4929
Comparison of Radial and Cartesian Acquisitions in Breast MRI for Improved Visualization of the Axilla1Department of Medical Physics, University of Wisconsin Madison, Madison, WI, United States, 2Department of Radiology, University of Wisconsin Madison, Madison, WI, United States, 3Carbone Cancer Center, University of Wisconsin Madison, Madison, WI, United States, 4Cardiac Center of Excellence, GE Healthcare, Garching bei München, Germany, 5GE Global Research Europe, Garching bei München, Germany, 6Global MR Applications & Workflow, GE Healthcare, Madison, WI, United States
Synopsis
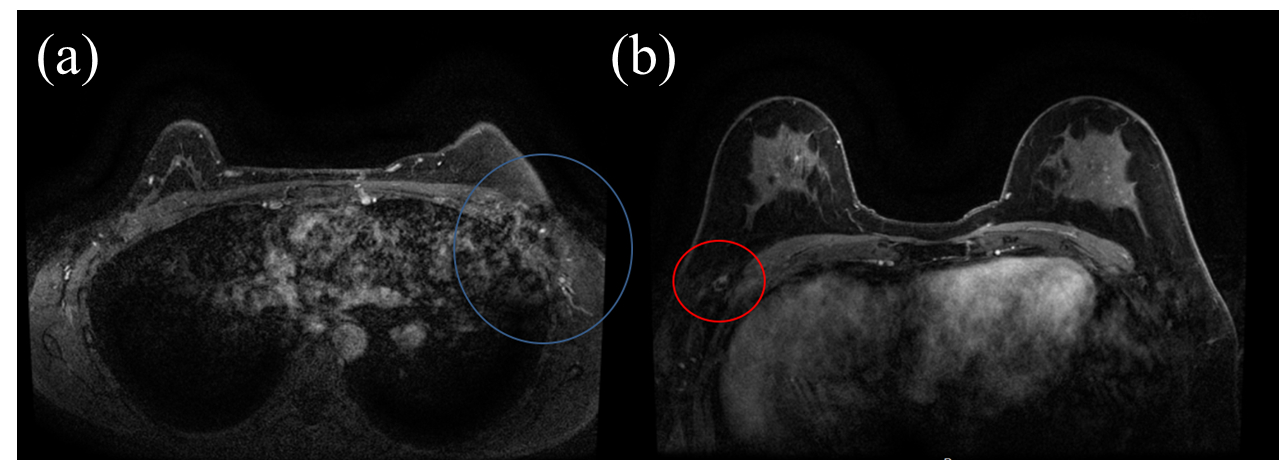
Dynamic contrast-enhanced (DCE) MRI is being increasingly used in the detection and diagnosis of breast cancer. Cartesian sampling is routinely used however ghosting artifacts caused by cardiac motion are a well known challenge that in some instances can severely obscure the gland tissue, axilla and even known cancer. Radial sampling has an intrinsic advantage for diminishing motion artifacts by averaging low special frequency signals through oversampling of central k-space data. In this study, we demonstrated the feasibility of using a 3D stack-of-stars radial acquisition to provide motion free images of the entire breast region including the axilla.
Introduction
There is increasing interest in the radiological diagnosis of axillary lymph nodes in patients with breast cancer, especially in the preoperative and post-neoadjuvant chemotherapy settings (1). As high-risk screening has progressively moved toward greater reliance on MRI, it becomes more important to provide comprehensive evaluation of the breasts and axillae, rather than relying on a second modality, such as ultrasound, for axillary assessment. Dynamic Contrast Enhanced (DCE) using conventional Cartesian sampling is known to be susceptible to ghosting artifacts, and for routine bilateral breast imaging, this includes ghosting due to cardiac motion (Figure 1). To avoid artifacts across the breast, the phase encoding direction is not anterior-posterior, but is instead medial-lateral (for axial imaging) or superior-inferior (for sagittal imaging). However, this leads to ghosting across the axillae in the commonly used axial scan plane. Prior work has looked at radial sampling for body imaging including abdominal (2-4) and breast (5-7), however there is limited work exploring the use of radial MRI specifically to address motion artifacts in breast imaging. The purpose of this study is to demonstrate the feasibility of using a 3D stack-of-stars radial acquisition to provide cardiac and respiratory artifact free visualization of the entire breasts, including the axillae.Methods
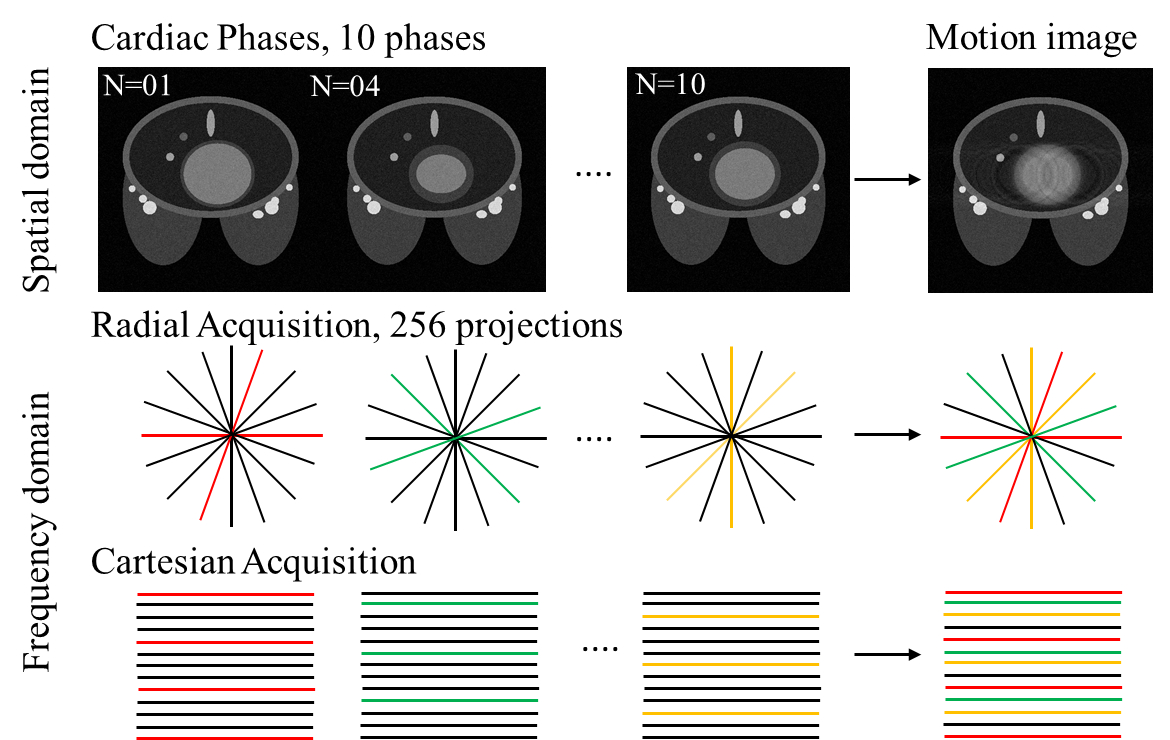
Simulations: First, a 3D stack-of-stars radial data acquisition was simulated by using a breast imaging phantom with cardiac motion. Simulated lesions were placed within a region near the axillae and had higher intensity than the surrounding fat tissue (Figure 2). A total of 10 cardiac phases were simulated and sub-sets of k-space data from each cardiac phase were sample and combined with Gaussian noise. The data were then recombined to simulate a Cartesian acquisition (matrix size 448×448) or radial acquisition with golden-angle (256 projections, and matrix size 448×448) during cardiac motion. A flow chart of the simulation is shown in Figure 2.
Volunteers: Six normal volunteers were imaged using radial and Cartesian acquisitions on a clinical 3T MR system (MR750w, GE Healthcare, Waukesha, WI) using an 8-channel breast coil (GE Healthcare) for this IRB approved, HIPAA compliant study. Acquisition times were 2:43 (min:sec) for the Cartesian and 2:52 for the radial acquisitions. Radial imaging was achieved using a 3D stack-of-stars golden-angle gradient echo imaging sequence and 256 radial projections were collected at each z-phase encode. The radial field of view (FOV) was oversampled to limit streaking artifact. Radial data were reconstructed by first shifting the center of the echo along each readout, followed by gridding. The Cartesian acquisition was combined with 2x parallel imaging acceleration.
Results
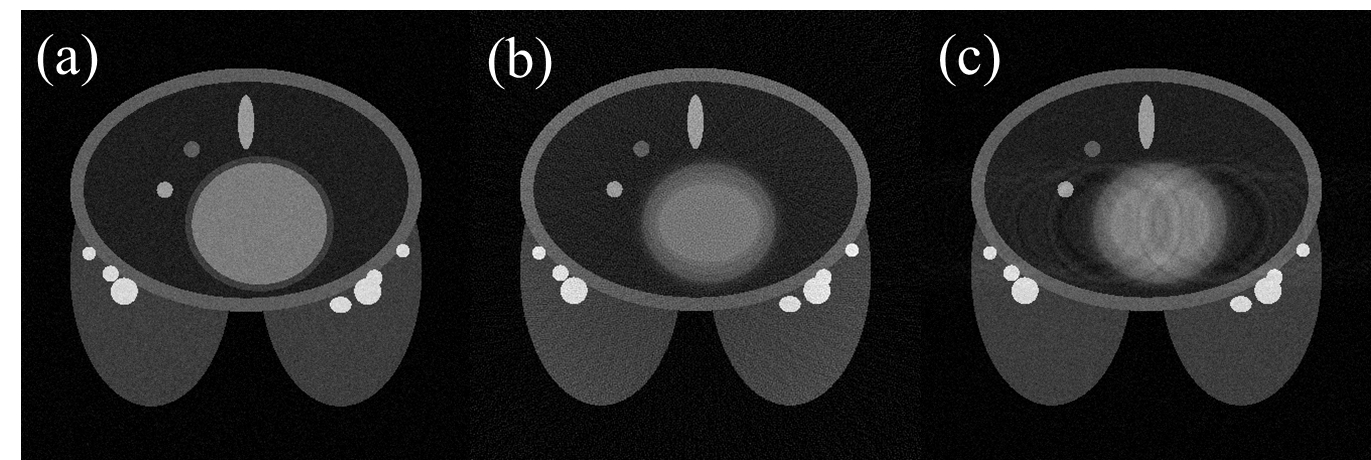
Simulations: Images from the numerical simulation are shown in Figure 3. The Cartesian acquisition demonstrates phase ghosting due to cardiac motion whereas the radial acquisition was not found to suffer from ghost artifacts, however there is some evidence of streaking due to radial undersampling and local blurring near the heart.
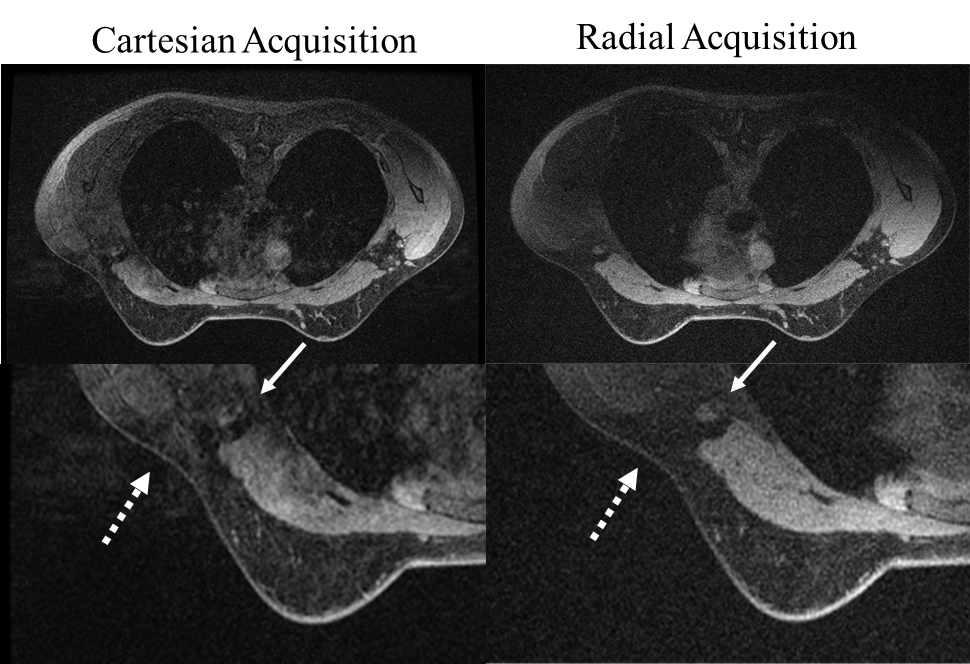
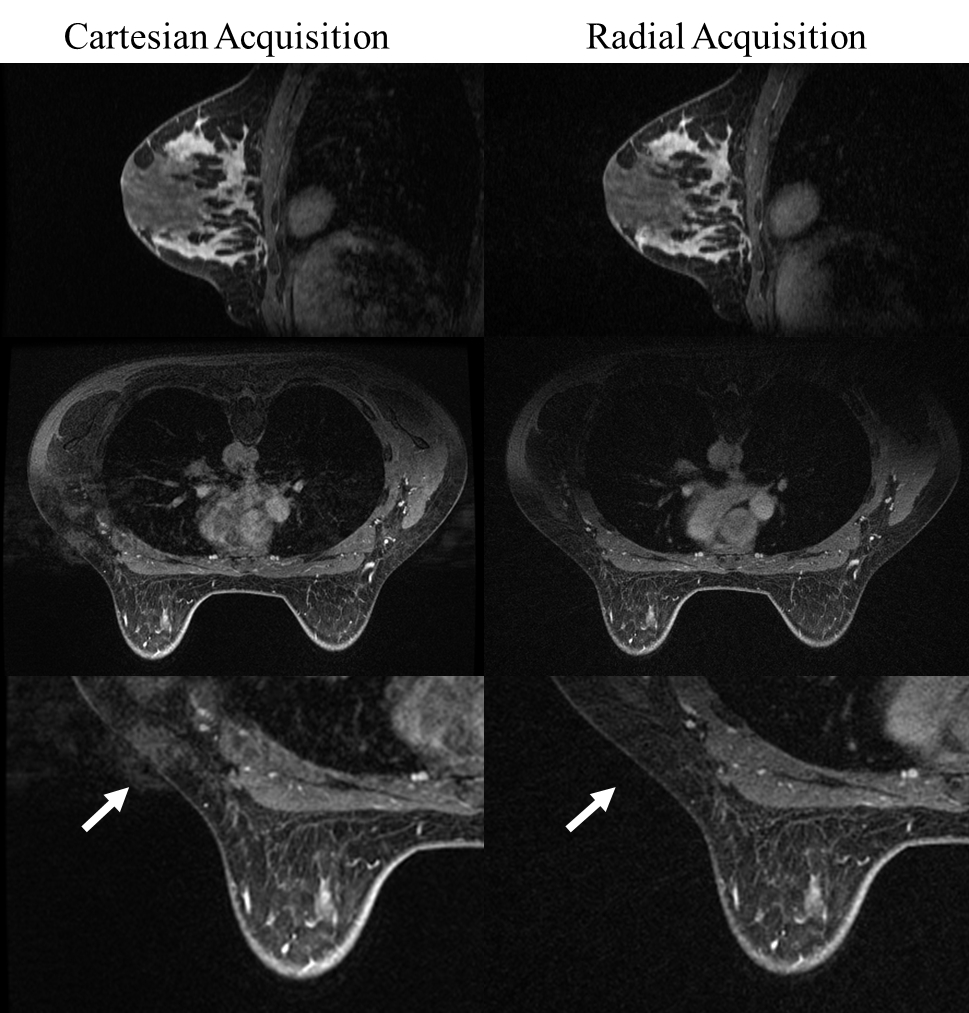
Volunteers: Example results from volunteers are in agreement with the simulation demonstrating reduced artifact in the axilla (Fig. 4-5 arrows). However the level of cardiac ghosting was found to be greater in vivo, likely due to the use of parallel imaging in the Cartesian acquisition.
Discussion
This study compared radial and Cartesian acquisitions in bilateral breast imaging for the reduction of phase ghosting across the axillae. The radial acquisition showed a decrease in artifacts across the axillae without compromise in other regions compared to Cartesian imaging, important for the clinical evaluation of axillary lymph nodes and axillary tail breast tissue. This work relies on the insensitivity to motion for radial imaging due to signal averaging of low spatial frequencies from oversampling of central k-space data. Further, the radial scheme provides great flexibility in the optimization of acquisition time and angular undersampling (6,7). In this work have optimized for higher spatial resolution at the expense of a small increase in undersampling artifact.Conclusion
We demonstrate the promise of a 3D stack-of-stars radial acquisition to reduce phase ghosting artifacts in breast MRI, particularly across the bilateral axillae. This has important clinical applications, as evaluation of the axillary lymph nodes is important in the setting of known breast cancer, a suspicious breast lesion, and post-neoadjuvant therapy.Acknowledgements
We appreciate support from the RSNA, GE Healthcare, NIH/NCI P30 CA014520, and the Department of Radiology at the authors' institution.References
(1) Kim, E. J., Kim, S. H., Kang, B. J., Choi, B. G., Song, B. J., & Choi, J. J. (2014). Diagnostic value of breast MRI for predicting metastatic axillary lymph nodes in breast cancer patients: diffusion-weighted MRI and conventional MRI. Magnetic resonance imaging, 32(10), 1230-1236.
(2) Chandarana, H., Feng, L., Block, T. K., Rosenkrantz, A. B., Lim, R. P., Babb, J. S., ... & Otazo, R. (2013). Free-breathing contrast-enhanced multiphase MRI of the liver using a combination of compressed sensing, parallel imaging, and golden-angle radial sampling. Investigative radiology, 48(1).
(3) Feng, L., Grimm, R., Block, K. T., Chandarana, H., Kim, S., Xu, J., ... & Otazo, R. (2014). Golden-angle radial sparse parallel MRI: Combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI. Magnetic resonance in medicine, 72(3), 707-717.
(4) Yedururi, S., Kang, H. C., Wei, W., Wagner-Bartak, N. A., Marcal, L. P., Stafford, R. J., ... & Szklaruk, J. (2016). Free-breathing radial volumetric interpolated breath-hold examination vs breath-hold cartesian volumetric interpolated breath-hold examination magnetic resonance imaging of the liver at 1.5 T. World Journal of Radiology, 8(7), 707.
(5) Joe, B.N., Wisner, D., Arasu, V.A., Suzukil, S., Deshpande, V.S., Chang, B., Laub, G., Hylton, N.M., (2011). Improved lesion conspicuity on contrast enhanced breast MRI at 3 Tesla using linear vs. radial-centric k-space ordering. International Society for Magnetic Resonance in Medicine (A), 3088.
(6) Chan, R. W., Ramsay, E. A., Cheung, E. Y., & Plewes, D. B. (2012). The influence of radial undersampling schemes on compressed sensing reconstruction in breast MRI. Magnetic resonance in medicine, 67(2), 363-377.
(7) Song, H. K., & Dougherty, L. (2004). Dynamic MRI with projection reconstruction and KWIC processing for simultaneous high spatial and temporal resolution. Magnetic resonance in medicine, 52(4), 815-824.
Figures