4926
Effect of Compressed Sensing Reconstruction Parameter on Ultrafast Dynamic Contrast Enhanced Breast MRI1Department of Radiology, Kyoto University Hospital, Kyoto, Japan, 2Department of Diagnostic Imaging and Nuclear Medicine, Kyoto University Graduate School of Medicine, Kyoto, Japan, 3Kyoto University Hospital, Kyoto, Japan, 4Siemens Healthcare GmbH, Erlangen, Germany, 5Department of Breast Surgery, Kyoto University Graduate School of Medicine, Kyoto, Japan
Synopsis
The aim of this study is to assess the impact of the number of iterations of CS reconstruction on kinetic parameters and the image similarity in DCE-MRI of the breast. Breast examinations include ultrafast DCE-MRI using CS were conducted for 21 patients. The images were reconstructed with different numbers of iterations, and the semi-quantitative and quantitative kinetics parameters were compared. The reconstructed images were evaluated by root mean square error (RMSE) and structural similarity (SSIM) as the quantitative image evaluation. In small number of iteration, the all kinetics parameters were underestimated especially in malignant lesion with hypervascularity.
Purpose
Compressed sensing (CS) has become an important tool for the acceleration of dynamic MRI acquisitions, which is achieved by enabling the reconstruction of subsampled data [1, 2]. CS algorithms can be utilized to improve the temporal/spatial resolution of DCE-MRI, and several works describing retrospective simulations have demonstrated the feasibility of such improvements [3-7]. Many of the reports on DCE-MRI using CS are retrospective studies in which fully sampled raw data sets are down-sampled after data collection. Khalsa showed the reconstruction parameters, regularization parameters affected the time intensity curve [8]. There is possibility that the other reconstruction parameters such as the number of iteration also affect the results and generate the estimation error in tumor enhancing characteristics. The aim of our study is to assess the impact of the number of iterations of CS reconstruction on kinetic parameters and the image quality in DCE-MRI of the breast with prospectively under-sampled CS-accelerated scans.Materials & Methods
Breast examinations including ultrafast DCE-MRI using CS were conducted for 21 patients. All breast MR examinations were performed using a 3T MRI system (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany) and a 18-channel breast coil. Breast DCE-MRI data were acquired using a prototypical non-fat-suppressed 3D volumetric interpolated breath-hold examination (VIBE) sequence with the following imaging parameters: TR=5.04ms, TE=2.46ms, flip angle=15°, slice thickness=2.5mm, matrix size=384x269, CS acceleration=16.5, temporal resolution=3.75sec. DCE-MRI was sequentially acquired for 20 consecutive time points with a total acquisition time of 75sec. After 15sec from scan start, gadoteridol of dose 0.1 mL/kg was injected at 2 mL/s followed by 20 ml saline flush injected at 2 mL/s. CS reconstruction was conducted with the following minimization problem:
$$\phi(x)={\parallel Ax - y \parallel}_2^2+\sum\lambda\parallel Wx \parallel_{1}$$
where A represents the system matrix including under-sampled Fourier transform and coil profiles, x is the reconstructed image, y is the measured k-space data, λ is the regularization parameter, and W is a redundant Haar wavelet transformation. CS reconstruction parameters were as follows:λ=0.002, with an additional weighting of 5 in the temporal dimension and number of iterations for a FISTA optimization using a time-averaged staring point=1, 2, 3, 5, 10, 15, 20, 25, 30, 40, 50. The peak enhancement ratio (PER) of aorta, wash-in slope, PER, initial area under the curve (IAUC) were measured from time intensity curve. Ktrans of the tumor was calculated by Osirix (www.osirix-viewer.com) plug-in software, DCE Tool using population based arterial input function (AIF) method. Root mean square error (RMSE) and structural similarity (SSIM) between the images with 50 iterations and images with other iterations were evaluated as the quantitative image evaluation.
Results
Figure 1 shows the example of the images reconstructed with different numbers of iterations at the different time points. Figure 2 shows the comparison of time intensity curves. The contrast-enhanced effect was highly underestimated in iteration 1.
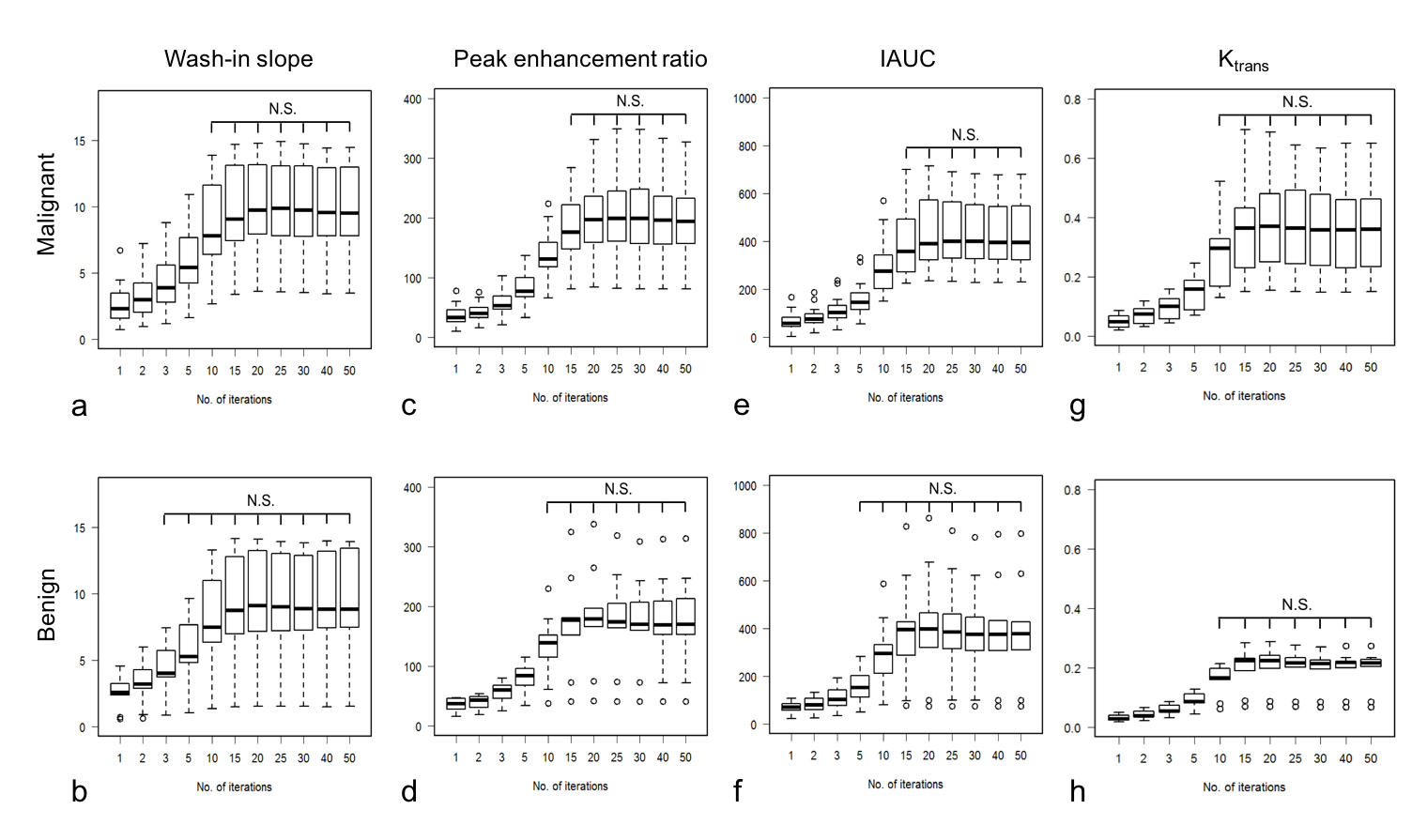
Figure 3 shows the boxplot of wash-in slope, PER, IAUC and Ktrans in malignant and benign lesions for different iterations. In all semi-quantitative parameters, the numbers of iterations which stabled the parameters in malignant lesions were higher than that in benign lesions. At least 15 iterations were needed in semi-quantitative parameters. For Ktrans, there were no significant differences between over 10 iterations and 50 iterations in both malignant and benign lesions.
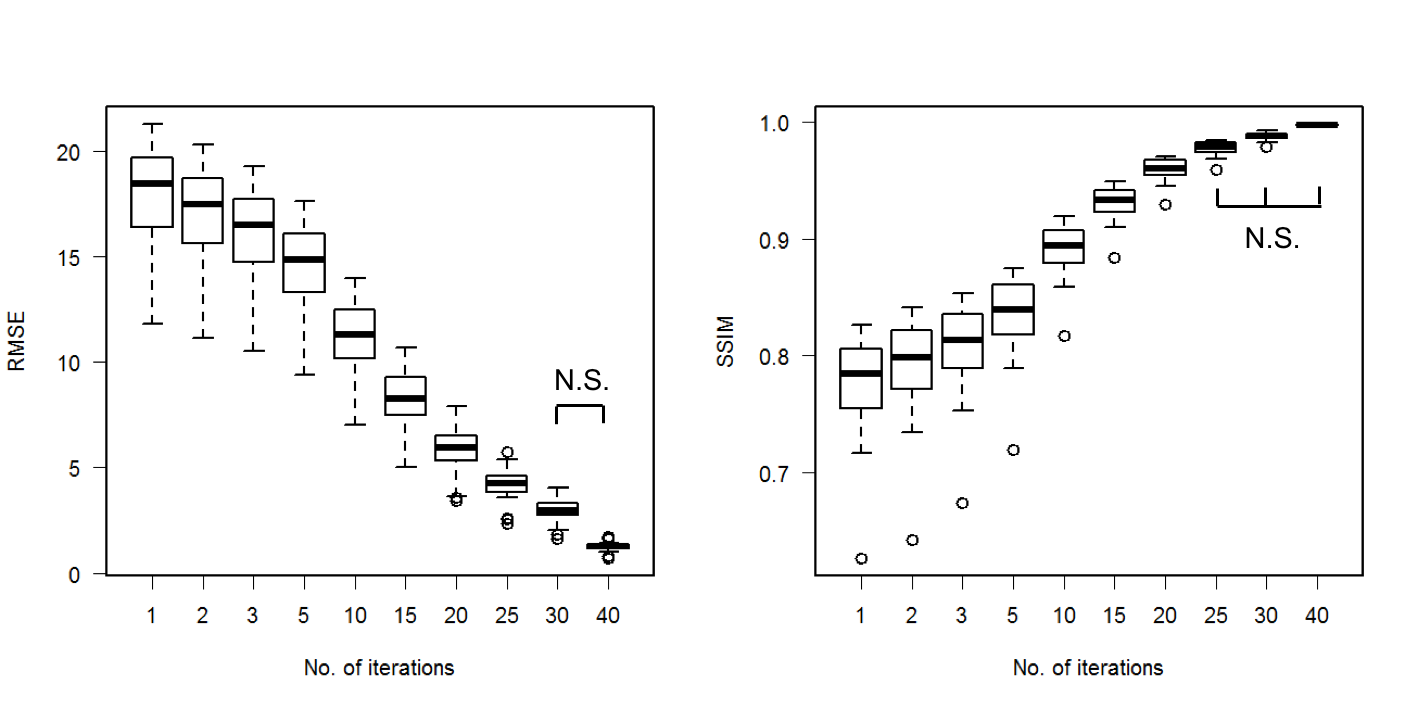
Figure 4 shows RMSE and SSIM between the images using 50 iterations and images using fewer iterations. SSIM values between 50 and 40 iterations were above 0.998, and the images were judged almost equal. There were no significant differences in RMSE between 30 and 40 iterations, and in SSIM between over 25 and 40 iterations.
Discussion and Conclusion
The effect of the number of iterations in an iterative CS reconstruction on kinetic parameters was analyzed for breast DCE-MRI. Increasing the number of iterations requires long reconstruction times, thus an optimization is required for clinical exams. In the quantitative image evaluation, the number of iteration needed 30 for RMSE and 25 for SSIM. On the other hand, the numbers of iterations which stabled the kinetic parameters were higher in malignant because of hyper-vascularity, though it was enough with 15 iterations. In conclusion, kinetics parameters using ultrafast DCE-MRI with CS are affected by the number of iterations especially in malignant regions. However, if the images are reconstructed with an adequate number of iterations, ultrafast DCE-MRI with CS can be a powerful technique having high temporal and spatial resolution.
Acknowledgements
This work was partly supported by Grant-in-Aid for Scientific Researchon Innovative Areas “Initiative for High-Dimensional Data-DrivenScience through Deepening of Sparse Modeling”, MEXT grant numbers25120002, 25120008.References
[1] Lustig M, Donoho D, Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. MRM 2007; 58: 1182-95
[2] Donoho D. Compressed sensing. IEEE Trans Inf Theory 2006; 52: 1289–1306.
[3] Wang H, Miao Y, Zhou K, et al. Feasibility of high temporal resolution breast DCE-MRI using compressed sensing theory. Medical Physics 2010; 37:4971-81
[4] Mann RM, Mus RD, Zelst J, et al. A novel approach to contrast-enhanced breast magnetic resonance imaging for screening: high-resolution ultrafast dynamic imaging. Invest. Radiol 2014; 49: 579–585
[5] Gamper U, Boesiger P, Kozerke S, Compressed sensing in dynamic MRI. MRM 2008; 59: 365–373
[6] Jung H, Sung K, Nayak KS, et al. k-t FOCUSS: A general compressed sensing framework for high resolution dynamic MRI. MRM 2009;61: 103–116
[7] Chan RW, Ramsay EA, Cheung EY, Plewes DB. The influence of radial undersampling schemes on compressed sensing reconstruction in breast MRI. MRM 2012; 67: 363–377.
[8] Khalsa KA, Fessler JA, Resolution properties in regularized dynamic MRI reconstruction, in IEEE Int. Symp. Biomed. Imag. 2007; 456–459.
Figures
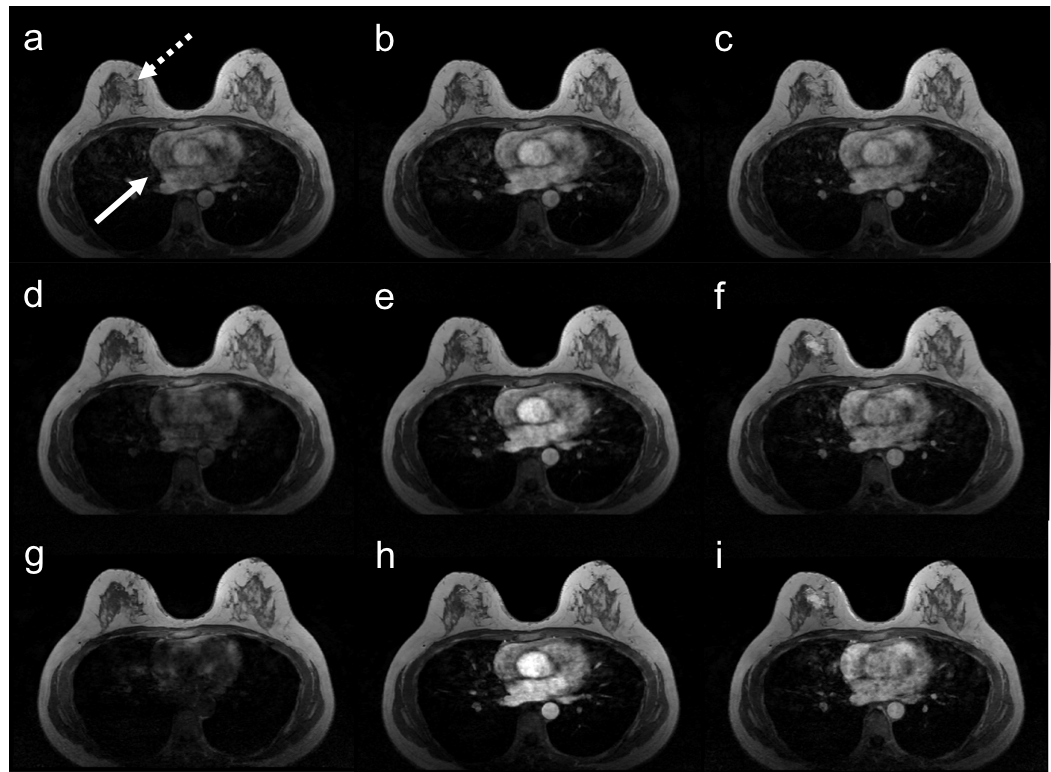
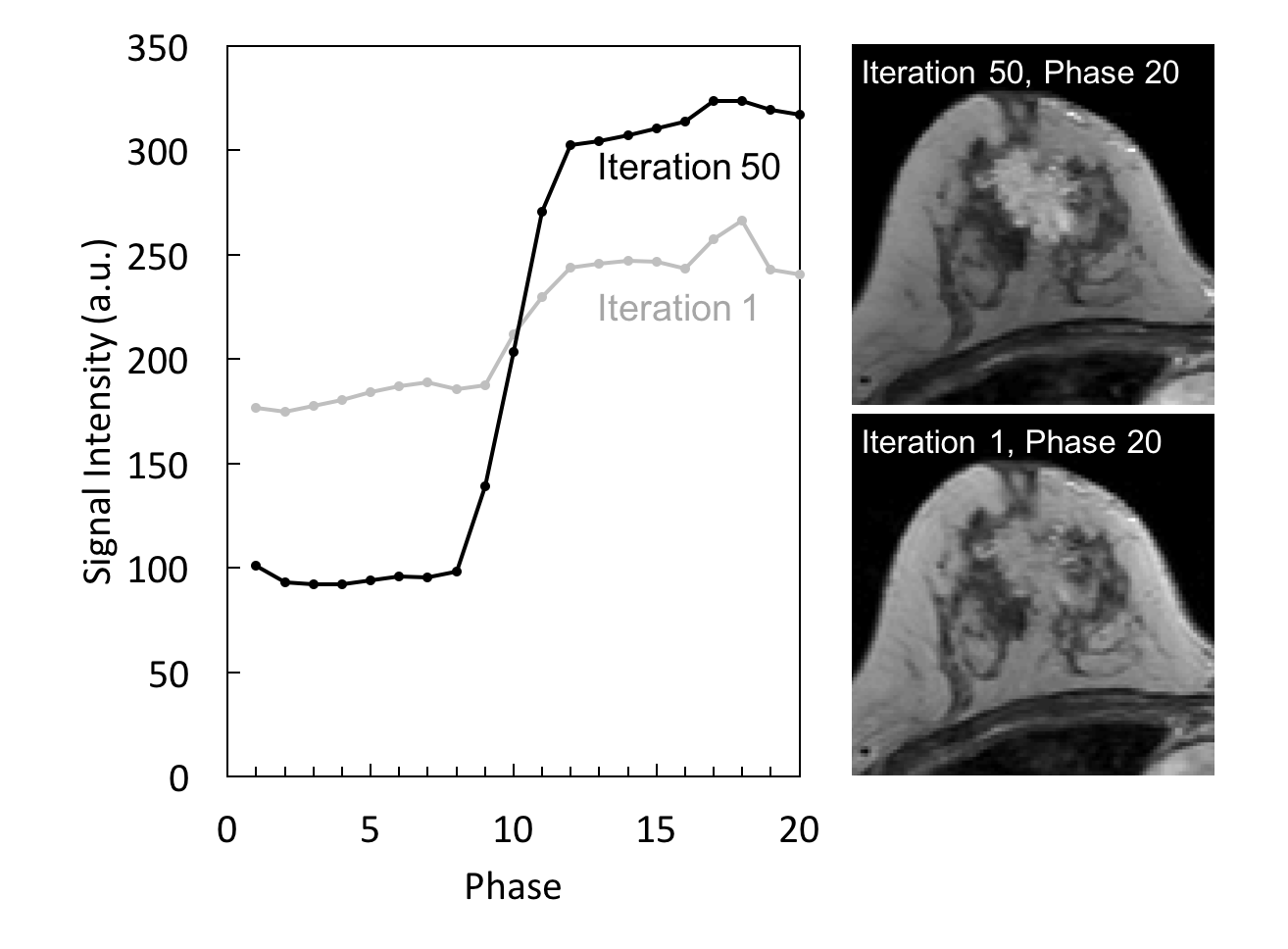
Fig.2: Comparison of time intensity curves of the tumor with iteration 1 and 50. The contrast enhanced effect was highly underestimated in iteration 1.