016.
7. Ji S, Roberts DW, Paulsen KD. Apparatus for measuring in-vivo mechanical properties of biological tissues. Google Patents; 2013.
8. Abstract, A new gravitational transducer concept for MR Elastography based on a rotational eccentric mass, Runge JH, Hoelzl SH, Sudakova J, Dokumaci AS, Nelissen JL, Lee J, Stoker J, Nederveen AJ, Nordsletten D, Sinkus R, submitted to ISMRM 2017
Figures