4934
Ultrafast Dynamic Contrast Enhanced MRI of the Breast Using Compressed Sensing: A Novel Technique for Separate Visualization of Breast Arteries and Veins in Very Early Phase1Department of Diagnostic Imaging and Nuclear Medicine, Kyoto University Graduate School of Medicine, Kyoto, Japan, 2Division of Clinical Radiology Service, Kyoto University Hospital, Kyoto, Japan, 3MR Application Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany, 4Department of Breast Surgery, Kyoto University Graduate School of Medicine, Kyoto, Japan
Synopsis
Ultrafast dynamic contrast enhanced (UF-DCE) MRI using compressed sensing enabled very fast scanning of the breast (every 3.7 sec/frame), and separately visualized breast arteries and veins. Breasts with cancers showed significantly shorter time intervals between arterial and venous visualization than the contralateral breasts without cancers. The time intervals in the breast with cancers tended to be shorter than those in the breasts with benign lesions. Shorter time intervals in breasts with cancers may reflect higher vascularity in malignancy. UF-DCE MRI has a potential to enable the differentiation of breast cancers in very early phase (0-60sec after contrast injection).
Background
On conventional dynamic contrast enhanced (C-DCE) MRI, breast cancers usually show ipsilateral higher vascularity1-3, though it is impossible to differentiate breast arteries and veins because of the long scan time (approximately 60 sec) for ensuring appropriate spatial resolution4. Ultrafast dynamic contrast enhanced (UF-DCE) MRI using compressed sensing has potential to separately visualize breast arteries and veins, preserving both temporal and spatial resolution. For the assessment of possible utility in the differentiation of breast cancer, this study aimed to analyze the timing of arterial/venous visualization, and the time interval between arterial and venous visualization.Methods
The institutional review board approved this study. Female patients who underwent MRI studies for diagnostic purpose between April and August 2016 were included in this study. Exclusion criteria were as follow: patients who did not underwent UF-DCE MRI in addition to the clinical studies, who had previous history of neoadjuvant chemotherapy, and who did not underwent pathological evaluation.
All MRI examinations were performed at a 3T scanner (MAGNETOM Skyra, Siemens Healthcare) with 18ch breast coil. The DCE MR protocols were as follows (Figure 1): 1. C-DCE MRI (pre phase); 2. UF-DCE MRI (15 sec before contrast injection-60 sec after contrast injection, 2 sec preparation time followed by 3.7 sec/frame✕continuous 20 frames); 3. C-DCE MRI (initial phase, 60-120 sec after contrast injection); 4. High spatial-resolution MRI (120-300 sec after contrast injection); 5. C-DCE MRI (delayed phase, 300-360 sec after contrast injection). UF-DCE MRI was performed by a prototype based on the 3D gradient-echo VIBE sequence using a compressed sensing reconstruction (TR/TE/FA=5.0/2.5/15°; Matrix, 384✕269; FOV, 360✕360mm; thickness, 2.5mm; 60 slices; number of iterations, 30). Gadobutrol (Gadovist, Bayer Healthcare, Leverkusen, Germany) was used as contrast material, and was intravenously infused at a dose of 0.1 ml/kg power and at a rate of 2.0 ml/s, followed by a 20 ml of saline at the same rate.
Using UF-DCE MR images, we reconstructed 19 maximum intensity projection (MIP) images from subtracted images (produced by the subtraction of the 1st of the 20 frames). Analysing the MIP images, we evaluated the each timing of breast arterial and venous visualization. The time intervals between arterial and venous visualization were calculated and compared between A) breasts with cancers vs. contralateral breasts without cancers (paired t-test) and B) breasts with cancers vs. breasts with benign lesions.
Results
A total of 28 female patients with 56 breasts were enrolled. Pathologically, breast cancers were confirmed in 27 breasts (bilateral cancers in 3 patients, unilateral cancers in 21 patients) and benign lesions were in 5 breasts. UF-DCE MRI separately visualized arteries and veins in all breasts except 2 without lesions. In the 2 breasts, only arteries were visualized during the acquisition time. Arteries were visualized at 6–11th frame (8.9-27.2 sec after contrast injection) and veins at 9–17th frame (19.9-49.1 sec after contrast injection). Representative cases were shown in Figure 2-4.
A) In the 21 patients with unilateral cancers, breasts with cancers showed significantly shorter time intervals between arterial and venous visualization than the contralateral breasts without cancers (2.7 frames [9.7 sec] vs. 4.8 frames [17.6 sec]; p<0.0001; Figure 5A).
B) The time intervals between arterial and venous visualization ranged 1–7 frames (mean, 3.0 frames [10.8 sec]) in the 27 breasts with cancers and 3–5 frames (mean, 3.8 frames [13.9 sec]) in the 5 breasts with benign lesions. The time intervals in the breasts with cancers tended to be shorter than those in the breasts with benign lesions (Figure 5B).
Discussion
UF-DCE MRI using compressed sensing enabled very fast scanning of the breasts (every 3.7 sec/frame) and separately visualized breast arteries and veins in 54 of 56 breasts. Compared to normal breasts and breasts with benign lesions, shorter time intervals between arterial and venous visualization were demonstrated in breasts with cancers, which may reflect higher vascularity in malignancy and can be a new approach to evaluate malignant potential.Conclusion
UF-DCE MRI using compressed sensing has a potential to enable the evaluation of breast tumor vascularity and the differentiation of breast cancers in very early phase (0-60sec after contrast injection).Acknowledgements
We thank Mr. Katsutoshi Murata and Mr. Yuta Urushibata, Siemens Healthcare K.K., for their technical support in this work.
This work was partly supported by Grant-in-Aid for Scientific Research on Innovative Areas “Initiative for High-Dimensional Data-Driven Science through Deepening of Sparse Modeling”, MEXT grant numbers 25120002, 25120008.
References
1. Sardanelli F, Iozzelli A, Fausto A, Carriero A, Kirchin MA. Gadobenate dimeglumine-enhanced MR imaging breast vascular maps: association between invasive cancer and ipsilateral increased vascularity. Radiology 2005; 235:791-797
2. Kul S, Cansu A, Alhan E, Dinc H, Reis A, Çan G. Contrast-enhanced MR angiography of the breast: Evaluation of ipsilateral increased vascularity and adjacent vessel sign in the characterization of breast lesions. AJR Am J Roentgenol 2010; 195:1250-1254
3. Mahfouz AE, Sherif H, Saad A, et al. Gadolinium-enhanced MR angiography of the breast: is breast cancer associated with ipsilateral higher vascularity? Eur Radiol 2001; 11:965-969
4. Kuhl C. The current status of breast MR imaging. Part I. Choice of technique, image interpretation, diagnostic accuracy, and transfer to clinical practice. Radiology 2007; 244:356-378
Figures
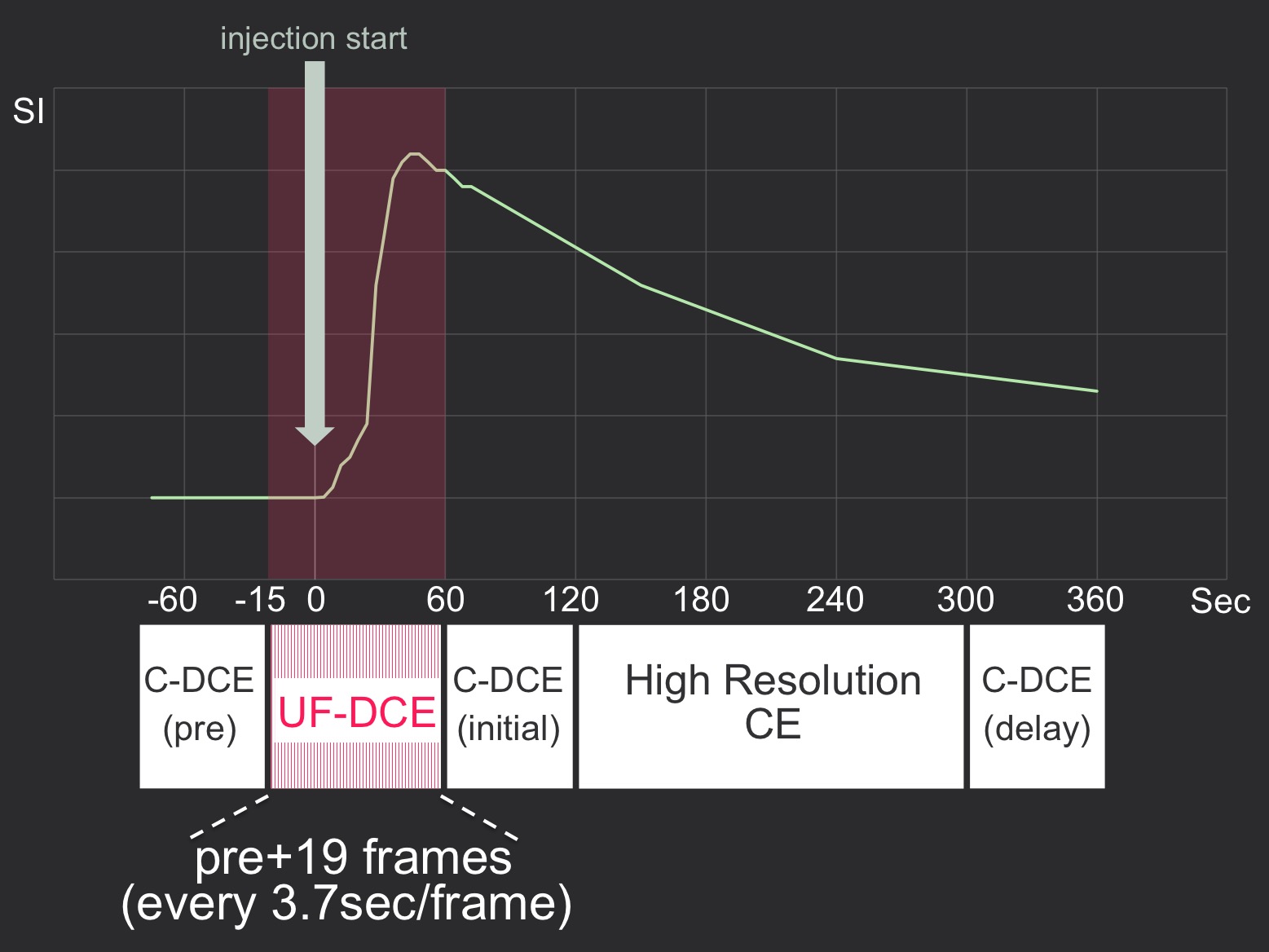
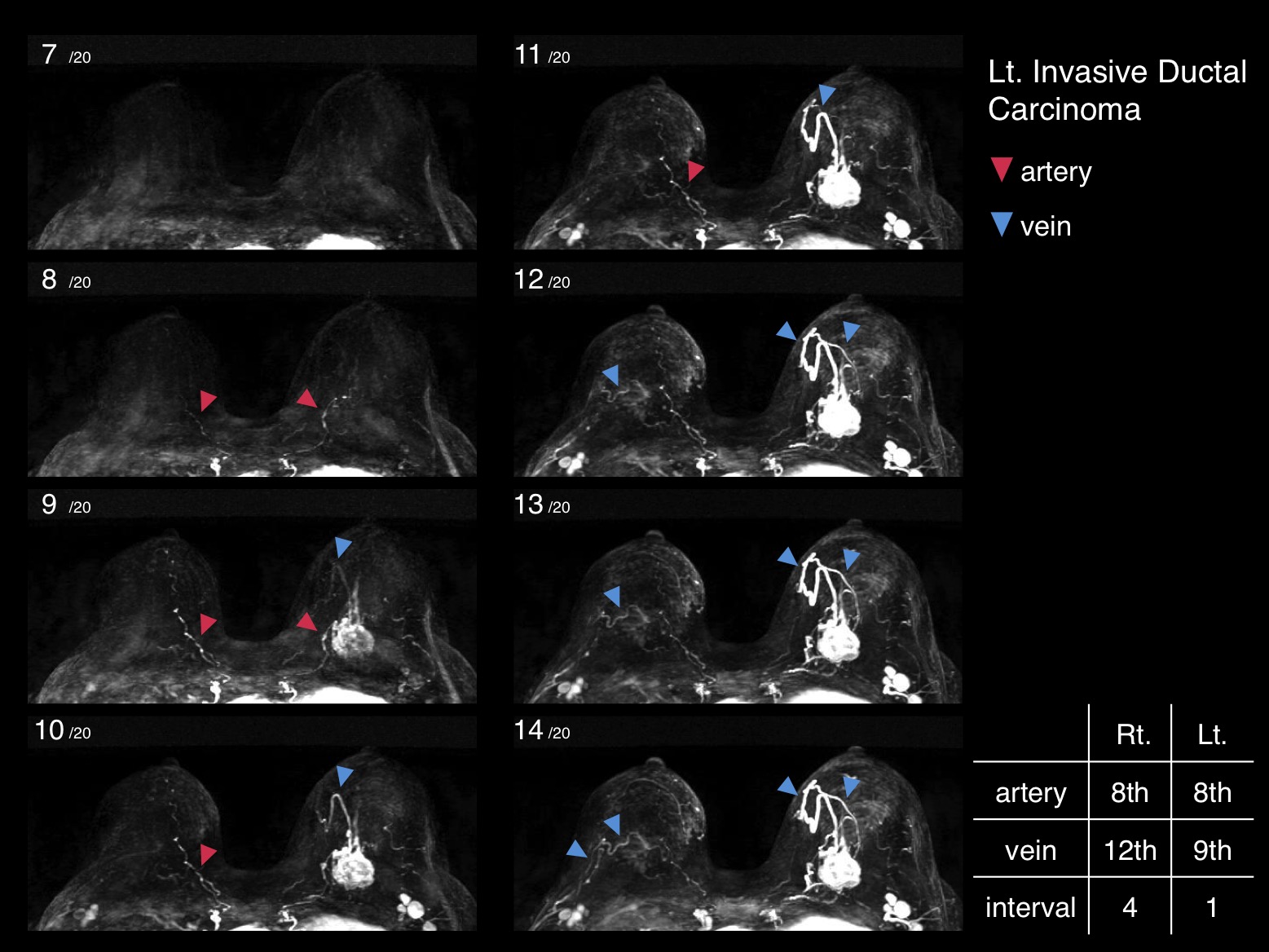
Figure 2. Lt. Invasive Ductal Carcinoma
The time intervals between arterial and venous visualization were Rt.=4 frames and Lt.=1 frame. In the left breast, both tumor and vein appeared at the same frame.
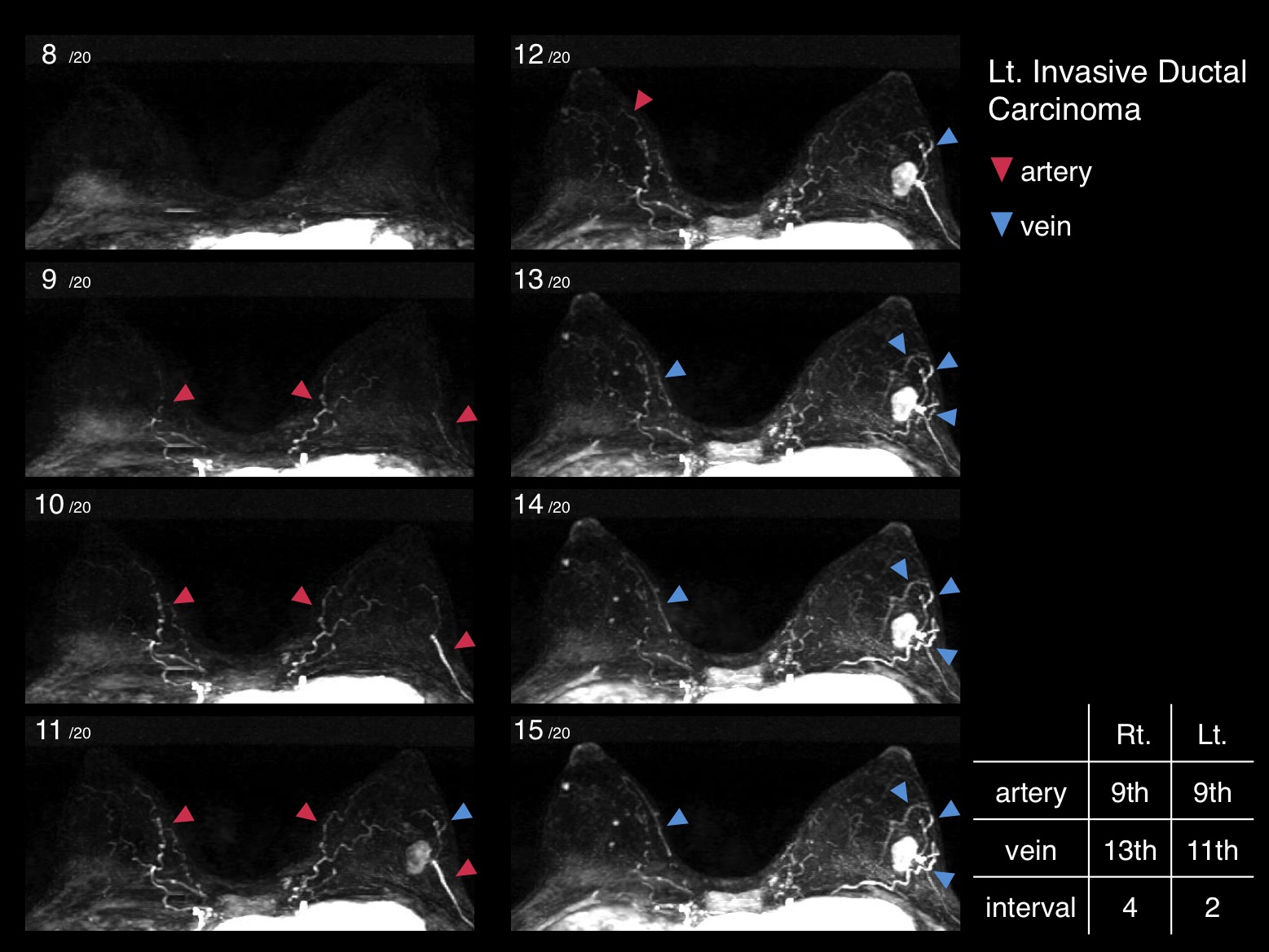
Figure 3. Lt. Invasive Ductal Carcinoma
The time intervals between arterial and venous visualization were Rt.=4 frames and Lt.=2 frames. In the left breast, both tumor and vein appeared at the same frame.
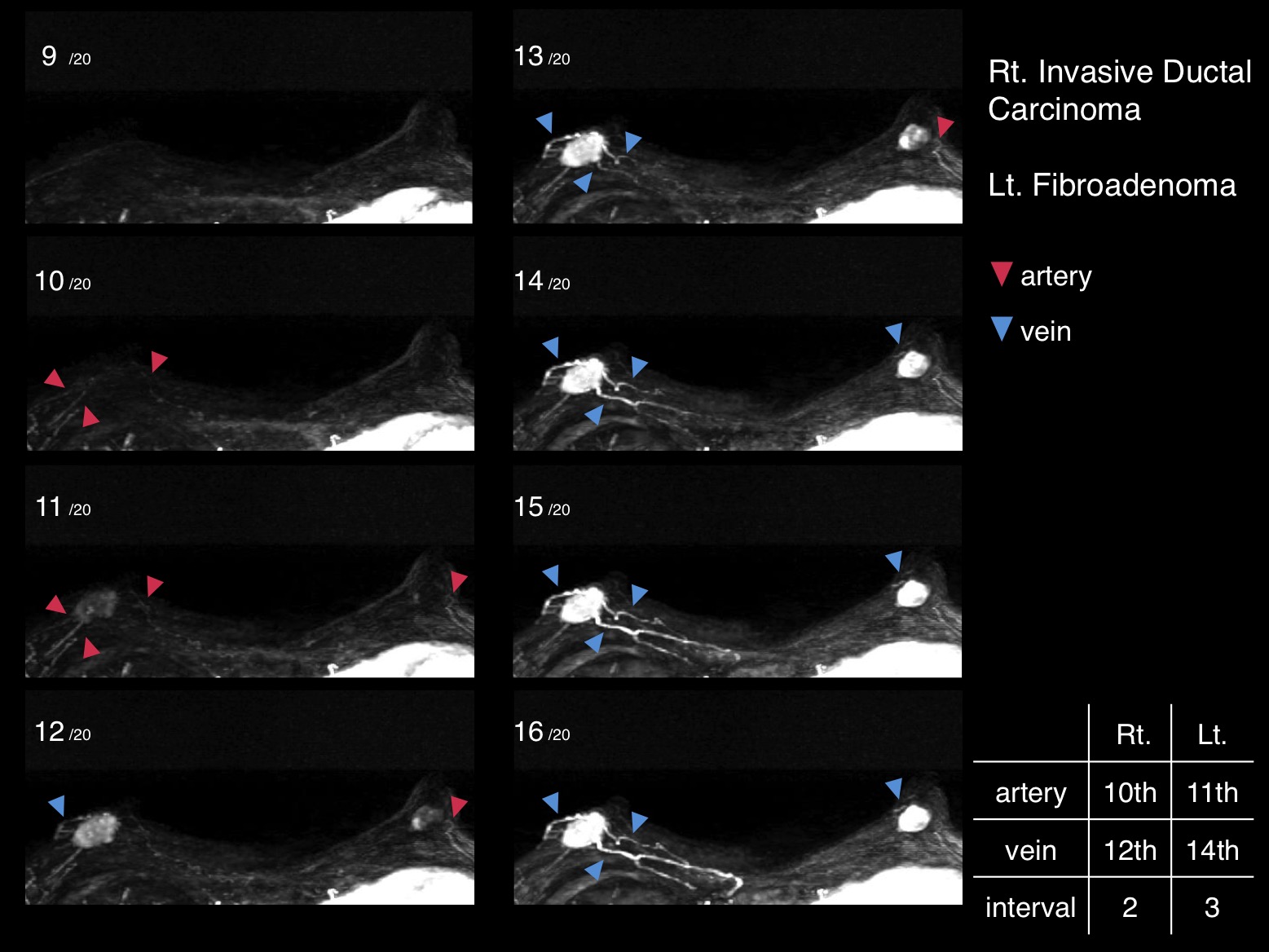
Figure 4. Rt. Invasive Ductal Carcinoma & Lt. Fibroadenoma
The time intervals between arterial and venous visualization were Rt.=2 frames and Lt.=3 frames.
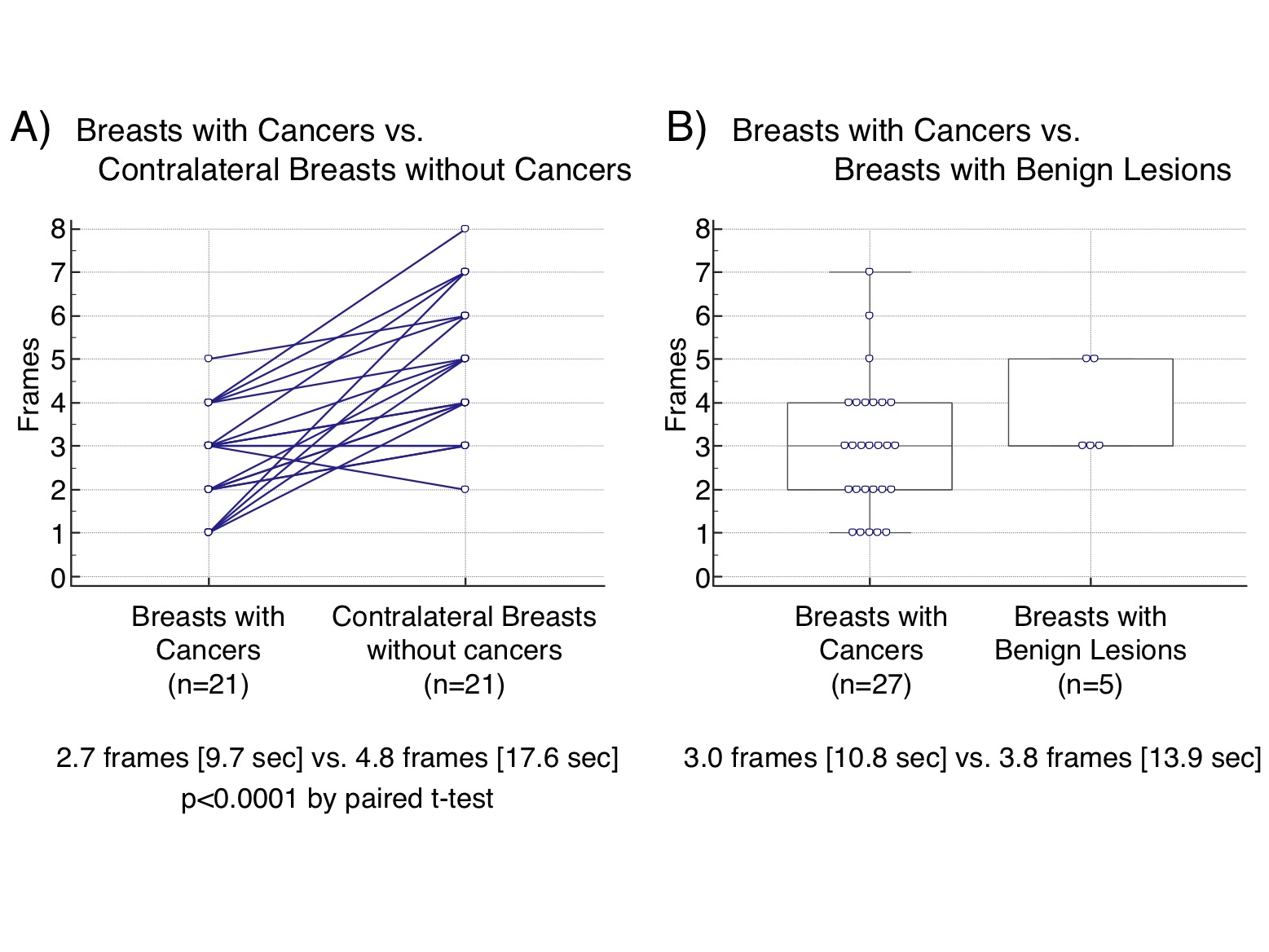
Figure 5. Time Intervals between Arterial and Venous Visualization
A) Breasts with Cancers vs. Contralateral Breasts without Cancers
B) Breasts with Cancers vs. Breasts with Benign Lesions